PUBH640 Global Health: Salt Reduction Initiative, Policy & Impact
VerifiedAdded on 2023/06/11
|11
|3325
|255
Report
AI Summary
This report delves into the critical issue of salt reduction as a global health strategy, emphasizing its link to lower blood pressure and reduced cardiovascular disease risk. It examines the UK Food Standards Agency's salt reduction program (2003-2010) as a case study, detailing its multi-pronged approach involving food industry engagement, consumer awareness campaigns, and front-of-pack labeling. The report identifies potential barriers and enablers for successful implementation, such as food safety concerns, consumer acceptance, and the importance of a conducive environment with motivated stakeholders. Furthermore, it proposes a qualitative study design to assess consumer understanding of nutrition labels and the need for salt reduction, highlighting the significance of consistent labeling methods and targeted public education. The document concludes by underscoring the importance of ongoing efforts to influence consumer behavior and create a supportive environment for sustained salt reduction, and students can find similar solved assignments and past papers on Desklib.

Global Health 1
Global health and sustainable development
Name
University
Global health and sustainable development
Name
University
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global Health 2
Reduction of salt intake is linked to lower levels of blood pressure and reduction in
the risk of cardiovascular disease. Hypertension is a global health problem and it increases
the risk of cardiovascular disease. Prevention of chronic diseases is a public health priority, it
is important to aim at reducing salt intake, particularly since there is evidence that it reduces
diastolic and systolic blood pressure (He, Li, & Macgregor, 2013). The public burden of
cardiovascular disease can be reduced and a reduction in health care costs are the benefits
derived from population-wide reduced sodium intake (Cobb, Appel, & Anderson, 2012). In
the developing world, the fiscal challenges leave little to cope with the increasing
expenditures on healthcare. Interventions that reduce the incidence hypertension, or that can
control and prevent associated chronic diseases through health education have been
recognised as an important step towards reducing inequities in delivery of healthcare
(Livingston, 1985). The importance of an initiative is underlined in settings where non-
adherence to a low-salt diet is common and hypertension remains uncontrolled (Shima,
Farizah, & Majid, 2014). 49% of coronary heart disease and 62% of strokes occur due to
hypertension and a reduction in salt intake can reduce the disease burden to a considerable
extent. Reduction in salt intake can be brought about through reduction in added salt in
processed food that accounts for 75% of the salt intake in Western diets. Additionally,
educating people about reduced addition of salt to home-cooked food can help reduce the
consumption of salt and reach closer to the target of consuming less salt (3 g/d) as per the
WHO recommendation (WHO, 2012; He & McGregor, A comprehensive review on salt and
health and current experience of worldwide salt reduction programmes., 2009). In economic
terms the benefit of a reduced salt diet by 3g/d and the concomitant reduction in blood
pressure can save upto $24 billion in healthcare costs each year, according to a Portuguese
study. A saving of 392,000 quality adjusted life years and a drop of 92000 deaths every year
are benefits that emphasize the importance of reduction in salt intake (Bibbins-Domingo, et
Reduction of salt intake is linked to lower levels of blood pressure and reduction in
the risk of cardiovascular disease. Hypertension is a global health problem and it increases
the risk of cardiovascular disease. Prevention of chronic diseases is a public health priority, it
is important to aim at reducing salt intake, particularly since there is evidence that it reduces
diastolic and systolic blood pressure (He, Li, & Macgregor, 2013). The public burden of
cardiovascular disease can be reduced and a reduction in health care costs are the benefits
derived from population-wide reduced sodium intake (Cobb, Appel, & Anderson, 2012). In
the developing world, the fiscal challenges leave little to cope with the increasing
expenditures on healthcare. Interventions that reduce the incidence hypertension, or that can
control and prevent associated chronic diseases through health education have been
recognised as an important step towards reducing inequities in delivery of healthcare
(Livingston, 1985). The importance of an initiative is underlined in settings where non-
adherence to a low-salt diet is common and hypertension remains uncontrolled (Shima,
Farizah, & Majid, 2014). 49% of coronary heart disease and 62% of strokes occur due to
hypertension and a reduction in salt intake can reduce the disease burden to a considerable
extent. Reduction in salt intake can be brought about through reduction in added salt in
processed food that accounts for 75% of the salt intake in Western diets. Additionally,
educating people about reduced addition of salt to home-cooked food can help reduce the
consumption of salt and reach closer to the target of consuming less salt (3 g/d) as per the
WHO recommendation (WHO, 2012; He & McGregor, A comprehensive review on salt and
health and current experience of worldwide salt reduction programmes., 2009). In economic
terms the benefit of a reduced salt diet by 3g/d and the concomitant reduction in blood
pressure can save upto $24 billion in healthcare costs each year, according to a Portuguese
study. A saving of 392,000 quality adjusted life years and a drop of 92000 deaths every year
are benefits that emphasize the importance of reduction in salt intake (Bibbins-Domingo, et
Global Health 3
al., 2010). Historically, man consumed as less as 0.25g of salt per day. But with its use in
preservation the use increased and though the advent of refrigeration caused some reduction,
the use of salt is still as high as 9 - 12 g/day. Governments of countries such as, Japan and
Finland have run public health campaigns to reduce salt intake (He & McGregor, A
comprehensive review on salt and health and current experience of worldwide salt reduction
programmes., 2009). The INTERSALT study established a link between increased sodium
intake, measured by urinary sodium excretion per day and increase in systolic blood pressure
with age (Group, 1988). Another study, the INTERMAP study compared salt intake and
several other micro- and macronutrient intake of participants from China, Japan, UK and
USA. The sodium intake was found to be higher among the Asians than their western
counterparts (Zhou, et al., 2003). Although current targets for salt reduction are 5-6g/d from
the current 9-12g/d of salt, a drop to the WHO recommended levels of 3g/d would be ideally
suited for maintenance of blood pressure in the normotensive range. Salt reduction initiatives
and programs have been started in many countries around the world (Webster, Dunford,
Hawkes, & Neal, 2011).
2. Solution generation :Description of initiative and how it may be used to change policy
and practice
The UK Food Standards Agency (FSA) ran a salt reduction program from the year 2003 to
2010. The Scientific Advisory Committee on Nutrition that advised the government on issues
related to nutrition in the UK recommended reduce salt intake to prevent morbidity and
mortality due to cardiovascular disease. It was estimated that 6% deaths due to coronary heart
disease could be reduced if the number of hypertensive persons could be reduced by 50%. If
the mean diastolic blood pressure could be lowered by just 2 mmHg, a 15% drop in the
incidence of stroke and transient ischemic attack can occur. A 6% drop in coronary heart
disease would be another positive outcome. From the then average consumption of 9.5 g/d of
al., 2010). Historically, man consumed as less as 0.25g of salt per day. But with its use in
preservation the use increased and though the advent of refrigeration caused some reduction,
the use of salt is still as high as 9 - 12 g/day. Governments of countries such as, Japan and
Finland have run public health campaigns to reduce salt intake (He & McGregor, A
comprehensive review on salt and health and current experience of worldwide salt reduction
programmes., 2009). The INTERSALT study established a link between increased sodium
intake, measured by urinary sodium excretion per day and increase in systolic blood pressure
with age (Group, 1988). Another study, the INTERMAP study compared salt intake and
several other micro- and macronutrient intake of participants from China, Japan, UK and
USA. The sodium intake was found to be higher among the Asians than their western
counterparts (Zhou, et al., 2003). Although current targets for salt reduction are 5-6g/d from
the current 9-12g/d of salt, a drop to the WHO recommended levels of 3g/d would be ideally
suited for maintenance of blood pressure in the normotensive range. Salt reduction initiatives
and programs have been started in many countries around the world (Webster, Dunford,
Hawkes, & Neal, 2011).
2. Solution generation :Description of initiative and how it may be used to change policy
and practice
The UK Food Standards Agency (FSA) ran a salt reduction program from the year 2003 to
2010. The Scientific Advisory Committee on Nutrition that advised the government on issues
related to nutrition in the UK recommended reduce salt intake to prevent morbidity and
mortality due to cardiovascular disease. It was estimated that 6% deaths due to coronary heart
disease could be reduced if the number of hypertensive persons could be reduced by 50%. If
the mean diastolic blood pressure could be lowered by just 2 mmHg, a 15% drop in the
incidence of stroke and transient ischemic attack can occur. A 6% drop in coronary heart
disease would be another positive outcome. From the then average consumption of 9.5 g/d of
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Global Health 4
salt consumption, a target level of 6 g/d was determined (Wyness, Butriss, & Stanner, 2011).
Rather than the 3 g/d recommended consumption by WHO, the 6g/d target was considered to
be more achievable at the population level (WHO, 2012). The key inputs to the programme
involved the UK food industry that was asked to reduce salt content in their formulations of
processed food. They were also asked to change the nutrition labels to formats that could be
easily understood by the consumers. Consumer awareness campaigns for a low salt intake
and raising consumer demand foe low salt containing foods was also part of the initiative. But
the current salt consumption in UK has only dropped to 8.1 to 8.8 g/d. The target of 6 g/d is
still distant (Food.gov.uk, 2017).
Food industry was given targets to achieve for reduced salt content in their processed food
products. While some players were able to exceed targets, others had problems due to
technical reasons and acceptability issues from consumers. The FSA continued with their
engagement with the food industry and in 2012 new targets were given to the producers. An
environment to continuous efforts towards reducing the salt content further has been an
achievement.
Front of pack labelling encouraged by the FSA in addition to nutrition information also
provides information on how healthy a food item is. Consumer behaviour in supermarkets is
influenced when they choose foods labelled as healthy than foods that are less healthy.
Indirectly, the food industry was also encouraged to label their foods with guideline daily
amount (GDA) of nutrients. Traffic light colour coding helped consumers to choose foods
that had more greens (low) than ambers (high).
Consumer awareness campaigns formed an important part of the salt reduction programme.
Print media, television, radio, digital media and the government website were used to relay
information about the need to reduce salt intake. Hard to reach sections of the population,
such as, certain ethnic minorities were taken to grocery shop tours, cooking shows and taught
salt consumption, a target level of 6 g/d was determined (Wyness, Butriss, & Stanner, 2011).
Rather than the 3 g/d recommended consumption by WHO, the 6g/d target was considered to
be more achievable at the population level (WHO, 2012). The key inputs to the programme
involved the UK food industry that was asked to reduce salt content in their formulations of
processed food. They were also asked to change the nutrition labels to formats that could be
easily understood by the consumers. Consumer awareness campaigns for a low salt intake
and raising consumer demand foe low salt containing foods was also part of the initiative. But
the current salt consumption in UK has only dropped to 8.1 to 8.8 g/d. The target of 6 g/d is
still distant (Food.gov.uk, 2017).
Food industry was given targets to achieve for reduced salt content in their processed food
products. While some players were able to exceed targets, others had problems due to
technical reasons and acceptability issues from consumers. The FSA continued with their
engagement with the food industry and in 2012 new targets were given to the producers. An
environment to continuous efforts towards reducing the salt content further has been an
achievement.
Front of pack labelling encouraged by the FSA in addition to nutrition information also
provides information on how healthy a food item is. Consumer behaviour in supermarkets is
influenced when they choose foods labelled as healthy than foods that are less healthy.
Indirectly, the food industry was also encouraged to label their foods with guideline daily
amount (GDA) of nutrients. Traffic light colour coding helped consumers to choose foods
that had more greens (low) than ambers (high).
Consumer awareness campaigns formed an important part of the salt reduction programme.
Print media, television, radio, digital media and the government website were used to relay
information about the need to reduce salt intake. Hard to reach sections of the population,
such as, certain ethnic minorities were taken to grocery shop tours, cooking shows and taught
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global Health 5
how to choose foods and read labels so that salt intake would remain low. Awareness
campaigns called 'Sid the slug', 'Talking food' and 'Full of it' tackled different aspects and
spread the word about reducing salt intake among consumers.
The food service sector, though not part of the initiative was also engaged and catering
services, restaurants and sandwich outlets were also part of the reduced salt initiative and
were educated on how to reduce addition of salt. The multi-pronged approach helped to reach
the goal of reducing salt intake by the UK population.
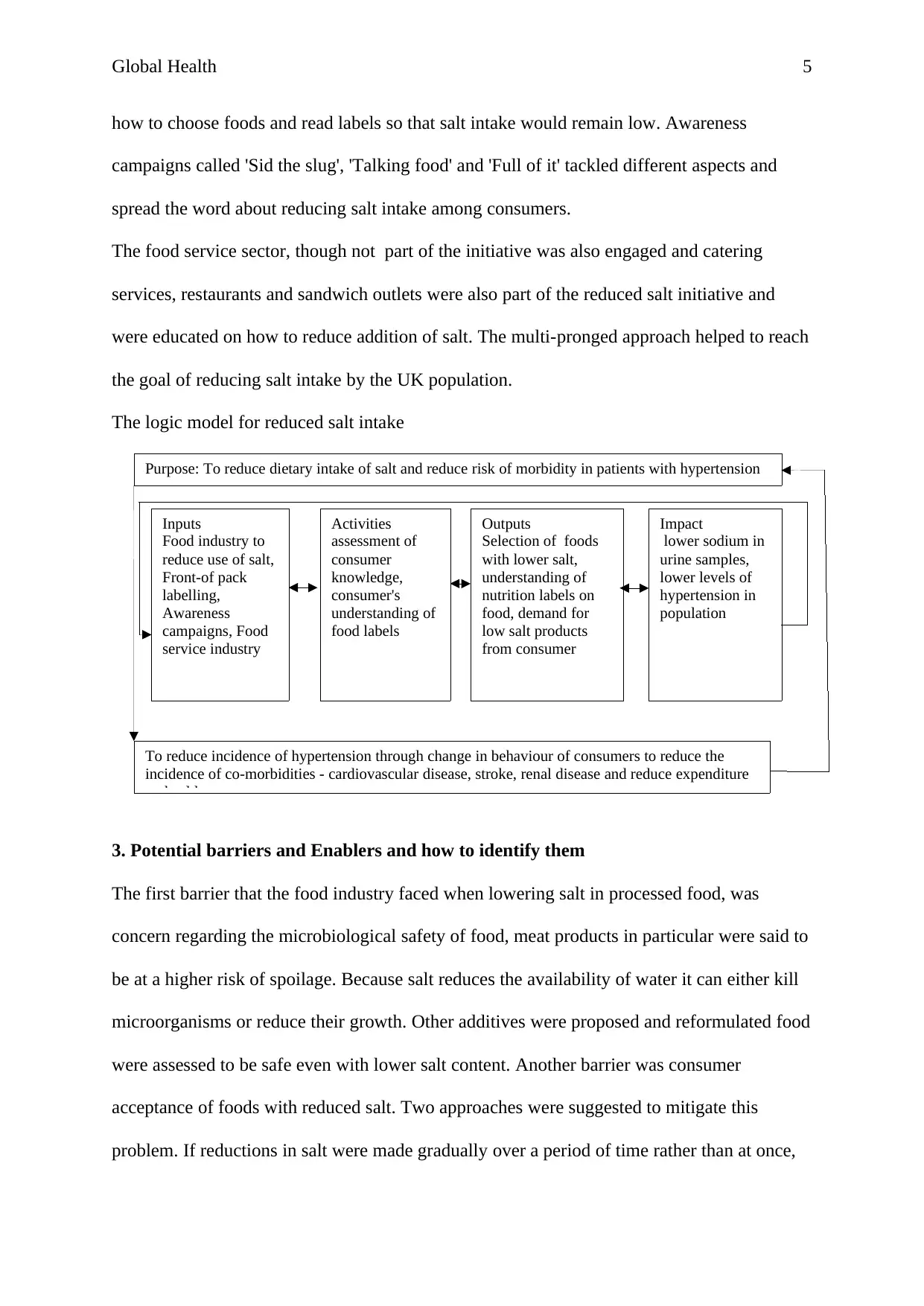
The logic model for reduced salt intake
3. Potential barriers and Enablers and how to identify them
The first barrier that the food industry faced when lowering salt in processed food, was
concern regarding the microbiological safety of food, meat products in particular were said to
be at a higher risk of spoilage. Because salt reduces the availability of water it can either kill
microorganisms or reduce their growth. Other additives were proposed and reformulated food
were assessed to be safe even with lower salt content. Another barrier was consumer
acceptance of foods with reduced salt. Two approaches were suggested to mitigate this
problem. If reductions in salt were made gradually over a period of time rather than at once,
Purpose: To reduce dietary intake of salt and reduce risk of morbidity in patients with hypertension
To reduce incidence of hypertension through change in behaviour of consumers to reduce the
incidence of co-morbidities - cardiovascular disease, stroke, renal disease and reduce expenditure
on health care.
Inputs
Food industry to
reduce use of salt,
Front-of pack
labelling,
Awareness
campaigns, Food
service industry
Activities
assessment of
consumer
knowledge,
consumer's
understanding of
food labels
Outputs
Selection of foods
with lower salt,
understanding of
nutrition labels on
food, demand for
low salt products
from consumer
Impact
lower sodium in
urine samples,
lower levels of
hypertension in
population
how to choose foods and read labels so that salt intake would remain low. Awareness
campaigns called 'Sid the slug', 'Talking food' and 'Full of it' tackled different aspects and
spread the word about reducing salt intake among consumers.
The food service sector, though not part of the initiative was also engaged and catering
services, restaurants and sandwich outlets were also part of the reduced salt initiative and
were educated on how to reduce addition of salt. The multi-pronged approach helped to reach
the goal of reducing salt intake by the UK population.
The logic model for reduced salt intake
3. Potential barriers and Enablers and how to identify them
The first barrier that the food industry faced when lowering salt in processed food, was
concern regarding the microbiological safety of food, meat products in particular were said to
be at a higher risk of spoilage. Because salt reduces the availability of water it can either kill
microorganisms or reduce their growth. Other additives were proposed and reformulated food
were assessed to be safe even with lower salt content. Another barrier was consumer
acceptance of foods with reduced salt. Two approaches were suggested to mitigate this
problem. If reductions in salt were made gradually over a period of time rather than at once,
Purpose: To reduce dietary intake of salt and reduce risk of morbidity in patients with hypertension
To reduce incidence of hypertension through change in behaviour of consumers to reduce the
incidence of co-morbidities - cardiovascular disease, stroke, renal disease and reduce expenditure
on health care.
Inputs
Food industry to
reduce use of salt,
Front-of pack
labelling,
Awareness
campaigns, Food
service industry
Activities
assessment of
consumer
knowledge,
consumer's
understanding of
food labels
Outputs
Selection of foods
with lower salt,
understanding of
nutrition labels on
food, demand for
low salt products
from consumer
Impact
lower sodium in
urine samples,
lower levels of
hypertension in
population
Global Health 6
consumers were able to accept the change more readily. Besides, the use of lesser salt is a
behaviour change that consumer palates are still adjusting to, an 8 week period is required to
accept low salt content. In certain foods like bread and cheese, the addition of salt is
technically intrinsic to the fermentation process and separation of whey. In such cases, the
FSA has allowed for a longer time period for the resolution and has supported the industry
with research projects that are working towards the development of low salt breads and low
salt cheese. This creates an enabling environment for stakeholders in the food industry and
ensures that their participation in the intervention will remain constructive. There has been
evidence of voluntary salt reduction by food industry. The consumer awareness program
needs to teach people to monitor their own salt intake through careful reading of nutrition
labels on packaged food and reduce addition of salt to home cooked food (Xuereb, 2013).
In order to provide equitable outreach to all sections of the population, special programs for
campaign effectiveness among the ethnic minorities are necessary. Public education through
campaigns is effective and relatively cheap. But it has to be coupled with the availability of
low sodium containing food. Dietary counselling by physicians and healthcare professionals
can help in disseminating information about the need to reduce sodium intake. Apart from
reading labels advice about eating fresh foods rather than processed food, avoiding
seasonings that contain sodium, choosing foods with less sodium, are steps that are easy to
follow (Cobb, Appel, & Anderson, 2012).
Efforts to influence consumer behaviour and reduce salt intake have to be made in an
environment that is conducive to change. Creating such an environment is possible when all
the stakeholders including the regulatory bodies, policy makers, food industry, consumers
and health professionals are highly motivated by a strong leadership and appropriate funding.
Behaviour change of consumers and keeping their motivation to reduce salt intake are
important factors in reaching the goal. Understanding nutrition labels and quickly calculating
consumers were able to accept the change more readily. Besides, the use of lesser salt is a
behaviour change that consumer palates are still adjusting to, an 8 week period is required to
accept low salt content. In certain foods like bread and cheese, the addition of salt is
technically intrinsic to the fermentation process and separation of whey. In such cases, the
FSA has allowed for a longer time period for the resolution and has supported the industry
with research projects that are working towards the development of low salt breads and low
salt cheese. This creates an enabling environment for stakeholders in the food industry and
ensures that their participation in the intervention will remain constructive. There has been
evidence of voluntary salt reduction by food industry. The consumer awareness program
needs to teach people to monitor their own salt intake through careful reading of nutrition
labels on packaged food and reduce addition of salt to home cooked food (Xuereb, 2013).
In order to provide equitable outreach to all sections of the population, special programs for
campaign effectiveness among the ethnic minorities are necessary. Public education through
campaigns is effective and relatively cheap. But it has to be coupled with the availability of
low sodium containing food. Dietary counselling by physicians and healthcare professionals
can help in disseminating information about the need to reduce sodium intake. Apart from
reading labels advice about eating fresh foods rather than processed food, avoiding
seasonings that contain sodium, choosing foods with less sodium, are steps that are easy to
follow (Cobb, Appel, & Anderson, 2012).
Efforts to influence consumer behaviour and reduce salt intake have to be made in an
environment that is conducive to change. Creating such an environment is possible when all
the stakeholders including the regulatory bodies, policy makers, food industry, consumers
and health professionals are highly motivated by a strong leadership and appropriate funding.
Behaviour change of consumers and keeping their motivation to reduce salt intake are
important factors in reaching the goal. Understanding nutrition labels and quickly calculating
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Global Health 7
the general dietary allowance calls for numeracy, that many consumers find difficult when
shopping in a supermarket. Making a quick assessment of salt intake through nutrition labels
is difficult for informed and motivated consumers. Public awareness programs should focus
on increasing consumer education through various media (McLean & Hoek, 2014).
4. Implementation of the initiative, qualitative study design, assessment of outcomes and
which outcomes studied to examine impact
Implementation of the initiative should focus on increasing public awareness. Some
consumers may have understood the need to reduce salt intake. But there are many who have
not understood the link between salt intake and health. There are difficulties in understanding
food labels and assessment of their understanding is important in order to fill gaps with easy
to understand campaign material (Cowburn & Stockley, 2004). An Australian study found
that consumers did not have the ability to understand labels that mentioned salt and/or
sodium, although 88% of the study participants were aware that high salt intake is linked to
hypertension. Nutrition labelling should follow consistent methods of labelling (Grimes,
Riddell, & Nowson, 2009).
A qualitative study design to assess consumer understanding of the need to reduce salt intake
and their understanding of nutrition labels needs to be assessed.
Questionnaire for qualitative study design to assess consumer knowledge about how to read
and interpret nutrition labels:
1. What influences your decision to buy a particular food product when grocery shopping and
do you think it is better to consume fresh food or processed food?
2. Do you read nutrition information printed on the food package when purchasing food?
3. Would you select foods with more green or more amber signs?
4. How do you find the amount of salt in the food?
5. What is the guideline daily allowance for salt in the UK?
the general dietary allowance calls for numeracy, that many consumers find difficult when
shopping in a supermarket. Making a quick assessment of salt intake through nutrition labels
is difficult for informed and motivated consumers. Public awareness programs should focus
on increasing consumer education through various media (McLean & Hoek, 2014).
4. Implementation of the initiative, qualitative study design, assessment of outcomes and
which outcomes studied to examine impact
Implementation of the initiative should focus on increasing public awareness. Some
consumers may have understood the need to reduce salt intake. But there are many who have
not understood the link between salt intake and health. There are difficulties in understanding
food labels and assessment of their understanding is important in order to fill gaps with easy
to understand campaign material (Cowburn & Stockley, 2004). An Australian study found
that consumers did not have the ability to understand labels that mentioned salt and/or
sodium, although 88% of the study participants were aware that high salt intake is linked to
hypertension. Nutrition labelling should follow consistent methods of labelling (Grimes,
Riddell, & Nowson, 2009).
A qualitative study design to assess consumer understanding of the need to reduce salt intake
and their understanding of nutrition labels needs to be assessed.
Questionnaire for qualitative study design to assess consumer knowledge about how to read
and interpret nutrition labels:
1. What influences your decision to buy a particular food product when grocery shopping and
do you think it is better to consume fresh food or processed food?
2. Do you read nutrition information printed on the food package when purchasing food?
3. Would you select foods with more green or more amber signs?
4. How do you find the amount of salt in the food?
5. What is the guideline daily allowance for salt in the UK?
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global Health 8
6. Why is it important to read the salt content of a food?
7. Is the sodium content of food related to salt content?
8. What could be the consequence if you consumed more salt than is recommended?
9. Which foods would you choose to minimise the salt intake?
10. Which nutrient labelling format do you understand?
11. Does it help while selecting food with front of pack labels about fat, saturates, sugar and
salt?
12. Does it help to have labels in the form of traffic light colour coding on food packages?
The questionnaire can be given to consumers to assess their knowledge and engagement with
the subject of reducing salt intake.
The questionnaire would be given to persons who do most of the grocery shopping for the
household. The whole family consumes the foods purchased by one or two people. Some
family members or the buyers themselves could be suffering from hypertension. In such a
case, it will be interesting to learn more about the attitude of the buyer towards the salt
content in the food. The salt restrictions are recommended to be followed by the children, and
the normotensive members of the family.
5. Strategies to disseminate the outcomes of the initiative
Dissemination of the outcome of the qualitative study is important because it will be useful in
addressing the shortcomings in the understanding of consumers regarding nutrition labelling.
The main findings of the study are usually mentioned in a bullet point format on the first
page. Policy makers can use it as a quick reference guide when formulating a policy change.
These are the main implications of the evaluation of the proposed initiative. The following
three pages should concisely describe the findings of the qualitative study. A detailed high
quality report should follow and must include the analysis of the study and give
recommendations. Other formats that can be used to disseminate information about the study
6. Why is it important to read the salt content of a food?
7. Is the sodium content of food related to salt content?
8. What could be the consequence if you consumed more salt than is recommended?
9. Which foods would you choose to minimise the salt intake?
10. Which nutrient labelling format do you understand?
11. Does it help while selecting food with front of pack labels about fat, saturates, sugar and
salt?
12. Does it help to have labels in the form of traffic light colour coding on food packages?
The questionnaire can be given to consumers to assess their knowledge and engagement with
the subject of reducing salt intake.
The questionnaire would be given to persons who do most of the grocery shopping for the
household. The whole family consumes the foods purchased by one or two people. Some
family members or the buyers themselves could be suffering from hypertension. In such a
case, it will be interesting to learn more about the attitude of the buyer towards the salt
content in the food. The salt restrictions are recommended to be followed by the children, and
the normotensive members of the family.
5. Strategies to disseminate the outcomes of the initiative
Dissemination of the outcome of the qualitative study is important because it will be useful in
addressing the shortcomings in the understanding of consumers regarding nutrition labelling.
The main findings of the study are usually mentioned in a bullet point format on the first
page. Policy makers can use it as a quick reference guide when formulating a policy change.
These are the main implications of the evaluation of the proposed initiative. The following
three pages should concisely describe the findings of the qualitative study. A detailed high
quality report should follow and must include the analysis of the study and give
recommendations. Other formats that can be used to disseminate information about the study

Global Health 9
on consumer understanding could be papers published in journals. This would allow the
academic community to access the findings (Health.vic.gov.au, 2011).
on consumer understanding could be papers published in journals. This would allow the
academic community to access the findings (Health.vic.gov.au, 2011).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Global Health 10
References
Bibbins-Domingo, K. C.-D., Chertow, G. M., Coxson, P., Moran, A. E., Lightwood, J. M.,
Pletcher, M. J., & Goldman, L. (2010). Reductions in Cardiovascular Disease
Projected from Modest Reductions in Dietary Salt. The New England Journal of
Medicine, 362(7):590-599.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066566/
Cobb, L. K., Appel, L. J., & Anderson, C. A. (2012). Strategies to Reduce Dietary Sodium
Intake. Current Treatment Options in Cardiovascular Medicine, 14(4): 425–434.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3612540/
Cowburn, G., & Stockley, L. (2004). Consumer understanding and use of nutrition labelling:.
Public Health Nutrition , 8(1): 21–28.
https://www.researchgate.net/profile/Gill_Cowburn/publication/
8028200_Consumer_understanding_and_use_of_nutrition_labelling_A_systematic_review/
links/0c9605278c3630eab3000000.pdf
Food.gov.uk. (2017). /salt. Retrieved from https://www.food.gov.uk:
https://www.food.gov.uk/business-guidance/salt
Grimes, C., Riddell, L., & Nowson, C. (2009). Consumer knowledge and attitudes to salt
intake and labelled salt information. Appetite, 53(2):189-194.
https://www.sciencedirect.com/science/article/pii/S019566630900542X
Group, I. C. (1988). Intersalt: an international study of electrolyte excretion and blood
pressure. Results for 24 hour urinary sodium and potassium excretion. . BMJ : British
Medical Journal, 297(6644), 319–328.
https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/3416162/
He, F., & McGregor, G. (2009). A comprehensive review on salt and health and current
experience of worldwide salt reduction programmes. Journal of human hypertension,
23(6):363-84.
https://www.nature.com/articles/jhh2008144
He, F., Li, J., & Macgregor, G. (2013). Effect of longer term modest salt reduction on blood
pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ,
346:f1325. doi: 10.1136/bmj.f1325.
https://www.bmj.com/content/346/bmj.f1325.long
Health.vic.gov.au. (2011). Evaluation-framework-for-health-promotion-and-disease-
prevention-programs. Retrieved from https://www2.health.vic.gov.au/:
https://www2.health.vic.gov.au/about/publications/policiesandguidelines/Evaluation-
framework-for-health-promotion-and-disease-prevention-programs
Livingston, I. L. (1985). Hypertension and Health Education Intervention in the Caribbean: A
Public Health Appraisal. . Journal of the National Medical Association, 77(4):273–
280.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2561854/
References
Bibbins-Domingo, K. C.-D., Chertow, G. M., Coxson, P., Moran, A. E., Lightwood, J. M.,
Pletcher, M. J., & Goldman, L. (2010). Reductions in Cardiovascular Disease
Projected from Modest Reductions in Dietary Salt. The New England Journal of
Medicine, 362(7):590-599.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066566/
Cobb, L. K., Appel, L. J., & Anderson, C. A. (2012). Strategies to Reduce Dietary Sodium
Intake. Current Treatment Options in Cardiovascular Medicine, 14(4): 425–434.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3612540/
Cowburn, G., & Stockley, L. (2004). Consumer understanding and use of nutrition labelling:.
Public Health Nutrition , 8(1): 21–28.
https://www.researchgate.net/profile/Gill_Cowburn/publication/
8028200_Consumer_understanding_and_use_of_nutrition_labelling_A_systematic_review/
links/0c9605278c3630eab3000000.pdf
Food.gov.uk. (2017). /salt. Retrieved from https://www.food.gov.uk:
https://www.food.gov.uk/business-guidance/salt
Grimes, C., Riddell, L., & Nowson, C. (2009). Consumer knowledge and attitudes to salt
intake and labelled salt information. Appetite, 53(2):189-194.
https://www.sciencedirect.com/science/article/pii/S019566630900542X
Group, I. C. (1988). Intersalt: an international study of electrolyte excretion and blood
pressure. Results for 24 hour urinary sodium and potassium excretion. . BMJ : British
Medical Journal, 297(6644), 319–328.
https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/3416162/
He, F., & McGregor, G. (2009). A comprehensive review on salt and health and current
experience of worldwide salt reduction programmes. Journal of human hypertension,
23(6):363-84.
https://www.nature.com/articles/jhh2008144
He, F., Li, J., & Macgregor, G. (2013). Effect of longer term modest salt reduction on blood
pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ,
346:f1325. doi: 10.1136/bmj.f1325.
https://www.bmj.com/content/346/bmj.f1325.long
Health.vic.gov.au. (2011). Evaluation-framework-for-health-promotion-and-disease-
prevention-programs. Retrieved from https://www2.health.vic.gov.au/:
https://www2.health.vic.gov.au/about/publications/policiesandguidelines/Evaluation-
framework-for-health-promotion-and-disease-prevention-programs
Livingston, I. L. (1985). Hypertension and Health Education Intervention in the Caribbean: A
Public Health Appraisal. . Journal of the National Medical Association, 77(4):273–
280.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2561854/
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global Health 11
McLean, R., & Hoek, J. (2014). Sodium and nutrition labelling: a qualitative study exploring
New Zealand consumers’ food purchasing behaviours. Public Health
NutritionVolume 17 Issue 5, 17(5):1138-1146.
https://www.cambridge.org/core/journals/public-health-nutrition/article/sodium-and-
nutrition-labelling-a-qualitative-study-exploring-new-zealand-consumers-food-purchasing-
behaviours/1EBB949FA607652810E2F4C98E721798/core-reader
Shima, R., Farizah, M. H., & Majid, H. A. (2014). A qualitative study on hypertensive care
behavior in primary health care settings in Malaysia. Patient Preference and
Adherence, 8: 1597–1609.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4240212/
Webster, J., Dunford, E., Hawkes, C., & Neal, B. (2011). Salt reduction initiatives around the
world. Journal of hypertension, 29(6):1043-50.
WHO. (2012). sodium_intake_printversion.pdf. Retrieved from http://www.who.int/:
http://www.who.int/nutrition/publications/guidelines/sodium_intake_printversion.pdf
Wyness, L., Butriss, J., & Stanner, S. (2011). Reducing the population’s sodium intake: the
UK Food. Public Health Nutrition, 15(2): 254–261 .
https://www.researchgate.net/profile/Sara_Stanner/publication/
51467550_Reducing_the_population's_sodium_intake_the_UK_Food_Standards_Agency's_
Salt_Reduction_Programme/links/542d45530cf27e39fa94236e.pdf
Xuereb, G. (2013). SRP_2013_Godfrey_Xuereb_WHO.pdf. Retrieved from
https://www.fsai.ie:
https://www.fsai.ie/uploadedFiles/Science_and_Health/Salt_and_Health/
SRP_2013_Godfrey_Xuereb_WHO.pdf
Zhou, B., Stamler, J., Dennis, B., Moag-Stahlberg, A., Okuda, N., Robertson, C., . . . Group,
I. R. (2003). Nutrient intakes of middle-aged men and women in China, Japan, United
Kingdom, and United States in the late 1990s: the INTERMAP study. Journal of
human hypertension, 17(9):623-30.
https://www.ncbi.nlm.nih.gov/pubmed/13679952
McLean, R., & Hoek, J. (2014). Sodium and nutrition labelling: a qualitative study exploring
New Zealand consumers’ food purchasing behaviours. Public Health
NutritionVolume 17 Issue 5, 17(5):1138-1146.
https://www.cambridge.org/core/journals/public-health-nutrition/article/sodium-and-
nutrition-labelling-a-qualitative-study-exploring-new-zealand-consumers-food-purchasing-
behaviours/1EBB949FA607652810E2F4C98E721798/core-reader
Shima, R., Farizah, M. H., & Majid, H. A. (2014). A qualitative study on hypertensive care
behavior in primary health care settings in Malaysia. Patient Preference and
Adherence, 8: 1597–1609.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4240212/
Webster, J., Dunford, E., Hawkes, C., & Neal, B. (2011). Salt reduction initiatives around the
world. Journal of hypertension, 29(6):1043-50.
WHO. (2012). sodium_intake_printversion.pdf. Retrieved from http://www.who.int/:
http://www.who.int/nutrition/publications/guidelines/sodium_intake_printversion.pdf
Wyness, L., Butriss, J., & Stanner, S. (2011). Reducing the population’s sodium intake: the
UK Food. Public Health Nutrition, 15(2): 254–261 .
https://www.researchgate.net/profile/Sara_Stanner/publication/
51467550_Reducing_the_population's_sodium_intake_the_UK_Food_Standards_Agency's_
Salt_Reduction_Programme/links/542d45530cf27e39fa94236e.pdf
Xuereb, G. (2013). SRP_2013_Godfrey_Xuereb_WHO.pdf. Retrieved from
https://www.fsai.ie:
https://www.fsai.ie/uploadedFiles/Science_and_Health/Salt_and_Health/
SRP_2013_Godfrey_Xuereb_WHO.pdf
Zhou, B., Stamler, J., Dennis, B., Moag-Stahlberg, A., Okuda, N., Robertson, C., . . . Group,
I. R. (2003). Nutrient intakes of middle-aged men and women in China, Japan, United
Kingdom, and United States in the late 1990s: the INTERMAP study. Journal of
human hypertension, 17(9):623-30.
https://www.ncbi.nlm.nih.gov/pubmed/13679952
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.