Public Health Report: COVID-19 Infection Rates in US and China
VerifiedAdded on 2023/01/03
|14
|4555
|40
Report
AI Summary
This report presents a comparative analysis of COVID-19 infection rates in the United States and China, focusing on government regulations, screening criteria, and testing methodologies. The study employed document analysis to examine the differences and similarities in the countries' responses to the pandemic, considering factors such as geographic area, resources, and the timing of outbreaks. The research delves into screening protocols, confirmation of COVID-19 cases through PCR testing, and government-issued community guidelines. The findings reveal variations in screening criteria, such as the inclusion of travel history and pneumonia as indicators, as well as differences in testing approaches. The report also explores the relationship between regulatory deadlines and infection rates, aiming to identify best practices and inform the development of future COVID-19 responses. The data collection involved examining government documents and guidelines from March to May 2020, with data analysis conducted through thematic review and content analysis. The study highlights the importance of understanding how different countries have managed the pandemic and the role of healthcare structures in shaping COVID-19 responses. The report concludes with a discussion on the need for global research efforts to interpret and address the conditions of global well-being.
HEALTHCARE
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Background of the topic:.................................................................................................................3
1. Introduction..................................................................................................................................3
2. Objective......................................................................................................................................4
3. Methods.......................................................................................................................................5
3.1 Research Design....................................................................................................................5
3.2 Country selection...................................................................................................................5
4. Data collection.............................................................................................................................6
4.1 Data analysis..........................................................................................................................6
5. Results..........................................................................................................................................7
5.1 Evaluation and testing............................................................................................................7
5.1.1 Screening criteria............................................................................................................7
5.1.2 Confirmation of COVID 19............................................................................................9
5.2 Infection control.....................................................................................................................9
5.2.1 General outpatient guidance...........................................................................................9
5.2.2 Triage Protocols............................................................................................................10
5.3 Cost support.........................................................................................................................11
6. Community guidelines...............................................................................................................11
6.1 Prevent getting sick..............................................................................................................11
7. Conclusion.................................................................................................................................13
References......................................................................................................................................14
Background of the topic:.................................................................................................................3
1. Introduction..................................................................................................................................3
2. Objective......................................................................................................................................4
3. Methods.......................................................................................................................................5
3.1 Research Design....................................................................................................................5
3.2 Country selection...................................................................................................................5
4. Data collection.............................................................................................................................6
4.1 Data analysis..........................................................................................................................6
5. Results..........................................................................................................................................7
5.1 Evaluation and testing............................................................................................................7
5.1.1 Screening criteria............................................................................................................7
5.1.2 Confirmation of COVID 19............................................................................................9
5.2 Infection control.....................................................................................................................9
5.2.1 General outpatient guidance...........................................................................................9
5.2.2 Triage Protocols............................................................................................................10
5.3 Cost support.........................................................................................................................11
6. Community guidelines...............................................................................................................11
6.1 Prevent getting sick..............................................................................................................11
7. Conclusion.................................................................................................................................13
References......................................................................................................................................14
Topic: Comparative report of rate of COVID-
19 infections in US and China
Background of the topic:
In late January, a total emergency called COVID-19 was declared by the WHO a public health
emergency of international concern. In half a month, the program reached pandemic levels,
affecting more than 100 countries. The regulation and control of COVID-19 has been an
important issue on both a public and global scale due to emotional expansion in confirmed cases
around the world. Government regulations provide essential funding for networks, as they
monitor residents in the best possible way to protect themselves from COVID-19; however, they
also provide basic guidance to strategy representatives and medical care experts on how to best
move to reduce COVID-19 transmission. The point was to recognize the differences and
similarities between the rules of the network framework and the medical services provided by the
governments of two specific countries (US and China) and to examine the connection between
the deadlines in case management and the leadership / level of COVID-19 cases.
1. Introduction
The new COVID-19 program has raised serious concerns about the increase in mortality on the
planet. The main COVID-19 program was planned in the city of Wuhan, the capital of China's
Hubei region, at the end of December 2019 (Guan et etal., 2020). Two months after the fact, on
11 March 2020, the World Health Organization (WHO) assigned a pandemic to the COVID-19
incident and handed the regulations to the COVID-19 case to the office and council of the
shundn network. Across the world, approximately 3,506,577 fixed instances of COVID-19 have
been reported, this data added with more than 247,467 passages (Johns Hopkins University, May
3, 2020) (COVID-19 Dashboard from the Center for Systems Science and Engineering (CSSE))
at the Johns Hopkins University (JHU), 2020). The rapid spread of the disease highlights the
connected global well-being and the need to invest resources in global research efforts to study,
interpret and address the conditions of global well-being.
19 infections in US and China
Background of the topic:
In late January, a total emergency called COVID-19 was declared by the WHO a public health
emergency of international concern. In half a month, the program reached pandemic levels,
affecting more than 100 countries. The regulation and control of COVID-19 has been an
important issue on both a public and global scale due to emotional expansion in confirmed cases
around the world. Government regulations provide essential funding for networks, as they
monitor residents in the best possible way to protect themselves from COVID-19; however, they
also provide basic guidance to strategy representatives and medical care experts on how to best
move to reduce COVID-19 transmission. The point was to recognize the differences and
similarities between the rules of the network framework and the medical services provided by the
governments of two specific countries (US and China) and to examine the connection between
the deadlines in case management and the leadership / level of COVID-19 cases.
1. Introduction
The new COVID-19 program has raised serious concerns about the increase in mortality on the
planet. The main COVID-19 program was planned in the city of Wuhan, the capital of China's
Hubei region, at the end of December 2019 (Guan et etal., 2020). Two months after the fact, on
11 March 2020, the World Health Organization (WHO) assigned a pandemic to the COVID-19
incident and handed the regulations to the COVID-19 case to the office and council of the
shundn network. Across the world, approximately 3,506,577 fixed instances of COVID-19 have
been reported, this data added with more than 247,467 passages (Johns Hopkins University, May
3, 2020) (COVID-19 Dashboard from the Center for Systems Science and Engineering (CSSE))
at the Johns Hopkins University (JHU), 2020). The rapid spread of the disease highlights the
connected global well-being and the need to invest resources in global research efforts to study,
interpret and address the conditions of global well-being.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

At the stage where China's main COVID-19 program was described, the Chinese government
introduced rules recommending keeping a social remote plantation open, living at home, and
freeing corrupt populations to keep the pandemic at bay. After a month, South Korea was
dispatched with the COVID-19 program. Starting activity by the two governments was solid in
attempting to forestall the spread of the infection, including both thorough testing for the illness
and ensuing reports. The COVID-19 reaction in China and South Korea stretched out the model
to different nations where COVID-19 was simply starting to develop. While it was not
satisfactory whether the exacting measures taken by China and South Korea could be changed or
modified by various nations, the multifaceted viewpoint of the infection all in all was
additionally supported by research on clinical administrations and organization input from
legislatures of various nations.
It reflects on factors which differ each country from each other such as capacities, risks, threats,
political and socio-economic challenges; additional to this various health care factor also make
difference on the way COVID impacts different countries. In any case, it is also crucial to look at
how different countries tended to deal with the Covid pandemic. Next, the rules of two specific
countries were looked at to examine the administration, frequency, and frequency of COVID-19
cases. Additionally, we looked at the relationship between regulatory deadlines and regulatory
frequency cycles of various countries.
2. Objective
The objective was to analyze government regulations on COVID-19 with two specific countries
(United States (US) and China). This included general population rules and the rules of medical
care specialists (clinical groups). The key point was to identify the differences and differences
between the national rules of nations and the rules of medical services and also to examine the
connection between the dates of issuance of the rules and the contamination / occurrence in
COVID-19 cases. This is huge because it looked at how different countries have responded to
COVID-19 and identified best practices. Similarly, this approach will allow us to see how the
medical services structure and boundaries of the strategy shape COVID-19 reactions and share
this data to inform COVID-19 reactions development.
introduced rules recommending keeping a social remote plantation open, living at home, and
freeing corrupt populations to keep the pandemic at bay. After a month, South Korea was
dispatched with the COVID-19 program. Starting activity by the two governments was solid in
attempting to forestall the spread of the infection, including both thorough testing for the illness
and ensuing reports. The COVID-19 reaction in China and South Korea stretched out the model
to different nations where COVID-19 was simply starting to develop. While it was not
satisfactory whether the exacting measures taken by China and South Korea could be changed or
modified by various nations, the multifaceted viewpoint of the infection all in all was
additionally supported by research on clinical administrations and organization input from
legislatures of various nations.
It reflects on factors which differ each country from each other such as capacities, risks, threats,
political and socio-economic challenges; additional to this various health care factor also make
difference on the way COVID impacts different countries. In any case, it is also crucial to look at
how different countries tended to deal with the Covid pandemic. Next, the rules of two specific
countries were looked at to examine the administration, frequency, and frequency of COVID-19
cases. Additionally, we looked at the relationship between regulatory deadlines and regulatory
frequency cycles of various countries.
2. Objective
The objective was to analyze government regulations on COVID-19 with two specific countries
(United States (US) and China). This included general population rules and the rules of medical
care specialists (clinical groups). The key point was to identify the differences and differences
between the national rules of nations and the rules of medical services and also to examine the
connection between the dates of issuance of the rules and the contamination / occurrence in
COVID-19 cases. This is huge because it looked at how different countries have responded to
COVID-19 and identified best practices. Similarly, this approach will allow us to see how the
medical services structure and boundaries of the strategy shape COVID-19 reactions and share
this data to inform COVID-19 reactions development.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
3. Methods
3.1 Research Design
The study has used document analysis, a standard thematic review strategy for letter evaluation
and strategy analysis, to examine the differences and similarities between the six-country
government COVID-19 regulations (Bowen, 2009). Accompanying progress for the experiment
was recalled: (I) build the archive observation rules, (ii) collect reports, (iii) examine key areas,
(iv) to "Code the register, (v) check and (vi) review (Bowen, 2009). In this approach, reps are the
essential means to validate and analyze information.
3.2 Country selection
The Covid is an overall pandemic that legitimizes an expansive general visibility from nations
that contrast in a couple of levels (e.g., Geographic Area, Benefit and Currency Resources,
COVID-19 Distribution and Response Rate ) to expand their openness and blend while
inspecting the degree of the Framework Regulations for Network and Medical Services
identified with COVID-19. During the decision of the two nations, thought was given to: 1) the
start and pinnacle season of COVID-19, 2) the closeness of China, where the spread of COVID-
19 started, 3) populace size, 4) province of GDP and 5 ) a bilingual expert's declaration in the
field of general prosperity. For instance, the fundamental fire of COVID-19 happened in China
in December 2019. The limits proceeded in a few nations, for example, the United States and the
UK in a brief timeframe in January and February 2020. At long last, in March 2020 , Brazil and
Haiti have seen an expansion in the recurrence and sections of contamination. In April 2020,
China and South Korea were at the phase of pandemic recuperation, while COVID-19 outflows
have gone up in nations, for example, the United States, the United Kingdom, Haiti and Brazil.
Land contrasts in the chose nations appeared as close geology as China (Korea), the biggest
populace in North America (the United States), the biggest populace in South America (Brazil),
and island nations with huge detachments from China (Haiti and the United Kingdom). Also, the
populace sizes of the nations were inconsistent recognized by the possibility and far reaching
dispersal of information with respect to COVID-19 guidelines (Cantini, 2020). Furthermore, the
GDP of the nations discussed the assets, abilities and techniques utilized by COVID-19. For
instance, close to the start of the COVID-19 spread in the UK and Haiti, the two countries had
close to no available resources for COVID testing. With Haiti's fragile clinical consideration
3.1 Research Design
The study has used document analysis, a standard thematic review strategy for letter evaluation
and strategy analysis, to examine the differences and similarities between the six-country
government COVID-19 regulations (Bowen, 2009). Accompanying progress for the experiment
was recalled: (I) build the archive observation rules, (ii) collect reports, (iii) examine key areas,
(iv) to "Code the register, (v) check and (vi) review (Bowen, 2009). In this approach, reps are the
essential means to validate and analyze information.
3.2 Country selection
The Covid is an overall pandemic that legitimizes an expansive general visibility from nations
that contrast in a couple of levels (e.g., Geographic Area, Benefit and Currency Resources,
COVID-19 Distribution and Response Rate ) to expand their openness and blend while
inspecting the degree of the Framework Regulations for Network and Medical Services
identified with COVID-19. During the decision of the two nations, thought was given to: 1) the
start and pinnacle season of COVID-19, 2) the closeness of China, where the spread of COVID-
19 started, 3) populace size, 4) province of GDP and 5 ) a bilingual expert's declaration in the
field of general prosperity. For instance, the fundamental fire of COVID-19 happened in China
in December 2019. The limits proceeded in a few nations, for example, the United States and the
UK in a brief timeframe in January and February 2020. At long last, in March 2020 , Brazil and
Haiti have seen an expansion in the recurrence and sections of contamination. In April 2020,
China and South Korea were at the phase of pandemic recuperation, while COVID-19 outflows
have gone up in nations, for example, the United States, the United Kingdom, Haiti and Brazil.
Land contrasts in the chose nations appeared as close geology as China (Korea), the biggest
populace in North America (the United States), the biggest populace in South America (Brazil),
and island nations with huge detachments from China (Haiti and the United Kingdom). Also, the
populace sizes of the nations were inconsistent recognized by the possibility and far reaching
dispersal of information with respect to COVID-19 guidelines (Cantini, 2020). Furthermore, the
GDP of the nations discussed the assets, abilities and techniques utilized by COVID-19. For
instance, close to the start of the COVID-19 spread in the UK and Haiti, the two countries had
close to no available resources for COVID testing. With Haiti's fragile clinical consideration

system, Haiti didn't have the establishment to fight the spread of the contamination, advocating
money related assistance from various countries.
4. Data collection
To guide the decision on a relationship between the delegates, an image was created in which
data was essential for each topic. Each table for every nation was dissected to decide the degree
to which the report gave reactions at any phase of one of the pre-distinguished themes (for
example study zones). The gathering examined government destinations step by step for around
a month and a half from March 2020 to May 2020 to acquire information from government
guidelines and to decide whether new records were delivered or whether to refresh the old
principles. A sum of 55 records (for example government guidelines, flyers, sees, pages) was
inspected to eliminate the data (10 for the US and 3 for China). Interpretations of the COVID-19
all out populace rules and government assistance advancement materials pertinent to each pre-
distinguished subject were rehashed verbatim in their particular language and added to a
predominant bookkeeping sheet. Verbatim messages written in a language other than English
(Portuguese, Chinese, Korean and Haitian Creole/French) demonstrated English by the
experimental group bilinguals and added to the fundamental bookkeeping page more to think
about the examination and investigation of the Collected information. Text understanding has
generally neglected to keep up the normal importance of clinical consideration language rather
than the social inner mind, along these lines, a conventional translation of the translation (for
example forward and turn around translation).
4.1 Data analysis
The main areas of the test were explained in the code book, which provided a collection of codes
(e.g. topics and subtopics) and included six essential categories: the code, a precise explanation,
a complete explanation, and the rules for when to use or do not use code and examples of code.
Unfortunately, the code book helped the review body determine the impact of the arguments and
clarified what should be looked at within the content of the rules. The effectiveness and clarity of
the codes were used as a tool to estimate the range of answers to analyze questions. Examination
of information involved the evaluation and integration of writings from the rules, which were
then co-ordinated into meaningful topics and subclasses through material analysis (Hsieh and
money related assistance from various countries.
4. Data collection
To guide the decision on a relationship between the delegates, an image was created in which
data was essential for each topic. Each table for every nation was dissected to decide the degree
to which the report gave reactions at any phase of one of the pre-distinguished themes (for
example study zones). The gathering examined government destinations step by step for around
a month and a half from March 2020 to May 2020 to acquire information from government
guidelines and to decide whether new records were delivered or whether to refresh the old
principles. A sum of 55 records (for example government guidelines, flyers, sees, pages) was
inspected to eliminate the data (10 for the US and 3 for China). Interpretations of the COVID-19
all out populace rules and government assistance advancement materials pertinent to each pre-
distinguished subject were rehashed verbatim in their particular language and added to a
predominant bookkeeping sheet. Verbatim messages written in a language other than English
(Portuguese, Chinese, Korean and Haitian Creole/French) demonstrated English by the
experimental group bilinguals and added to the fundamental bookkeeping page more to think
about the examination and investigation of the Collected information. Text understanding has
generally neglected to keep up the normal importance of clinical consideration language rather
than the social inner mind, along these lines, a conventional translation of the translation (for
example forward and turn around translation).
4.1 Data analysis
The main areas of the test were explained in the code book, which provided a collection of codes
(e.g. topics and subtopics) and included six essential categories: the code, a precise explanation,
a complete explanation, and the rules for when to use or do not use code and examples of code.
Unfortunately, the code book helped the review body determine the impact of the arguments and
clarified what should be looked at within the content of the rules. The effectiveness and clarity of
the codes were used as a tool to estimate the range of answers to analyze questions. Examination
of information involved the evaluation and integration of writings from the rules, which were
then co-ordinated into meaningful topics and subclasses through material analysis (Hsieh and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Shannon, 2005). Content analysis within the review group was encouraged through online
meetings, which were beneficial and removed geographical barriers. The experts looked at
information for coding projects (e.g. comparison, differences, recycling) in different countries
against their administrative rules for the total population and medical services specialists. All
rule writing has been matched to the previous arguments (subtraction codes). During the iterative
study measurement of materials, new arguments (inductive codes) also emerged. By the time the
contradiction occurred when the information was analyzed, the scouting group either went back
or the programmer needed to seek the advice of another colleague for control and interpretation
(Hsieh and Shannon, 2005). The original and prior information was downloaded from the Johns
Hopkins University Center for Systems Science and Engineering (Cantini, 2020). Tableau, a
well-known big data analytics website, was used to clean up and redesign data for public sharing.
The data was then converted into excellent files and used to generate figures (Coronavirus Data
Hub FAQ: What you should know about our COVID-19 dataset, 2020).
5. Results
5.1 Evaluation and testing
5.1.1 Screening criteria
When contrasting the distinctive government rules on screening for signs and manifestations in
theoretical COVID-19 cases, all nations have recorded respiratory results as the norm and
generally significant: Brazil as help - even fever with a line. Shockingly, the US and the UK
have not recorded travel history as a model. We additionally found that the United States and
Brazil don't recommend pneumonia as a screening rule, albeit South Korea, the United Kingdom
and Haiti have affirmed an obscure illustration of seizures, a clinical or radioactive finding of
pneumonia and bronchopneumonia. A one of a kind declaration that the makers have noted is
that China and the UK have chosen to recognize associated cases with COVID-19 inside the
crisis facility through radiological affirmation by means of chest X-beams and tomography.
Chest figured tomography (CT) or expansions in lymphocytes. Haiti, as of April 20, 2020, has
expanded the screening rate from '' fever is more articulated than 38 ° C over the most recent 10
days '' to '' anybody with a fever more articulated or equivalent to 38 ° C (see the extra table 3).
"Haitian screening models likewise included body spreads, startling changes in taste (ageusia) or
meetings, which were beneficial and removed geographical barriers. The experts looked at
information for coding projects (e.g. comparison, differences, recycling) in different countries
against their administrative rules for the total population and medical services specialists. All
rule writing has been matched to the previous arguments (subtraction codes). During the iterative
study measurement of materials, new arguments (inductive codes) also emerged. By the time the
contradiction occurred when the information was analyzed, the scouting group either went back
or the programmer needed to seek the advice of another colleague for control and interpretation
(Hsieh and Shannon, 2005). The original and prior information was downloaded from the Johns
Hopkins University Center for Systems Science and Engineering (Cantini, 2020). Tableau, a
well-known big data analytics website, was used to clean up and redesign data for public sharing.
The data was then converted into excellent files and used to generate figures (Coronavirus Data
Hub FAQ: What you should know about our COVID-19 dataset, 2020).
5. Results
5.1 Evaluation and testing
5.1.1 Screening criteria
When contrasting the distinctive government rules on screening for signs and manifestations in
theoretical COVID-19 cases, all nations have recorded respiratory results as the norm and
generally significant: Brazil as help - even fever with a line. Shockingly, the US and the UK
have not recorded travel history as a model. We additionally found that the United States and
Brazil don't recommend pneumonia as a screening rule, albeit South Korea, the United Kingdom
and Haiti have affirmed an obscure illustration of seizures, a clinical or radioactive finding of
pneumonia and bronchopneumonia. A one of a kind declaration that the makers have noted is
that China and the UK have chosen to recognize associated cases with COVID-19 inside the
crisis facility through radiological affirmation by means of chest X-beams and tomography.
Chest figured tomography (CT) or expansions in lymphocytes. Haiti, as of April 20, 2020, has
expanded the screening rate from '' fever is more articulated than 38 ° C over the most recent 10
days '' to '' anybody with a fever more articulated or equivalent to 38 ° C (see the extra table 3).
"Haitian screening models likewise included body spreads, startling changes in taste (ageusia) or
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

smell (anosmia), occasions to collaborate with an individual with demonstrated clinical
consideration has COVID-19 or lives in a high-hazard region while meeting COVID19 viable
introductions.
5.1.2 Confirmation of COVID 19
Each one of the two countries performed consistent PCR to certify COVID-19 cases. Some
intriguing kinds of verifying lab tests were by methods for quality sequencing in China, and
serological evaluation in the US. The US, regardless, made the separation that an individual who
met those standards was seen as a conceivable case. The US furthermore portrayed likely cases
as an individual assembling the speculative lab verification and either the clinical measures or
the epidemiological evidence. Finally, an individual could be seen as a feasible case by the US if
their basic records, as in their passing validation, shown the individual kicked the basin of causes
related to COVID-19, regardless of not having a confirmed exploration office test result.
5.2 Infection control
5.2.1 General outpatient guidance
Outpatients are patients outside the emergency clinic who need periodic clinical examination due
to various diseases (epilepsy, malignant tumors, HIV / AIDS, etc.) in different countries, patients
outpatients requiring treatment are medically non-COVID-19 infections coordinated to a Public
Relief Hospital for improvement or to see a specialist. These outpatients were carefully separated
from patients with no respiratory signal.
In the United States, outpatients have been advised to visit during their stay and have been
diagnosed with signs of respiratory contamination. Chinese patients could, then again, contract
by phone or online and could end their stay at the medical clinic as long as the patient met
qualified professional and tried not to use the trauma center (ER) or fever facilities where
COVID-19 patients were treated. The United States updated its rules on April 13, 2020,
encouraging medical care offices to make options for emergencies and intimate and personal
visits, and training patients to use product face masks while not giving they pay a lot of attention
to side effects during the section of his medical support office. However, the rule did not specify
which options were achieved.
consideration has COVID-19 or lives in a high-hazard region while meeting COVID19 viable
introductions.
5.1.2 Confirmation of COVID 19
Each one of the two countries performed consistent PCR to certify COVID-19 cases. Some
intriguing kinds of verifying lab tests were by methods for quality sequencing in China, and
serological evaluation in the US. The US, regardless, made the separation that an individual who
met those standards was seen as a conceivable case. The US furthermore portrayed likely cases
as an individual assembling the speculative lab verification and either the clinical measures or
the epidemiological evidence. Finally, an individual could be seen as a feasible case by the US if
their basic records, as in their passing validation, shown the individual kicked the basin of causes
related to COVID-19, regardless of not having a confirmed exploration office test result.
5.2 Infection control
5.2.1 General outpatient guidance
Outpatients are patients outside the emergency clinic who need periodic clinical examination due
to various diseases (epilepsy, malignant tumors, HIV / AIDS, etc.) in different countries, patients
outpatients requiring treatment are medically non-COVID-19 infections coordinated to a Public
Relief Hospital for improvement or to see a specialist. These outpatients were carefully separated
from patients with no respiratory signal.
In the United States, outpatients have been advised to visit during their stay and have been
diagnosed with signs of respiratory contamination. Chinese patients could, then again, contract
by phone or online and could end their stay at the medical clinic as long as the patient met
qualified professional and tried not to use the trauma center (ER) or fever facilities where
COVID-19 patients were treated. The United States updated its rules on April 13, 2020,
encouraging medical care offices to make options for emergencies and intimate and personal
visits, and training patients to use product face masks while not giving they pay a lot of attention
to side effects during the section of his medical support office. However, the rule did not specify
which options were achieved.
5.2.2 Triage Protocols
Hospital admission criteria
All countries’ hospital preferences were presented based on the defense building. Chinese rule
has not established the certification standards for emergency clinics. The United States has
recommended hospitalization for people with severe symptoms: septic shock, sepsis, pneumonia,
hypoxemic respiratory distress, severe respiratory pain disorder (ARDS), and cardiomyopathy,
and so on, clinical manifestations of pneumonia or radioactive diagnosis with high susceptibility
to COVID-19, with symptoms similar to ARDS or influenza for hospitalization. Positive
asymptomatic COVID-19 or those with moderate symptoms were evacuated by the Live
Treatment Center, an office that observed the side effects of the double day and transferred help
to the clinic in case the population was negatively affected.
5.2.2.1 Healthcare triage isolations
Each of the two countries has established a non-segregated area for screening and follow-up
work for patients who aim to disconnect speculative issues. The United States has encouraged
medical services offices to place speculative cases in well-ventilated areas that allow for
adequate space between patients. China was coordinating its medical care offices at various
levels of care, as evidenced by the absence or presence of respiratory manifestations. More
clearly, China has declared emergency separation zones in those for patients with confirmed,
suspected or non-COVID-19.
5.2.2.2 Visitor’s access to healthcare facilities
In China, guests were disallowed from getting to medical services offices, though the US made
no suggestions with respect to guest access, by April the US Center for Disease Control and
Prevention (CDC) instructed clinics to restrict the number concerning guests permitted.
In addition to Chinese regulations, each country has avoided potential dangers to guests by
establishing norms for guests regarding appropriate personal protective equipment (PPE) and
hygiene. Despite the fact that U.S. CDC regulations were less restrictive than different countries
regarding guest barriers, U.S. regulations recommended effective guest screening for fever and
COVID-19 section symptoms of the medical services offices. Given the unavailability of
COVID-19 side effects, the rules required the guest to enter the office. Basically, Brazil
Hospital admission criteria
All countries’ hospital preferences were presented based on the defense building. Chinese rule
has not established the certification standards for emergency clinics. The United States has
recommended hospitalization for people with severe symptoms: septic shock, sepsis, pneumonia,
hypoxemic respiratory distress, severe respiratory pain disorder (ARDS), and cardiomyopathy,
and so on, clinical manifestations of pneumonia or radioactive diagnosis with high susceptibility
to COVID-19, with symptoms similar to ARDS or influenza for hospitalization. Positive
asymptomatic COVID-19 or those with moderate symptoms were evacuated by the Live
Treatment Center, an office that observed the side effects of the double day and transferred help
to the clinic in case the population was negatively affected.
5.2.2.1 Healthcare triage isolations
Each of the two countries has established a non-segregated area for screening and follow-up
work for patients who aim to disconnect speculative issues. The United States has encouraged
medical services offices to place speculative cases in well-ventilated areas that allow for
adequate space between patients. China was coordinating its medical care offices at various
levels of care, as evidenced by the absence or presence of respiratory manifestations. More
clearly, China has declared emergency separation zones in those for patients with confirmed,
suspected or non-COVID-19.
5.2.2.2 Visitor’s access to healthcare facilities
In China, guests were disallowed from getting to medical services offices, though the US made
no suggestions with respect to guest access, by April the US Center for Disease Control and
Prevention (CDC) instructed clinics to restrict the number concerning guests permitted.
In addition to Chinese regulations, each country has avoided potential dangers to guests by
establishing norms for guests regarding appropriate personal protective equipment (PPE) and
hygiene. Despite the fact that U.S. CDC regulations were less restrictive than different countries
regarding guest barriers, U.S. regulations recommended effective guest screening for fever and
COVID-19 section symptoms of the medical services offices. Given the unavailability of
COVID-19 side effects, the rules required the guest to enter the office. Basically, Brazil
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
recommended avoiding guest corridors with breath-taking displays. Similarly, the U.S. CDC and
the Brazilian government have issued visual warnings to encourage guests to wash their hands
most of the time, restricting guests to weaker patients (e.g. oncology and transfer bags.), allows
video call applications to be used instead of personal visits and recommendations for guests to
leave the patient during vaporized production strategies or other examples of assortment
procedures. Eventually, the United States instructed guests to visit the patient-only room, with no
separate areas in the office.
5.3 Cost support
Financial assistance for testing and treatment was provided mainly or entirely by a UK public
authority. While the United States and the World Bank's governing body were affiliated with
some global and private associations, they gave them the money to take care of the costs of the
country's COVID-19 response. In China, a person's clinical cost was funded under the
neighborhood implementation strategy where the patient was associated with COVID-19. In any
case, when the patient was diagnosed with COVID-19 contamination, the clinical cost was
funded by specialists. The cost of the center visit and testing made U.S. residents widely aware
of the protection status, under the Family Coronavirus Response Act, which required private and
governmental protection to pay for the Food and Drug Administration (FDA) - proof supported
and free trial for the uninsured. The extent to which COVID-19 treatment was covered was
across insurance groups.
6. Community guidelines
6.1 Prevent getting sick
Most of the recommendations for the network on disease prevention were compared to the six
comparable countries. To explore major differences, the subdivisions were coordinated with
specific tasks (e.g. total time to wash hands, cover hacks and sniffles, suggestions for covering
the face, and so on)
In general, recommendations for facial coverage changed during the pandemic, but China has
suggested that the use of open face masks takes the first place of onset of the pandemic,
regardless of whether the individual has swept away. The U.S. did not initially recommend
the Brazilian government have issued visual warnings to encourage guests to wash their hands
most of the time, restricting guests to weaker patients (e.g. oncology and transfer bags.), allows
video call applications to be used instead of personal visits and recommendations for guests to
leave the patient during vaporized production strategies or other examples of assortment
procedures. Eventually, the United States instructed guests to visit the patient-only room, with no
separate areas in the office.
5.3 Cost support
Financial assistance for testing and treatment was provided mainly or entirely by a UK public
authority. While the United States and the World Bank's governing body were affiliated with
some global and private associations, they gave them the money to take care of the costs of the
country's COVID-19 response. In China, a person's clinical cost was funded under the
neighborhood implementation strategy where the patient was associated with COVID-19. In any
case, when the patient was diagnosed with COVID-19 contamination, the clinical cost was
funded by specialists. The cost of the center visit and testing made U.S. residents widely aware
of the protection status, under the Family Coronavirus Response Act, which required private and
governmental protection to pay for the Food and Drug Administration (FDA) - proof supported
and free trial for the uninsured. The extent to which COVID-19 treatment was covered was
across insurance groups.
6. Community guidelines
6.1 Prevent getting sick
Most of the recommendations for the network on disease prevention were compared to the six
comparable countries. To explore major differences, the subdivisions were coordinated with
specific tasks (e.g. total time to wash hands, cover hacks and sniffles, suggestions for covering
the face, and so on)
In general, recommendations for facial coverage changed during the pandemic, but China has
suggested that the use of open face masks takes the first place of onset of the pandemic,
regardless of whether the individual has swept away. The U.S. did not initially recommend
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
wearing face cover, despite the updated rules by the U.S. CDC on April 4, 2020, to show that
everyone is individual, regardless of whether they have been wiped off or not, they should wear
linen clothes in daylight. However, a clinical face recommendation has not yet been proposed for
the network, as they had to be retained for medical care staff due to shortages.
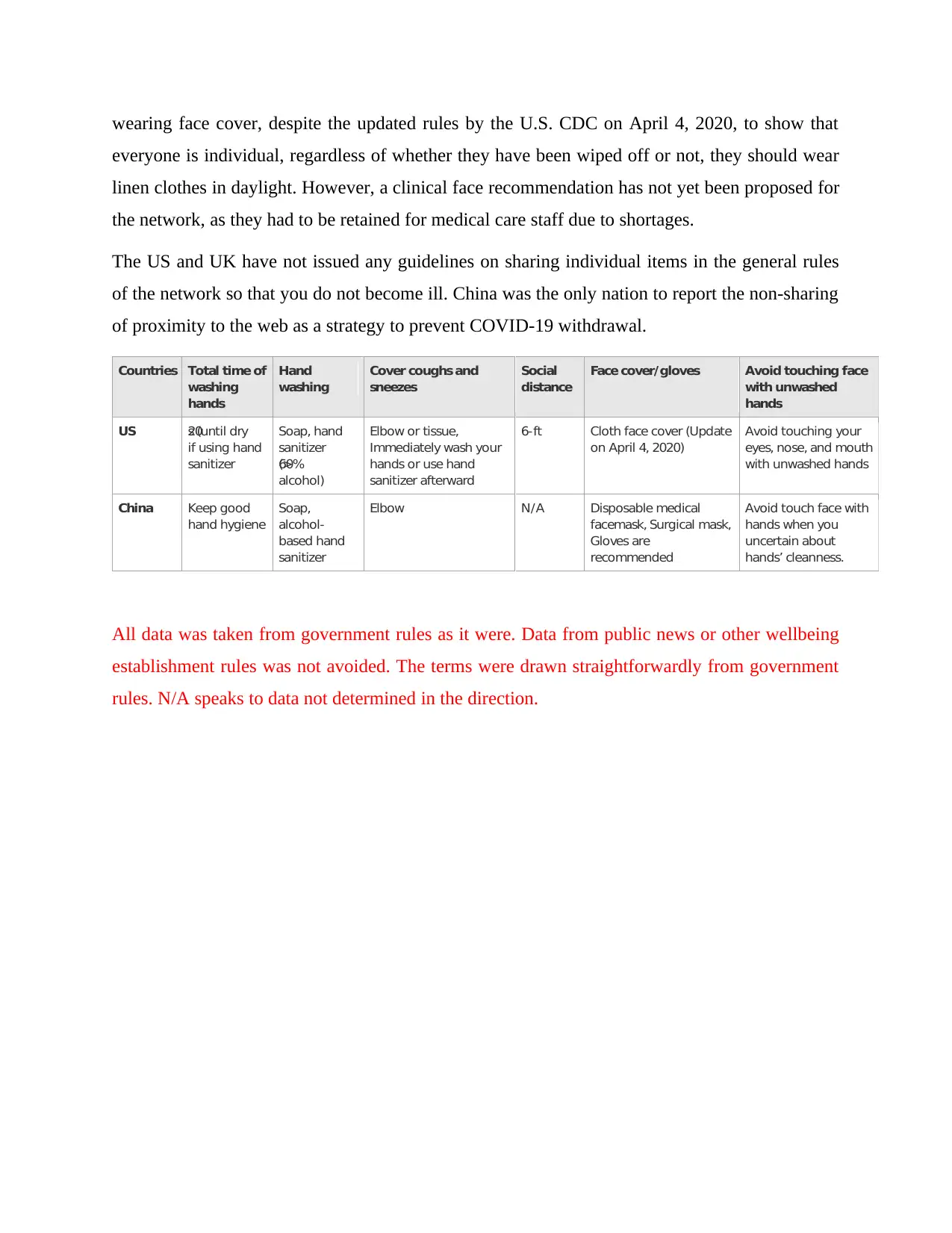
The US and UK have not issued any guidelines on sharing individual items in the general rules
of the network so that you do not become ill. China was the only nation to report the non-sharing
of proximity to the web as a strategy to prevent COVID-19 withdrawal.
Countries Total time of
washing
hands
Hand
washing
Cover coughs and
sneezes
Social
distance
Face cover/gloves Avoid touching face
with unwashed
hands
US 20s (until dry
if using hand
sanitizer
Soap, hand
sanitizer
(>60%
alcohol)
Elbow or tissue,
Immediately wash your
hands or use hand
sanitizer afterward
6-ft Cloth face cover (Update
on April 4, 2020)
Avoid touching your
eyes, nose, and mouth
with unwashed hands
China Keep good
hand hygiene
Soap,
alcohol-
based hand
sanitizer
Elbow N/A Disposable medical
facemask, Surgical mask,
Gloves are
recommended
Avoid touch face with
hands when you
uncertain about
hands’ cleanness.
All data was taken from government rules as it were. Data from public news or other wellbeing
establishment rules was not avoided. The terms were drawn straightforwardly from government
rules. N/A speaks to data not determined in the direction.
everyone is individual, regardless of whether they have been wiped off or not, they should wear
linen clothes in daylight. However, a clinical face recommendation has not yet been proposed for
the network, as they had to be retained for medical care staff due to shortages.
The US and UK have not issued any guidelines on sharing individual items in the general rules
of the network so that you do not become ill. China was the only nation to report the non-sharing
of proximity to the web as a strategy to prevent COVID-19 withdrawal.
Countries Total time of
washing
hands
Hand
washing
Cover coughs and
sneezes
Social
distance
Face cover/gloves Avoid touching face
with unwashed
hands
US 20s (until dry
if using hand
sanitizer
Soap, hand
sanitizer
(>60%
alcohol)
Elbow or tissue,
Immediately wash your
hands or use hand
sanitizer afterward
6-ft Cloth face cover (Update
on April 4, 2020)
Avoid touching your
eyes, nose, and mouth
with unwashed hands
China Keep good
hand hygiene
Soap,
alcohol-
based hand
sanitizer
Elbow N/A Disposable medical
facemask, Surgical mask,
Gloves are
recommended
Avoid touch face with
hands when you
uncertain about
hands’ cleanness.
All data was taken from government rules as it were. Data from public news or other wellbeing
establishment rules was not avoided. The terms were drawn straightforwardly from government
rules. N/A speaks to data not determined in the direction.
7. Conclusion
In summary, both countries have updated their rules, especially screening rules, as COVID-19
has expanded to make stronger moves against the COVID-19 transmission movement and to
help "bending the loop", resulting in a proportion of the burden on individual medical care
facilities. In the basic stages of the event, some procedures were used to control the spread of the
dangerous disease, including isolation of the debilitated, communication and cause social
departure. However, these measures may be of limited value unless the people involved in the
diagnosis are diagnosed. It's annoying, if possible; identify a factor as the best reason for the
spread of Covid, but looking at the practices of these countries it is possible to distinguish
between several components that contribute to a generally powerful approach to reducing its
transmission. Additionally, there are a number of factors that influence the prevalence and
prevalence of COVID-19, including population thickness, differences in the basis of medical
care, and essential modes of transportation. Future studies should focus on these elements and
their impact on the prevalence and prevalence of COVID-19.
In summary, both countries have updated their rules, especially screening rules, as COVID-19
has expanded to make stronger moves against the COVID-19 transmission movement and to
help "bending the loop", resulting in a proportion of the burden on individual medical care
facilities. In the basic stages of the event, some procedures were used to control the spread of the
dangerous disease, including isolation of the debilitated, communication and cause social
departure. However, these measures may be of limited value unless the people involved in the
diagnosis are diagnosed. It's annoying, if possible; identify a factor as the best reason for the
spread of Covid, but looking at the practices of these countries it is possible to distinguish
between several components that contribute to a generally powerful approach to reducing its
transmission. Additionally, there are a number of factors that influence the prevalence and
prevalence of COVID-19, including population thickness, differences in the basis of medical
care, and essential modes of transportation. Future studies should focus on these elements and
their impact on the prevalence and prevalence of COVID-19.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.