Global Health: A Comprehensive Initiative to Reduce Sodium Consumption
VerifiedAdded on 2021/06/15
|16
|4933
|59
Report
AI Summary
This report delves into a global initiative designed to reduce sodium consumption and its impact on public health. It begins by defining the problem of high dietary salt intake, linking it to non-communicable diseases such as cardiovascular disease, stroke, and renal issues. The report then outlines a logic model to explore inputs, outputs, and the overall impact of the initiative. It emphasizes that the majority of sodium intake comes from processed and restaurant foods, and suggests various solutions including reading nutrition labels, choosing fresh foods, avoiding added salt, and reducing food portions. The report further discusses resource mobilization, potential barriers such as poor government policy implementation, insufficient funding, and lack of stakeholder involvement. The enablers include government support and strong inter-organizational links. Public education, individual dietary counseling, food labeling, and coordinated voluntary industry sodium reduction are also discussed as strategies to reduce sodium intake. The report concludes by emphasizing the importance of public awareness and the need for government policies to restrict excessive salt use in processed foods.

Running Head: PUBLIC HEALTH 1
A GLOBAL INITIATIVE TO REDUCE SODIUM CONSUMPTION
Name
Institutional affiliation
A GLOBAL INITIATIVE TO REDUCE SODIUM CONSUMPTION
Name
Institutional affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PUBLIC HEALTH 2
Contents
PROBLEM DEFINITION.................................................................................................................................3
LOGIC MODEL TO EXPLORE THE INPUTS, OUTPUTS, AND IMPACT OF THE INITIATIVE...............................5
RESOURCE MOBILIZATION...........................................................................................................................5
IMPLEMENTATION/OUTCOME ASSESSMENT............................................................................................11
DISSEMINATION........................................................................................................................................13
CONCLUSION.............................................................................................................................................13
REFERENCES..............................................................................................................................................14
Contents
PROBLEM DEFINITION.................................................................................................................................3
LOGIC MODEL TO EXPLORE THE INPUTS, OUTPUTS, AND IMPACT OF THE INITIATIVE...............................5
RESOURCE MOBILIZATION...........................................................................................................................5
IMPLEMENTATION/OUTCOME ASSESSMENT............................................................................................11
DISSEMINATION........................................................................................................................................13
CONCLUSION.............................................................................................................................................13
REFERENCES..............................................................................................................................................14
PUBLIC HEALTH 3
PROBLEM DEFINITION
High dietary salt consumption has been linked to harmful effects such as increased risk of
stroke due to heightened blood pressure, renal disease, and ventricular left hypertrophy. There
are studies that relate salt intake with obesity, with osteoporosis and renal stones and also as a
cause of stomach cancer (Wyness et al., 2012). Because excessive salt consumption is known to
contribute to these non-communicable diseases, the world is looking for ways to reduce salt
intake. Studies have shown that there are 36million deaths caused by non-communicable
diseases around the world which include cancer, diabetes, cardiovascular disease(CVD
andchronic lung diseases (He et al., 2014). This accounts for close to two-thirds of an
approximated 56 million deaths around the world among per year. CVDs the group of conditions
leading to deaths globally with an estimated 17.5 million people having have died from CVDs in
2005 (He et al., 2014). Low-and middle-income countries have over 80% of the estimated deaths
from CVD (He et al., 2015).
Description of the solution for the problem
It has been assumed that use of salt shaker when eating is one of the greatest contributors to
increased salt levels in your diet (Joffres et al., 2013). This, however, is not true, as packaged and
restaurant foods contribute 75% of dietary sodium with only 11% contributed with addition
when eating or cooking(Webster et al., 2014). Sodium exists in foods when purchase them and
this may be reduced in the following ways: with over 1.65 million people dying every year of
CVDs, there is a need for the stakeholders to look for all ways to fight this problem
(Strazzullo et al., 2009). Improper usage of the salt is the problem as opposed to the use
of salt alone and this gives the reason why the world struggles with this problem since the 1970s
(Petersen., 2009).
Reading the nutrition facts label would help to reduce salt intake as one is able to
determine the amount present in the beverage or processed food. This would allow one to
PROBLEM DEFINITION
High dietary salt consumption has been linked to harmful effects such as increased risk of
stroke due to heightened blood pressure, renal disease, and ventricular left hypertrophy. There
are studies that relate salt intake with obesity, with osteoporosis and renal stones and also as a
cause of stomach cancer (Wyness et al., 2012). Because excessive salt consumption is known to
contribute to these non-communicable diseases, the world is looking for ways to reduce salt
intake. Studies have shown that there are 36million deaths caused by non-communicable
diseases around the world which include cancer, diabetes, cardiovascular disease(CVD
andchronic lung diseases (He et al., 2014). This accounts for close to two-thirds of an
approximated 56 million deaths around the world among per year. CVDs the group of conditions
leading to deaths globally with an estimated 17.5 million people having have died from CVDs in
2005 (He et al., 2014). Low-and middle-income countries have over 80% of the estimated deaths
from CVD (He et al., 2015).
Description of the solution for the problem
It has been assumed that use of salt shaker when eating is one of the greatest contributors to
increased salt levels in your diet (Joffres et al., 2013). This, however, is not true, as packaged and
restaurant foods contribute 75% of dietary sodium with only 11% contributed with addition
when eating or cooking(Webster et al., 2014). Sodium exists in foods when purchase them and
this may be reduced in the following ways: with over 1.65 million people dying every year of
CVDs, there is a need for the stakeholders to look for all ways to fight this problem
(Strazzullo et al., 2009). Improper usage of the salt is the problem as opposed to the use
of salt alone and this gives the reason why the world struggles with this problem since the 1970s
(Petersen., 2009).
Reading the nutrition facts label would help to reduce salt intake as one is able to
determine the amount present in the beverage or processed food. This would allow one to
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PUBLIC HEALTH 4
choose the products from manufacturers who have lower salt or sodium contents(World
Health Organization, 2010).
Buying fresh meat, seafood, poultry, then processed one is also advisable to avoid the
increased amount of sodium in the food. It is also advisable to check if salt water or
saline has been added to the fresh meat, seafood, and poultry(Webster et al., 2014).
When cooking or eating, in the table on when baking adding salt should be avoided by
using other flavors in food such as herbs and spices (Strazzullo et al., 2009).
Reducing food portions since more food portion means more salt intake. Make sure you
prepare a small portion of your meal when at home and sometimes share with a friend to
avoid consuming the bigger amount of salts (Liem et al., 2011).
Rinse sodium from foods such as beans, vegetables, and tuna before eating. This will
help you reduce the amount of sodium content in your food.
There is a need to increase public awareness on effects of salts on their health. Bruce
Neal a Professor from UNSW Sydney and George Institute of Global Health says, "Most
of the actions trying to contain how much salt people eat have been about trying to
educate people and tell them about the problem. And that's important, but the food
environment means that's not desperately helpful. It has almost no impact at
all"(McKenzie-Mohr, 2011).
The government should come up with policies which restrict processing industries using
too much salt on the processed food but rather reduce it to a required amount.
choose the products from manufacturers who have lower salt or sodium contents(World
Health Organization, 2010).
Buying fresh meat, seafood, poultry, then processed one is also advisable to avoid the
increased amount of sodium in the food. It is also advisable to check if salt water or
saline has been added to the fresh meat, seafood, and poultry(Webster et al., 2014).
When cooking or eating, in the table on when baking adding salt should be avoided by
using other flavors in food such as herbs and spices (Strazzullo et al., 2009).
Reducing food portions since more food portion means more salt intake. Make sure you
prepare a small portion of your meal when at home and sometimes share with a friend to
avoid consuming the bigger amount of salts (Liem et al., 2011).
Rinse sodium from foods such as beans, vegetables, and tuna before eating. This will
help you reduce the amount of sodium content in your food.
There is a need to increase public awareness on effects of salts on their health. Bruce
Neal a Professor from UNSW Sydney and George Institute of Global Health says, "Most
of the actions trying to contain how much salt people eat have been about trying to
educate people and tell them about the problem. And that's important, but the food
environment means that's not desperately helpful. It has almost no impact at
all"(McKenzie-Mohr, 2011).
The government should come up with policies which restrict processing industries using
too much salt on the processed food but rather reduce it to a required amount.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PUBLIC HEALTH 5
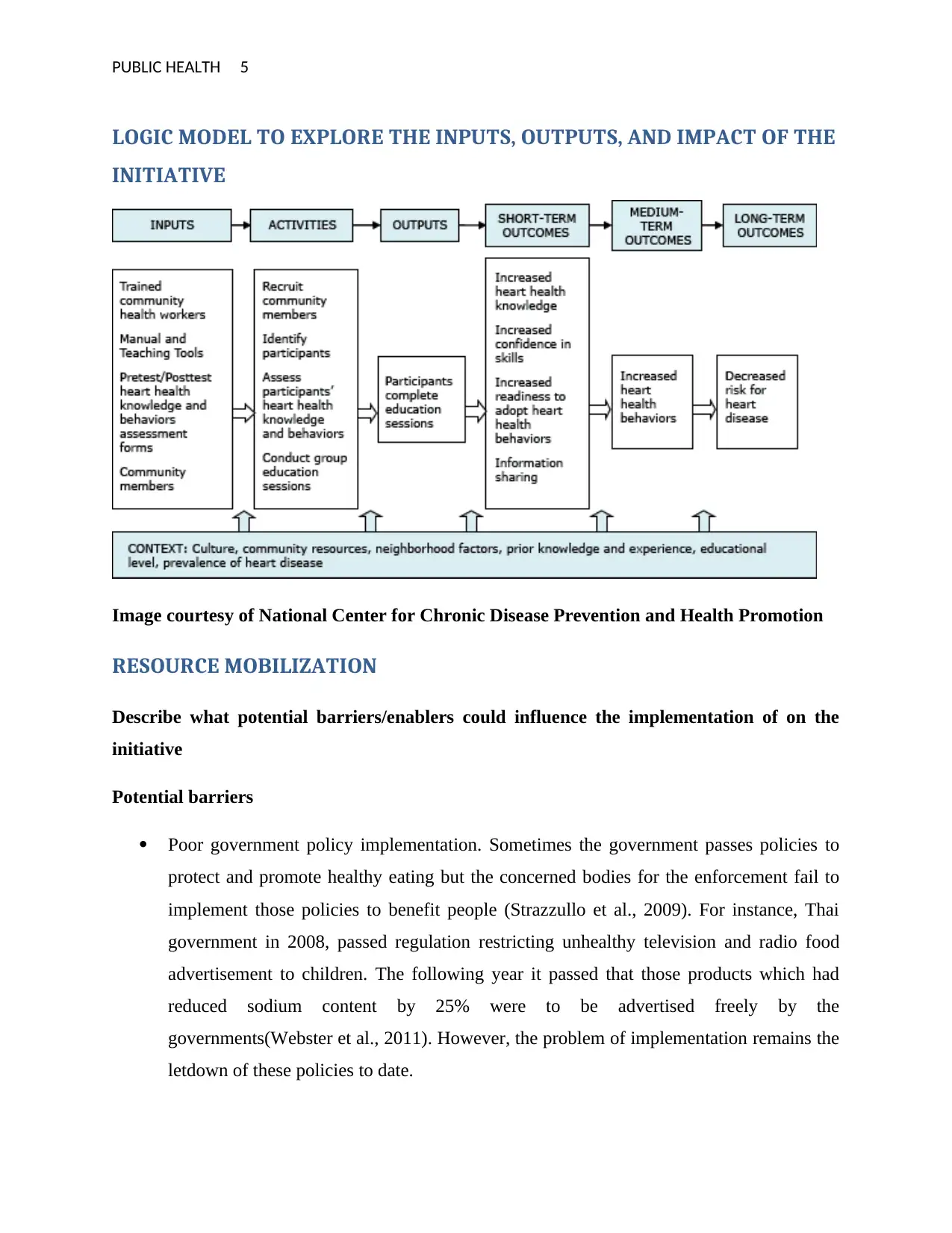
LOGIC MODEL TO EXPLORE THE INPUTS, OUTPUTS, AND IMPACT OF THE
INITIATIVE
Image courtesy of National Center for Chronic Disease Prevention and Health Promotion
RESOURCE MOBILIZATION
Describe what potential barriers/enablers could influence the implementation of on the
initiative
Potential barriers
Poor government policy implementation. Sometimes the government passes policies to
protect and promote healthy eating but the concerned bodies for the enforcement fail to
implement those policies to benefit people (Strazzullo et al., 2009). For instance, Thai
government in 2008, passed regulation restricting unhealthy television and radio food
advertisement to children. The following year it passed that those products which had
reduced sodium content by 25% were to be advertised freely by the
governments(Webster et al., 2011). However, the problem of implementation remains the
letdown of these policies to date.
LOGIC MODEL TO EXPLORE THE INPUTS, OUTPUTS, AND IMPACT OF THE
INITIATIVE
Image courtesy of National Center for Chronic Disease Prevention and Health Promotion
RESOURCE MOBILIZATION
Describe what potential barriers/enablers could influence the implementation of on the
initiative
Potential barriers
Poor government policy implementation. Sometimes the government passes policies to
protect and promote healthy eating but the concerned bodies for the enforcement fail to
implement those policies to benefit people (Strazzullo et al., 2009). For instance, Thai
government in 2008, passed regulation restricting unhealthy television and radio food
advertisement to children. The following year it passed that those products which had
reduced sodium content by 25% were to be advertised freely by the
governments(Webster et al., 2011). However, the problem of implementation remains the
letdown of these policies to date.
PUBLIC HEALTH 6
Poor governance of systems which would support the implementation(Webster et al.,
2011).
Social factors such as lack of effective communication and insufficient involvements
with stakeholders (government and NGOs) as well as lack of strengthened social support
networks(Webster et al., 2011).
Organizational structure instability as a result of a change of executive-level leaders may
be a major blow for implementing the initiatives(Strazzullo et al., 2009).
Unclear roles boundaries and too many levels of management (NGO, GO and AC)
Executive's leadership inability of achieving the implementation (25% SFS: NGO and
AC; RTA: NGO and AC),(Joffres et al., 2013).
Government and NGOs insufficient funding for the implementation of policy (25% SFS:
NGO, GO, AC and PV; RTA: GO),(Joffres et al., 2013).
The enablers
Individual support from the government officials(25% SFS: NGO, GO and AC; RTA:
NGO and AC.
If the policy is compatible with the intended users’ context (AC and GO).
Mechanisms for good financial management tracking funding means available to
support implementation (GO, NGO and PV)
If there are strong inter-organization links across and within sectors (25% SFS: GO
and PV; RTA: GO, NGO and AC)
Strategies to identify barriers and enablers of salt reduction initiative
Public education
What is most disturbing is that problems associated with salt intake affect both children
and adults in the developing and developed countries. Although salt reduction has been shown to
reduce cardiovascular occurrences many people are not interested in a salt reduction or are not
aware of the needs to reduce their salt intake(Beaglehole et al., 2011). This endangers their lives
even more and puts more burdens on the government and private sectors which are concerned
about the reduction of risks associated with the increased salt intake(Joffres et al., 2013). The
Poor governance of systems which would support the implementation(Webster et al.,
2011).
Social factors such as lack of effective communication and insufficient involvements
with stakeholders (government and NGOs) as well as lack of strengthened social support
networks(Webster et al., 2011).
Organizational structure instability as a result of a change of executive-level leaders may
be a major blow for implementing the initiatives(Strazzullo et al., 2009).
Unclear roles boundaries and too many levels of management (NGO, GO and AC)
Executive's leadership inability of achieving the implementation (25% SFS: NGO and
AC; RTA: NGO and AC),(Joffres et al., 2013).
Government and NGOs insufficient funding for the implementation of policy (25% SFS:
NGO, GO, AC and PV; RTA: GO),(Joffres et al., 2013).
The enablers
Individual support from the government officials(25% SFS: NGO, GO and AC; RTA:
NGO and AC.
If the policy is compatible with the intended users’ context (AC and GO).
Mechanisms for good financial management tracking funding means available to
support implementation (GO, NGO and PV)
If there are strong inter-organization links across and within sectors (25% SFS: GO
and PV; RTA: GO, NGO and AC)
Strategies to identify barriers and enablers of salt reduction initiative
Public education
What is most disturbing is that problems associated with salt intake affect both children
and adults in the developing and developed countries. Although salt reduction has been shown to
reduce cardiovascular occurrences many people are not interested in a salt reduction or are not
aware of the needs to reduce their salt intake(Beaglehole et al., 2011). This endangers their lives
even more and puts more burdens on the government and private sectors which are concerned
about the reduction of risks associated with the increased salt intake(Joffres et al., 2013). The
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PUBLIC HEALTH 7
motivation for individuals in general population to decrease salt consumption through engaging
them in sustained behavior change has been found difficult and challenging(He, Pombo-
Rodrigues & MacGregor, 2014). General population behavior concerning the willingness to
change must have a solid understanding and is important for targeted research and successful salt
reduction initiatives(Wang &Labarthe, 2011). The public education on salt reduction started in
1970’s sponsored by Lung, Blood and National Heart Institute when they were backing
education campaign for national blood pressure (Sørensen et al., 2012). Since then major efforts
have been put in place to educate people on the importance of salt intake reduction(Joffres et al.,
2013). Consumer awareness since raised from 12% in 1979 to 48% in 1984, though there has
been difficult in sustaining these gains and raising fears that they may have reduced significantly
higher in the recent years(He, Pombo-Rodrigues &MacGregor, 2014). For instance, in 2002,
there was a reduction of these gains to 39%.
Other problems hindering the reduction of salt intake in the low percentage of consumer
actively trying to reduce this behavior and has never increased beyond 33% which is linked with
several Americans not aware of their own sodium intake(Strazzullo et al., 2009). Education is the
easiest and most inexpensive strategy to implement; it requires the reduction of salt composition
in the processed and packaged foods in order for it to be effective. This means the creation of
awareness through education implementation initiative may not be the better option if there is a
continued salt composition in these foods.
Individual dietary counseling
Counseling is important in changing attitudes, beliefs, and knowledge of salt intake habits
since it is hard to estimate and monitor salt intake. There is a need for better understanding in
developing interventions implementable on a large population scale, focusing on the barriers and
motivators to change(World Health Organization, 2010). Individual dietary counseling can be
done by the physician or healthcare providers as evident in smoking cessation and weight control
that shows the significant role they play in reinforcing these and maintenance of these
habits(Chen et al., 2009). To make effective the role of these physicians is to increase their skills,
knowledge, optimistic approach towards sodium decline and other ways of life changes(Joffres
motivation for individuals in general population to decrease salt consumption through engaging
them in sustained behavior change has been found difficult and challenging(He, Pombo-
Rodrigues & MacGregor, 2014). General population behavior concerning the willingness to
change must have a solid understanding and is important for targeted research and successful salt
reduction initiatives(Wang &Labarthe, 2011). The public education on salt reduction started in
1970’s sponsored by Lung, Blood and National Heart Institute when they were backing
education campaign for national blood pressure (Sørensen et al., 2012). Since then major efforts
have been put in place to educate people on the importance of salt intake reduction(Joffres et al.,
2013). Consumer awareness since raised from 12% in 1979 to 48% in 1984, though there has
been difficult in sustaining these gains and raising fears that they may have reduced significantly
higher in the recent years(He, Pombo-Rodrigues &MacGregor, 2014). For instance, in 2002,
there was a reduction of these gains to 39%.
Other problems hindering the reduction of salt intake in the low percentage of consumer
actively trying to reduce this behavior and has never increased beyond 33% which is linked with
several Americans not aware of their own sodium intake(Strazzullo et al., 2009). Education is the
easiest and most inexpensive strategy to implement; it requires the reduction of salt composition
in the processed and packaged foods in order for it to be effective. This means the creation of
awareness through education implementation initiative may not be the better option if there is a
continued salt composition in these foods.
Individual dietary counseling
Counseling is important in changing attitudes, beliefs, and knowledge of salt intake habits
since it is hard to estimate and monitor salt intake. There is a need for better understanding in
developing interventions implementable on a large population scale, focusing on the barriers and
motivators to change(World Health Organization, 2010). Individual dietary counseling can be
done by the physician or healthcare providers as evident in smoking cessation and weight control
that shows the significant role they play in reinforcing these and maintenance of these
habits(Chen et al., 2009). To make effective the role of these physicians is to increase their skills,
knowledge, optimistic approach towards sodium decline and other ways of life changes(Joffres
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PUBLIC HEALTH 8
et al., 2013). A barrier to this initiative is that clinicians might be restricted by the difficulty with
patients’ adjustment behavior in their present nutrition supply(Pimenta et al., 2009).
Food labeling
Despite the effort of the governments and WHO to curb the salt intake amongst worlds’
population through industrial food labeling initiative, there remain excuses from these branded
industries that manufacture processed foods(Fleischhacker et al., 2011). According to the
chairman of Consensus Action on Salt and Health, Graham MacGregor “we feel that the food
industry has done a terrific job but it still has further much to go, and we would like to see
branded manufacturers taking a much more entrepreneurial and not come up with these excuses
all the time” (Joffres et al., 2013). Gregory states that, the brands apart from technical issues may
be too conservative in regard to changing consumers taste panel in their recipes (Chen et al.,
2009). However, regarding tastes of consumers, Gregory says, “10% reduction cannot be
detected by the salt tastes receptors.”Issues surrounding taste has been the main barrier to
changing the amount of salt in the processed food with companies wondering whether to
formulate CASH requirements for products with no salt at all. Gregory says that “We don’t
accept that taste is a big problem without evidence” (He, Li & MacGregor, 2013). The major
setback for this is that labeling systems such as Nutritional Facts Panel are poorly designed
hence wrong information may be experienced.
Coordinated, voluntary industry sodium reduction
Calls for industrial voluntary action for salt reduction have been futile in countries like
the US. There is evidence that shows that for this to be effective companies should be held
responsible for their pledges toward coordinated voluntary action and backed by authoritative
bodies. Data from the Public Interest Center for Science found that only 5% reduction in the
amount of sodium in packed food from 1983 to 2004 where from 1994 the levels
increased(Batcagan-Abueg et al., 2013). To achieve salt reduction of the restaurant and packaged
food in this initiative there should be there should be no limitation of consumer choice and
acceptance(Liem, Miremadi&Keast, 2011). The amount of salt added back with the salt shaker is
said to be only a portion and this means if people are given food with small amount of sodium in
their food they will, therefore, adapt slowly to average salt needed(Aburto et al., 2013).
et al., 2013). A barrier to this initiative is that clinicians might be restricted by the difficulty with
patients’ adjustment behavior in their present nutrition supply(Pimenta et al., 2009).
Food labeling
Despite the effort of the governments and WHO to curb the salt intake amongst worlds’
population through industrial food labeling initiative, there remain excuses from these branded
industries that manufacture processed foods(Fleischhacker et al., 2011). According to the
chairman of Consensus Action on Salt and Health, Graham MacGregor “we feel that the food
industry has done a terrific job but it still has further much to go, and we would like to see
branded manufacturers taking a much more entrepreneurial and not come up with these excuses
all the time” (Joffres et al., 2013). Gregory states that, the brands apart from technical issues may
be too conservative in regard to changing consumers taste panel in their recipes (Chen et al.,
2009). However, regarding tastes of consumers, Gregory says, “10% reduction cannot be
detected by the salt tastes receptors.”Issues surrounding taste has been the main barrier to
changing the amount of salt in the processed food with companies wondering whether to
formulate CASH requirements for products with no salt at all. Gregory says that “We don’t
accept that taste is a big problem without evidence” (He, Li & MacGregor, 2013). The major
setback for this is that labeling systems such as Nutritional Facts Panel are poorly designed
hence wrong information may be experienced.
Coordinated, voluntary industry sodium reduction
Calls for industrial voluntary action for salt reduction have been futile in countries like
the US. There is evidence that shows that for this to be effective companies should be held
responsible for their pledges toward coordinated voluntary action and backed by authoritative
bodies. Data from the Public Interest Center for Science found that only 5% reduction in the
amount of sodium in packed food from 1983 to 2004 where from 1994 the levels
increased(Batcagan-Abueg et al., 2013). To achieve salt reduction of the restaurant and packaged
food in this initiative there should be there should be no limitation of consumer choice and
acceptance(Liem, Miremadi&Keast, 2011). The amount of salt added back with the salt shaker is
said to be only a portion and this means if people are given food with small amount of sodium in
their food they will, therefore, adapt slowly to average salt needed(Aburto et al., 2013).
PUBLIC HEALTH 9
The other possibility for this initiative becoming effective is through government creating
processed food database on daily basis, 24-hour urine collection periodic measurements of
peoples’ sodium intake and company reports (Strazzullo et al., 2009). The 2010 targets have
today been achieved by many UK companies which saw approximated 10% drop intake of
sodium from 2000 to 2008(Webster et al., 2014). This initiative was adopted by National Salt
Reduction Initiative for the United States which aimed in achieving sodium content reduction to
between 20% and by 25% reduction in restaurant and packed foods by 2014(Bibbins-Domingo,
2010). This target for sodium reduction has been achieved by some large national players such as
Target, Subway, and Kraft with a total of 28 packaged food and restaurant companies
today(Webster et al., 2014). The committed companies and restaurant are asked to give a report
on their progress in nutrition information every target year(Strazzullo et al., 2009). The other
application by the NSRI is the creation of national restaurant and packaged food databases which
help to assess the amount of sodium independently.
There are advantages that are associated with this initiative and they include; one, less
controversial compared to regulation, for both public and food companies. Two, it makes
companies be responsible for their commitments (Webster et al., 2011). Three, it targets on the
content of sodium in restaurant and packaged food, instead of shopper decision, and four, it is a
gradual system of minimizing intake, enabling adjustments and differentiating of tastes for
various types food, while consumer variety and choices remain unchanged (Fleischhacker et al.,
2011).
This initiative has a challenge of voluntary initiative not requiring the industry to
participate making sodium reduction limited to the number of companies involved. It is also not
compulsory for the commitment even if it is publicized and monitored(Joffres et al., 2013). This
initiative has been found to face a lot of opposition for instance in US groups like Salt Institute
and Centre for Consumer Freedom and opposed NSRI.
Government and private sector food procurement policies
The UK’s program for salt reduction reduced average salt intake in its population and
also boosted consumer awareness. There are however significant challenges that remain towards
achieving an average salt intake of 6g/d among its population which is recommended by UK’s
The other possibility for this initiative becoming effective is through government creating
processed food database on daily basis, 24-hour urine collection periodic measurements of
peoples’ sodium intake and company reports (Strazzullo et al., 2009). The 2010 targets have
today been achieved by many UK companies which saw approximated 10% drop intake of
sodium from 2000 to 2008(Webster et al., 2014). This initiative was adopted by National Salt
Reduction Initiative for the United States which aimed in achieving sodium content reduction to
between 20% and by 25% reduction in restaurant and packed foods by 2014(Bibbins-Domingo,
2010). This target for sodium reduction has been achieved by some large national players such as
Target, Subway, and Kraft with a total of 28 packaged food and restaurant companies
today(Webster et al., 2014). The committed companies and restaurant are asked to give a report
on their progress in nutrition information every target year(Strazzullo et al., 2009). The other
application by the NSRI is the creation of national restaurant and packaged food databases which
help to assess the amount of sodium independently.
There are advantages that are associated with this initiative and they include; one, less
controversial compared to regulation, for both public and food companies. Two, it makes
companies be responsible for their commitments (Webster et al., 2011). Three, it targets on the
content of sodium in restaurant and packaged food, instead of shopper decision, and four, it is a
gradual system of minimizing intake, enabling adjustments and differentiating of tastes for
various types food, while consumer variety and choices remain unchanged (Fleischhacker et al.,
2011).
This initiative has a challenge of voluntary initiative not requiring the industry to
participate making sodium reduction limited to the number of companies involved. It is also not
compulsory for the commitment even if it is publicized and monitored(Joffres et al., 2013). This
initiative has been found to face a lot of opposition for instance in US groups like Salt Institute
and Centre for Consumer Freedom and opposed NSRI.
Government and private sector food procurement policies
The UK’s program for salt reduction reduced average salt intake in its population and
also boosted consumer awareness. There are however significant challenges that remain towards
achieving an average salt intake of 6g/d among its population which is recommended by UK’s
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PUBLIC HEALTH 10
scientific advisory committee on nutrition (Pimenta et al., 2009). Other worlds have started
implementing this approach as the UK demonstrated the success of this program(Puska&Ståhl,
2010). This initiative is achievable by the government if it includes sodium standards in their
procurement policies, which also means private and non-profit institutions doing the same.
One of the best methods which seem to have the potentiality to this initiative is the US
government annual purchases of a large amount of food, of more than $800 million in its
program for feeding employees in military and 1.9 billion pounds used for purchasing for
feeding school lunch program(Petersen, 2009). There are also food purchases for schools, child-
care centers, senior centers, correctional institutions, and other institutions by both local and state
governments(Stolarz-Skrzypek,2011). If these programs require that inclusion of specific sodium
standard is adhered to, it can contribute towards achieving voluntary coordinated reductions
through demanding low quantity of sodium products and there is not a single company which
can stand to lose this opportunity(Fleischhacker et al., 2011).
Policies for procurement increases demand low sodium food, high healthy food, which
ensures food industries adhere to it when producing and marketing their products as well as
ensuring that people depending on government for food can get low sodium and balanced
diet(Legetic& Campbell,2011). This initiative has however very small impact as it targets only a
fraction of countries population making it not to be fully reliable.
FDA regulations
This approach has a big advantage which is, FDA approves food staffs prepared with
additives lacking GRAS status before marketing, modifying. Despite this advantage, it is not
clear if it will implement IOM recommendation which required regulation of the content of salt
in both packed and restaurant food to decrease sodium intake(He, Li&MacGregor, 2013). There
is a likelihood of opposition by food industries in case of any changes to regulatory
environments because the modification would affect large numbers of the industry(Wyness,
Butriss&Stanner, 2012). However, FDA’s implementing this recommendation is likely to take
years to draft and be approved.
scientific advisory committee on nutrition (Pimenta et al., 2009). Other worlds have started
implementing this approach as the UK demonstrated the success of this program(Puska&Ståhl,
2010). This initiative is achievable by the government if it includes sodium standards in their
procurement policies, which also means private and non-profit institutions doing the same.
One of the best methods which seem to have the potentiality to this initiative is the US
government annual purchases of a large amount of food, of more than $800 million in its
program for feeding employees in military and 1.9 billion pounds used for purchasing for
feeding school lunch program(Petersen, 2009). There are also food purchases for schools, child-
care centers, senior centers, correctional institutions, and other institutions by both local and state
governments(Stolarz-Skrzypek,2011). If these programs require that inclusion of specific sodium
standard is adhered to, it can contribute towards achieving voluntary coordinated reductions
through demanding low quantity of sodium products and there is not a single company which
can stand to lose this opportunity(Fleischhacker et al., 2011).
Policies for procurement increases demand low sodium food, high healthy food, which
ensures food industries adhere to it when producing and marketing their products as well as
ensuring that people depending on government for food can get low sodium and balanced
diet(Legetic& Campbell,2011). This initiative has however very small impact as it targets only a
fraction of countries population making it not to be fully reliable.
FDA regulations
This approach has a big advantage which is, FDA approves food staffs prepared with
additives lacking GRAS status before marketing, modifying. Despite this advantage, it is not
clear if it will implement IOM recommendation which required regulation of the content of salt
in both packed and restaurant food to decrease sodium intake(He, Li&MacGregor, 2013). There
is a likelihood of opposition by food industries in case of any changes to regulatory
environments because the modification would affect large numbers of the industry(Wyness,
Butriss&Stanner, 2012). However, FDA’s implementing this recommendation is likely to take
years to draft and be approved.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PUBLIC HEALTH 11
IMPLEMENTATION/OUTCOME ASSESSMENT
Evaluating the initiative using qualitative study design
Objectives
It is important to reduce sodium contents in our diet for public health intervention that
will help to reduce chronic disease and blood pressure. To understand how Americans population
purchases are influenced by how they perceive sodium contents in diet will inform future
strategies of sodium reduction.
Design
The contemporary qualitative study has used an in-depth questionnaire to adults
‘population in exploring peoples’ knowledge, understanding of food purchasing behavior and
food labels with regards to dietary sodium.
Setting
United States
Subjects
A convenient sample of 80 adult supermarket shoppers
Results
Detailed analyses of the receipts showed that American adults lacked knowledge that is
necessary for recognizing and adjust their own intake of salt and could not interpret the existing
food labels in regards to dietary sodium.
Conclusion
There is further weight added from the findings to calls for food labels that do not need
knowledge or numerical skills with highlighting the needs for peoples’ based interventions for
public health. This approach would be complemented by the education for Americans people on
the health benefit of reducing sodium contents.
IMPLEMENTATION/OUTCOME ASSESSMENT
Evaluating the initiative using qualitative study design
Objectives
It is important to reduce sodium contents in our diet for public health intervention that
will help to reduce chronic disease and blood pressure. To understand how Americans population
purchases are influenced by how they perceive sodium contents in diet will inform future
strategies of sodium reduction.
Design
The contemporary qualitative study has used an in-depth questionnaire to adults
‘population in exploring peoples’ knowledge, understanding of food purchasing behavior and
food labels with regards to dietary sodium.
Setting
United States
Subjects
A convenient sample of 80 adult supermarket shoppers
Results
Detailed analyses of the receipts showed that American adults lacked knowledge that is
necessary for recognizing and adjust their own intake of salt and could not interpret the existing
food labels in regards to dietary sodium.
Conclusion
There is further weight added from the findings to calls for food labels that do not need
knowledge or numerical skills with highlighting the needs for peoples’ based interventions for
public health. This approach would be complemented by the education for Americans people on
the health benefit of reducing sodium contents.
PUBLIC HEALTH 12
Describe which outcomes would be used to examine the impact of the initiative on the health priority
area
Cardiovascular diseases dropping from the current 17 million deaths reported per
year(Legetic& Campbell, 2011).
The decrease in high blood pressure among individuals who have raised blood pressure
and few or no new cases for high blood pressure reported as a result of sodium
consumption
Reduction of cases of heart diseases and stroke(Pelikan,2012).
Consumers becoming more cautious about reading food labels to choose from the one
with the required amount of sodium contents(Pimenta et al., 2009).
People starting to avoid using salt shakeups when eating (Trieu et al., 2015).
Reduced restaurant and processed food purchases.
Describe how these outcomes would be assessed
A total of 75 countries have a strategy for national salt reduction a double of the reported in 2010
Taxation on high salt foods (3)
Interventions in public institutions (54)(Strazzullo et al., 2009).
Front-of-pack labeling schemes (31)
consumer education (71)
Establishment of sodium content targets for foods (39)
industry engagement to reformulate products (n = 61)
Regulations related reduction of salt intakes like front pack labeling, mandatory targets,
taxation, and food procurement policies have been implemented in over 33 countries.
Reductions in salt intake have been reported amongst populations in 12 countries, 19
having reduced content of salt in foods and 6 improvements in consumer attitude,
behavior, and knowledge on salt(Strazzullo et al., 2009).
Describe which outcomes would be used to examine the impact of the initiative on the health priority
area
Cardiovascular diseases dropping from the current 17 million deaths reported per
year(Legetic& Campbell, 2011).
The decrease in high blood pressure among individuals who have raised blood pressure
and few or no new cases for high blood pressure reported as a result of sodium
consumption
Reduction of cases of heart diseases and stroke(Pelikan,2012).
Consumers becoming more cautious about reading food labels to choose from the one
with the required amount of sodium contents(Pimenta et al., 2009).
People starting to avoid using salt shakeups when eating (Trieu et al., 2015).
Reduced restaurant and processed food purchases.
Describe how these outcomes would be assessed
A total of 75 countries have a strategy for national salt reduction a double of the reported in 2010
Taxation on high salt foods (3)
Interventions in public institutions (54)(Strazzullo et al., 2009).
Front-of-pack labeling schemes (31)
consumer education (71)
Establishment of sodium content targets for foods (39)
industry engagement to reformulate products (n = 61)
Regulations related reduction of salt intakes like front pack labeling, mandatory targets,
taxation, and food procurement policies have been implemented in over 33 countries.
Reductions in salt intake have been reported amongst populations in 12 countries, 19
having reduced content of salt in foods and 6 improvements in consumer attitude,
behavior, and knowledge on salt(Strazzullo et al., 2009).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.