Case Study: GORD - Aetiology, Pathophysiology, Nursing Care, Treatment
VerifiedAdded on 2022/10/01
|15
|3331
|208
Case Study
AI Summary
This case study focuses on a 48-year-old building manager, Mr. Seamus O’Neil, diagnosed with Gastro-oesophageal Reflux Disease (GORD). The study explores the aetiology of GORD, highlighting lifestyle factors like diet and stress as contributing causes, and discusses the pathophysiology, including the mechanisms of acid reflux and its impact on the oesophagus and other organs. It details various laboratory tests used for diagnosis and provides a comprehensive nursing care plan, covering nutritional considerations, elimination issues, and psychosocial aspects. The assignment also examines pharmacological treatments, including antacids, H-2-receptor blockers, and proton pump inhibitors, along with their potential side effects. The case study concludes with a summary of the disease, nursing interventions, and the importance of patient management.

Running head: CASE STUDY (GORD)
CASE STUDY (GORD)
Name of the Student
Name of the University
Author Note
CASE STUDY (GORD)
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
CASE STUDY (GORD)
Table of Contents
Introduction....................................................................................................................................2
Aetiology.........................................................................................................................................2
Pathophysiology and Clinical Manifestation...............................................................................2
Laboratory Tests............................................................................................................................4
Nursing care...................................................................................................................................4
Pharmacological treatment and Potential Side Effects of the Medications.............................5
Conclusion......................................................................................................................................6
Reference........................................................................................................................................7
CASE STUDY (GORD)
Table of Contents
Introduction....................................................................................................................................2
Aetiology.........................................................................................................................................2
Pathophysiology and Clinical Manifestation...............................................................................2
Laboratory Tests............................................................................................................................4
Nursing care...................................................................................................................................4
Pharmacological treatment and Potential Side Effects of the Medications.............................5
Conclusion......................................................................................................................................6
Reference........................................................................................................................................7
2
CASE STUDY (GORD)
Introduction
According to the case study, the case subject, Mr Seamus O’Neil who is a 48 year old
building manager diagnosed with Gastro-oesophageal reflux disease (GORD). This is a condition
in which the acid of the stomach of the person leaks out in oesophagus (Ness-Jensen, Hveem, El-
Serag & Lagergren, 2016). This condition primarily occurs due to loosening of ring muscles at
the bottom of the oesophagus. Because of this condition burning sensation in chest, acid reflux,
bloating, esophagitis, bad breath and other symptoms can be seen among the patients affected by
this disease.
Aetiology
GORD is one of the most prevalent gastrointestinal disorders in Australia, with about 10-
15% of the Australian population suffering from this disease due to the increase of improper
food habits causing widespread obesity and weakening of gastro-intestinal systems. GORD is
observed to have been affected by environmental causes and individual lifestyle habits as well.
Lifestyle habits like diet, sleep pattern, substance and alcohol abuse as well as medical
conditions including stomach abnormalities like lower oesophageal sphincter dysfunction and
pregnancy are some of the key risk factors for GORD.
The increased incorporation of fried, fatty food items, reduced and abnormal sleeping patterns as
well as substance and alcohol abuse tend to result in prolonged and constant incidence of acid
reflux by facilitating the untimely relaxing of the lower oesophageal sphincter (Ness-Jensen &
Lagergren, 2017).
CASE STUDY (GORD)
Introduction
According to the case study, the case subject, Mr Seamus O’Neil who is a 48 year old
building manager diagnosed with Gastro-oesophageal reflux disease (GORD). This is a condition
in which the acid of the stomach of the person leaks out in oesophagus (Ness-Jensen, Hveem, El-
Serag & Lagergren, 2016). This condition primarily occurs due to loosening of ring muscles at
the bottom of the oesophagus. Because of this condition burning sensation in chest, acid reflux,
bloating, esophagitis, bad breath and other symptoms can be seen among the patients affected by
this disease.
Aetiology
GORD is one of the most prevalent gastrointestinal disorders in Australia, with about 10-
15% of the Australian population suffering from this disease due to the increase of improper
food habits causing widespread obesity and weakening of gastro-intestinal systems. GORD is
observed to have been affected by environmental causes and individual lifestyle habits as well.
Lifestyle habits like diet, sleep pattern, substance and alcohol abuse as well as medical
conditions including stomach abnormalities like lower oesophageal sphincter dysfunction and
pregnancy are some of the key risk factors for GORD.
The increased incorporation of fried, fatty food items, reduced and abnormal sleeping patterns as
well as substance and alcohol abuse tend to result in prolonged and constant incidence of acid
reflux by facilitating the untimely relaxing of the lower oesophageal sphincter (Ness-Jensen &
Lagergren, 2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
CASE STUDY (GORD)
However, the severity of the acid reflux of GORD can be reduced by properly diagnosing the
disorder and taking effective medications like antacids and H-2-receptor blockers. Lifestyle
modifications like changing sleeping patterns, eating healthy, balanced diets as well as reducing
alcohol and smoking habits are long-term interventions for this disorder.
Thus, the food habits, imbalanced routines as well as occupational stress of Mr Seamus O’Neil
can be considered as the cause of this disease (Lam & Hart, 2017).
Pathophysiology and Clinical Manifestation
GORD is a complex disease that can be caused by the complex changes in the reflux
exposure, epithelial resistance and also the visceral sensitivity (Tack & Pandolfino, 2018). The
process of the reflux can be identified as the acidic leakage from the stomach to the oesophagus
and spreading the effects of the acidic reaction to other body organs. Increased and consistent
exposure to unhealthy foods having high fat content is the most common reason behind the
incidence of severe acid reflux. Other than an unbalanced diet, lifestyle choices and habits like
sleeping patterns and alcohol and drug addictions can also facilitate the process of the hiatal
hernia and severe acid reflux.
The increased incorporation of junk foods in daily diets of individuals has paved the way for the
observed surge in the individuals affected by GORD in recent years. The junk foods have been
observed to detrimentally affect the epithelial layer of the stomach and the oesophagus. These fat
enriched food items which tend to induce acid reflux reactions can thus be considered as the
primary cause of GORD. In-taking fatty and spicy food items can also hamper the visceral
sensitivity, along with detrimentally affecting the tissues in the stomach.
CASE STUDY (GORD)
However, the severity of the acid reflux of GORD can be reduced by properly diagnosing the
disorder and taking effective medications like antacids and H-2-receptor blockers. Lifestyle
modifications like changing sleeping patterns, eating healthy, balanced diets as well as reducing
alcohol and smoking habits are long-term interventions for this disorder.
Thus, the food habits, imbalanced routines as well as occupational stress of Mr Seamus O’Neil
can be considered as the cause of this disease (Lam & Hart, 2017).
Pathophysiology and Clinical Manifestation
GORD is a complex disease that can be caused by the complex changes in the reflux
exposure, epithelial resistance and also the visceral sensitivity (Tack & Pandolfino, 2018). The
process of the reflux can be identified as the acidic leakage from the stomach to the oesophagus
and spreading the effects of the acidic reaction to other body organs. Increased and consistent
exposure to unhealthy foods having high fat content is the most common reason behind the
incidence of severe acid reflux. Other than an unbalanced diet, lifestyle choices and habits like
sleeping patterns and alcohol and drug addictions can also facilitate the process of the hiatal
hernia and severe acid reflux.
The increased incorporation of junk foods in daily diets of individuals has paved the way for the
observed surge in the individuals affected by GORD in recent years. The junk foods have been
observed to detrimentally affect the epithelial layer of the stomach and the oesophagus. These fat
enriched food items which tend to induce acid reflux reactions can thus be considered as the
primary cause of GORD. In-taking fatty and spicy food items can also hamper the visceral
sensitivity, along with detrimentally affecting the tissues in the stomach.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
CASE STUDY (GORD)
The BMI of an individual can also be a risk factor for the incidence of GORD. Thus, the diet of
individuals plays a very crucial part in determining the severity of the incident acid reflux (Chen
& Brady, 2019). Thus, individuals with unhealthy food habits and limited effective maintenance
of physical health are the most vulnerable to this disease.
The pathophysiology of GORD thus relates to the development of the discomfort in the stomach
tissue and also the peripheral organ tissues so that the overflow of the acidic fluid and the reflux
as well (Menezes & Herbella, 2017). However, the physical activity and the healthy living
contexts are the factors that can also affect the optimal condition of the gastro-intestinal system.
The sensitivity of the tissues and also the development of the unwanted acidic fluid in the
stomach lead to the discomforting condition and also development of other discomforting
conditions as well and also leads to the condition of the severe damage on other organs as well.
According to Del Grande, Herbella, Bigatao, Abrao, Jardim and Patti (2016), it has been seen
that among the people with obstructive pulmonary disease the GORD affects also leads to the
development of the increased Trans-diaphragmatic Pressure. Hence, it can be stated that GORD
leads to the damage of other organs and create and extensive condition which should be stopped
in the early development of the disease.
Laboratory Tests
In order to help diagnose the condition of GORD in Mr O’Neil, several investigative tests
can be employed to determine the incidence as well as the extent of the Gastro-oesophageal
reflux. The diagnostic laboratory tests include blood tests which determine the acid ration of the
CASE STUDY (GORD)
The BMI of an individual can also be a risk factor for the incidence of GORD. Thus, the diet of
individuals plays a very crucial part in determining the severity of the incident acid reflux (Chen
& Brady, 2019). Thus, individuals with unhealthy food habits and limited effective maintenance
of physical health are the most vulnerable to this disease.
The pathophysiology of GORD thus relates to the development of the discomfort in the stomach
tissue and also the peripheral organ tissues so that the overflow of the acidic fluid and the reflux
as well (Menezes & Herbella, 2017). However, the physical activity and the healthy living
contexts are the factors that can also affect the optimal condition of the gastro-intestinal system.
The sensitivity of the tissues and also the development of the unwanted acidic fluid in the
stomach lead to the discomforting condition and also development of other discomforting
conditions as well and also leads to the condition of the severe damage on other organs as well.
According to Del Grande, Herbella, Bigatao, Abrao, Jardim and Patti (2016), it has been seen
that among the people with obstructive pulmonary disease the GORD affects also leads to the
development of the increased Trans-diaphragmatic Pressure. Hence, it can be stated that GORD
leads to the damage of other organs and create and extensive condition which should be stopped
in the early development of the disease.
Laboratory Tests
In order to help diagnose the condition of GORD in Mr O’Neil, several investigative tests
can be employed to determine the incidence as well as the extent of the Gastro-oesophageal
reflux. The diagnostic laboratory tests include blood tests which determine the acid ration of the
5
CASE STUDY (GORD)
body, which helps understand the severity of the acid refluxes. Doctors often suggest ultra-
sonography of the stomach of the patient along with bile and liver function tests which could
help determine the condition of the digestive system better (Genco et al., 2017). The healthcare
professionals will be able to assess the extent of the medical condition better, and provide the
patient with effective interventions in accordance with their age as well as medical history.
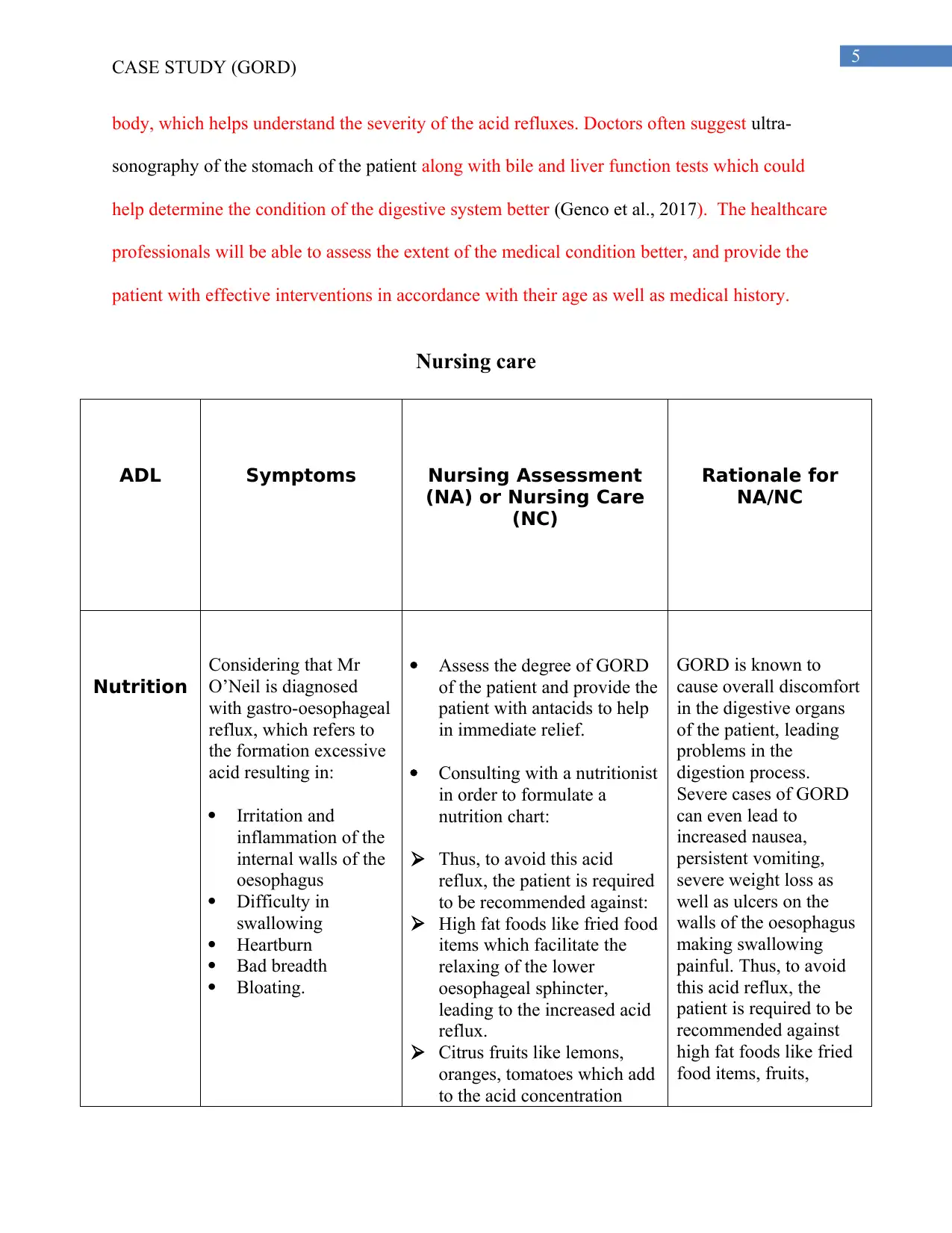
Nursing care
ADL Symptoms Nursing Assessment
(NA) or Nursing Care
(NC)
Rationale for
NA/NC
Nutrition
Considering that Mr
O’Neil is diagnosed
with gastro-oesophageal
reflux, which refers to
the formation excessive
acid resulting in:
Irritation and
inflammation of the
internal walls of the
oesophagus
Difficulty in
swallowing
Heartburn
Bad breadth
Bloating.
Assess the degree of GORD
of the patient and provide the
patient with antacids to help
in immediate relief.
Consulting with a nutritionist
in order to formulate a
nutrition chart:
Thus, to avoid this acid
reflux, the patient is required
to be recommended against:
High fat foods like fried food
items which facilitate the
relaxing of the lower
oesophageal sphincter,
leading to the increased acid
reflux.
Citrus fruits like lemons,
oranges, tomatoes which add
to the acid concentration
GORD is known to
cause overall discomfort
in the digestive organs
of the patient, leading
problems in the
digestion process.
Severe cases of GORD
can even lead to
increased nausea,
persistent vomiting,
severe weight loss as
well as ulcers on the
walls of the oesophagus
making swallowing
painful. Thus, to avoid
this acid reflux, the
patient is required to be
recommended against
high fat foods like fried
food items, fruits,
CASE STUDY (GORD)
body, which helps understand the severity of the acid refluxes. Doctors often suggest ultra-
sonography of the stomach of the patient along with bile and liver function tests which could
help determine the condition of the digestive system better (Genco et al., 2017). The healthcare
professionals will be able to assess the extent of the medical condition better, and provide the
patient with effective interventions in accordance with their age as well as medical history.
Nursing care
ADL Symptoms Nursing Assessment
(NA) or Nursing Care
(NC)
Rationale for
NA/NC
Nutrition
Considering that Mr
O’Neil is diagnosed
with gastro-oesophageal
reflux, which refers to
the formation excessive
acid resulting in:
Irritation and
inflammation of the
internal walls of the
oesophagus
Difficulty in
swallowing
Heartburn
Bad breadth
Bloating.
Assess the degree of GORD
of the patient and provide the
patient with antacids to help
in immediate relief.
Consulting with a nutritionist
in order to formulate a
nutrition chart:
Thus, to avoid this acid
reflux, the patient is required
to be recommended against:
High fat foods like fried food
items which facilitate the
relaxing of the lower
oesophageal sphincter,
leading to the increased acid
reflux.
Citrus fruits like lemons,
oranges, tomatoes which add
to the acid concentration
GORD is known to
cause overall discomfort
in the digestive organs
of the patient, leading
problems in the
digestion process.
Severe cases of GORD
can even lead to
increased nausea,
persistent vomiting,
severe weight loss as
well as ulcers on the
walls of the oesophagus
making swallowing
painful. Thus, to avoid
this acid reflux, the
patient is required to be
recommended against
high fat foods like fried
food items, fruits,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
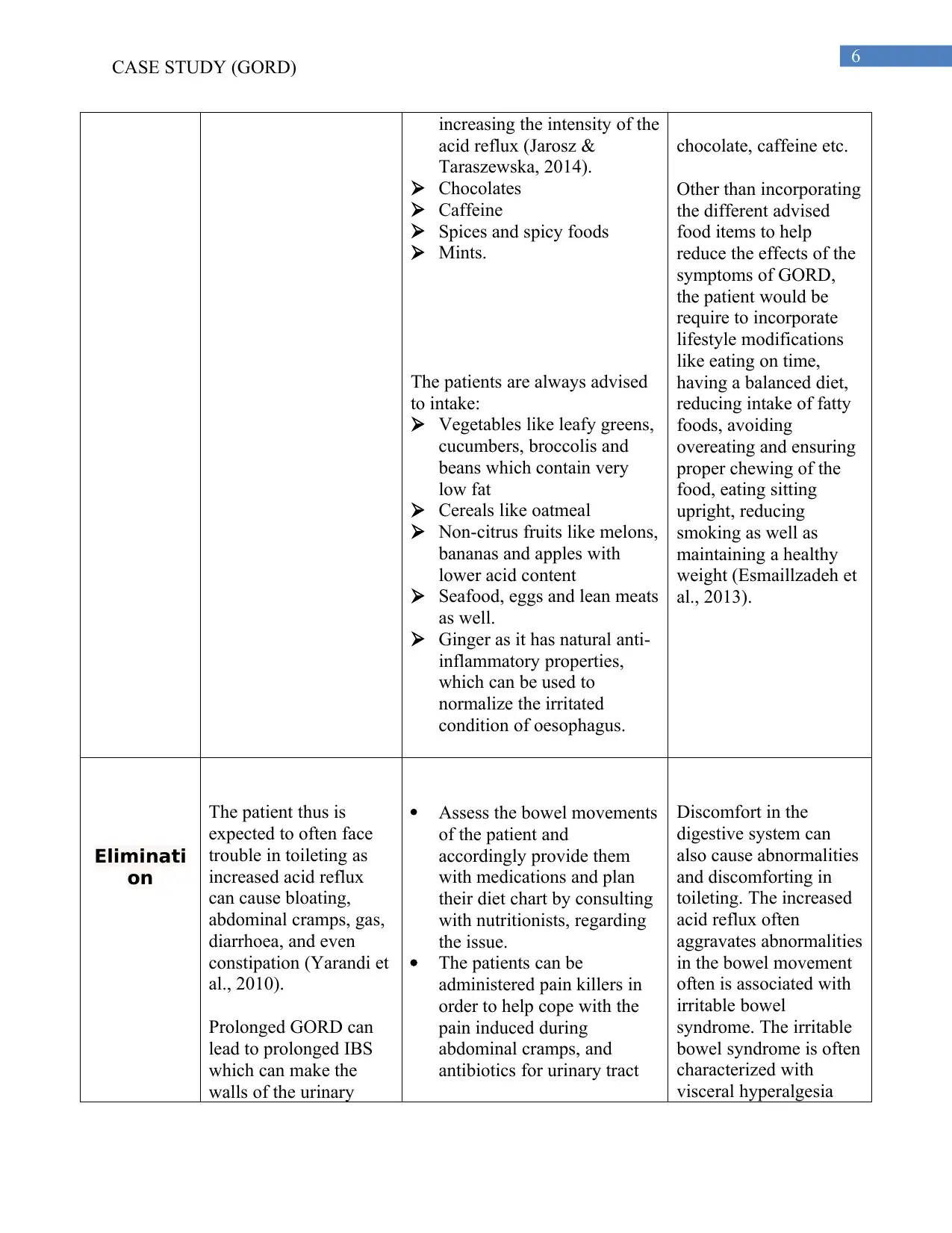
CASE STUDY (GORD)
increasing the intensity of the
acid reflux (Jarosz &
Taraszewska, 2014).
Chocolates
Caffeine
Spices and spicy foods
Mints.
The patients are always advised
to intake:
Vegetables like leafy greens,
cucumbers, broccolis and
beans which contain very
low fat
Cereals like oatmeal
Non-citrus fruits like melons,
bananas and apples with
lower acid content
Seafood, eggs and lean meats
as well.
Ginger as it has natural anti-
inflammatory properties,
which can be used to
normalize the irritated
condition of oesophagus.
chocolate, caffeine etc.
Other than incorporating
the different advised
food items to help
reduce the effects of the
symptoms of GORD,
the patient would be
require to incorporate
lifestyle modifications
like eating on time,
having a balanced diet,
reducing intake of fatty
foods, avoiding
overeating and ensuring
proper chewing of the
food, eating sitting
upright, reducing
smoking as well as
maintaining a healthy
weight (Esmaillzadeh et
al., 2013).
Eliminati
on
The patient thus is
expected to often face
trouble in toileting as
increased acid reflux
can cause bloating,
abdominal cramps, gas,
diarrhoea, and even
constipation (Yarandi et
al., 2010).
Prolonged GORD can
lead to prolonged IBS
which can make the
walls of the urinary
Assess the bowel movements
of the patient and
accordingly provide them
with medications and plan
their diet chart by consulting
with nutritionists, regarding
the issue.
The patients can be
administered pain killers in
order to help cope with the
pain induced during
abdominal cramps, and
antibiotics for urinary tract
Discomfort in the
digestive system can
also cause abnormalities
and discomforting in
toileting. The increased
acid reflux often
aggravates abnormalities
in the bowel movement
often is associated with
irritable bowel
syndrome. The irritable
bowel syndrome is often
characterized with
visceral hyperalgesia
CASE STUDY (GORD)
increasing the intensity of the
acid reflux (Jarosz &
Taraszewska, 2014).
Chocolates
Caffeine
Spices and spicy foods
Mints.
The patients are always advised
to intake:
Vegetables like leafy greens,
cucumbers, broccolis and
beans which contain very
low fat
Cereals like oatmeal
Non-citrus fruits like melons,
bananas and apples with
lower acid content
Seafood, eggs and lean meats
as well.
Ginger as it has natural anti-
inflammatory properties,
which can be used to
normalize the irritated
condition of oesophagus.
chocolate, caffeine etc.
Other than incorporating
the different advised
food items to help
reduce the effects of the
symptoms of GORD,
the patient would be
require to incorporate
lifestyle modifications
like eating on time,
having a balanced diet,
reducing intake of fatty
foods, avoiding
overeating and ensuring
proper chewing of the
food, eating sitting
upright, reducing
smoking as well as
maintaining a healthy
weight (Esmaillzadeh et
al., 2013).
Eliminati
on
The patient thus is
expected to often face
trouble in toileting as
increased acid reflux
can cause bloating,
abdominal cramps, gas,
diarrhoea, and even
constipation (Yarandi et
al., 2010).
Prolonged GORD can
lead to prolonged IBS
which can make the
walls of the urinary
Assess the bowel movements
of the patient and
accordingly provide them
with medications and plan
their diet chart by consulting
with nutritionists, regarding
the issue.
The patients can be
administered pain killers in
order to help cope with the
pain induced during
abdominal cramps, and
antibiotics for urinary tract
Discomfort in the
digestive system can
also cause abnormalities
and discomforting in
toileting. The increased
acid reflux often
aggravates abnormalities
in the bowel movement
often is associated with
irritable bowel
syndrome. The irritable
bowel syndrome is often
characterized with
visceral hyperalgesia
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
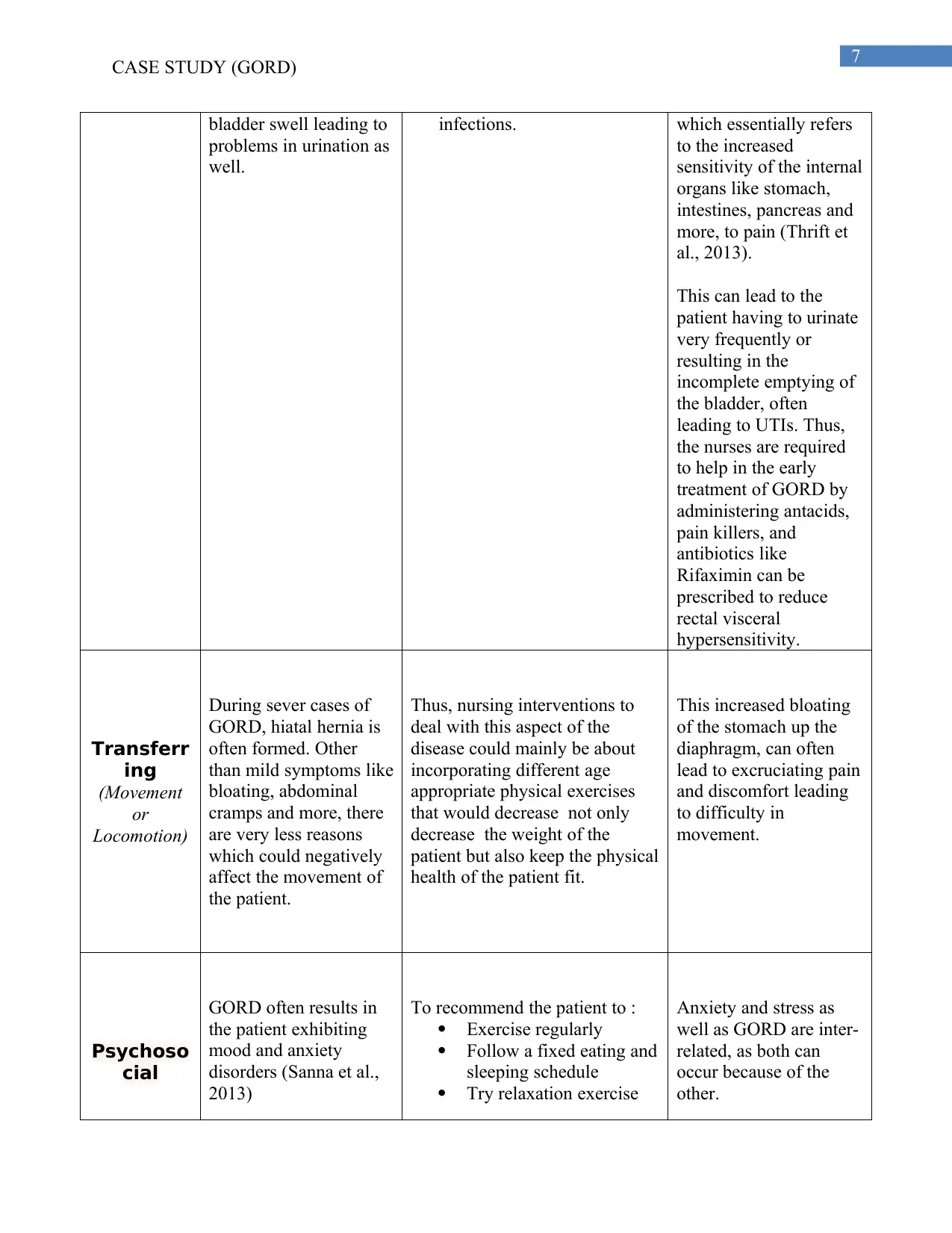
CASE STUDY (GORD)
bladder swell leading to
problems in urination as
well.
infections. which essentially refers
to the increased
sensitivity of the internal
organs like stomach,
intestines, pancreas and
more, to pain (Thrift et
al., 2013).
This can lead to the
patient having to urinate
very frequently or
resulting in the
incomplete emptying of
the bladder, often
leading to UTIs. Thus,
the nurses are required
to help in the early
treatment of GORD by
administering antacids,
pain killers, and
antibiotics like
Rifaximin can be
prescribed to reduce
rectal visceral
hypersensitivity.
Transferr
ing
(Movement
or
Locomotion)
During sever cases of
GORD, hiatal hernia is
often formed. Other
than mild symptoms like
bloating, abdominal
cramps and more, there
are very less reasons
which could negatively
affect the movement of
the patient.
Thus, nursing interventions to
deal with this aspect of the
disease could mainly be about
incorporating different age
appropriate physical exercises
that would decrease not only
decrease the weight of the
patient but also keep the physical
health of the patient fit.
This increased bloating
of the stomach up the
diaphragm, can often
lead to excruciating pain
and discomfort leading
to difficulty in
movement.
Psychoso
cial
GORD often results in
the patient exhibiting
mood and anxiety
disorders (Sanna et al.,
2013)
To recommend the patient to :
Exercise regularly
Follow a fixed eating and
sleeping schedule
Try relaxation exercise
Anxiety and stress as
well as GORD are inter-
related, as both can
occur because of the
other.
CASE STUDY (GORD)
bladder swell leading to
problems in urination as
well.
infections. which essentially refers
to the increased
sensitivity of the internal
organs like stomach,
intestines, pancreas and
more, to pain (Thrift et
al., 2013).
This can lead to the
patient having to urinate
very frequently or
resulting in the
incomplete emptying of
the bladder, often
leading to UTIs. Thus,
the nurses are required
to help in the early
treatment of GORD by
administering antacids,
pain killers, and
antibiotics like
Rifaximin can be
prescribed to reduce
rectal visceral
hypersensitivity.
Transferr
ing
(Movement
or
Locomotion)
During sever cases of
GORD, hiatal hernia is
often formed. Other
than mild symptoms like
bloating, abdominal
cramps and more, there
are very less reasons
which could negatively
affect the movement of
the patient.
Thus, nursing interventions to
deal with this aspect of the
disease could mainly be about
incorporating different age
appropriate physical exercises
that would decrease not only
decrease the weight of the
patient but also keep the physical
health of the patient fit.
This increased bloating
of the stomach up the
diaphragm, can often
lead to excruciating pain
and discomfort leading
to difficulty in
movement.
Psychoso
cial
GORD often results in
the patient exhibiting
mood and anxiety
disorders (Sanna et al.,
2013)
To recommend the patient to :
Exercise regularly
Follow a fixed eating and
sleeping schedule
Try relaxation exercise
Anxiety and stress as
well as GORD are inter-
related, as both can
occur because of the
other.
8
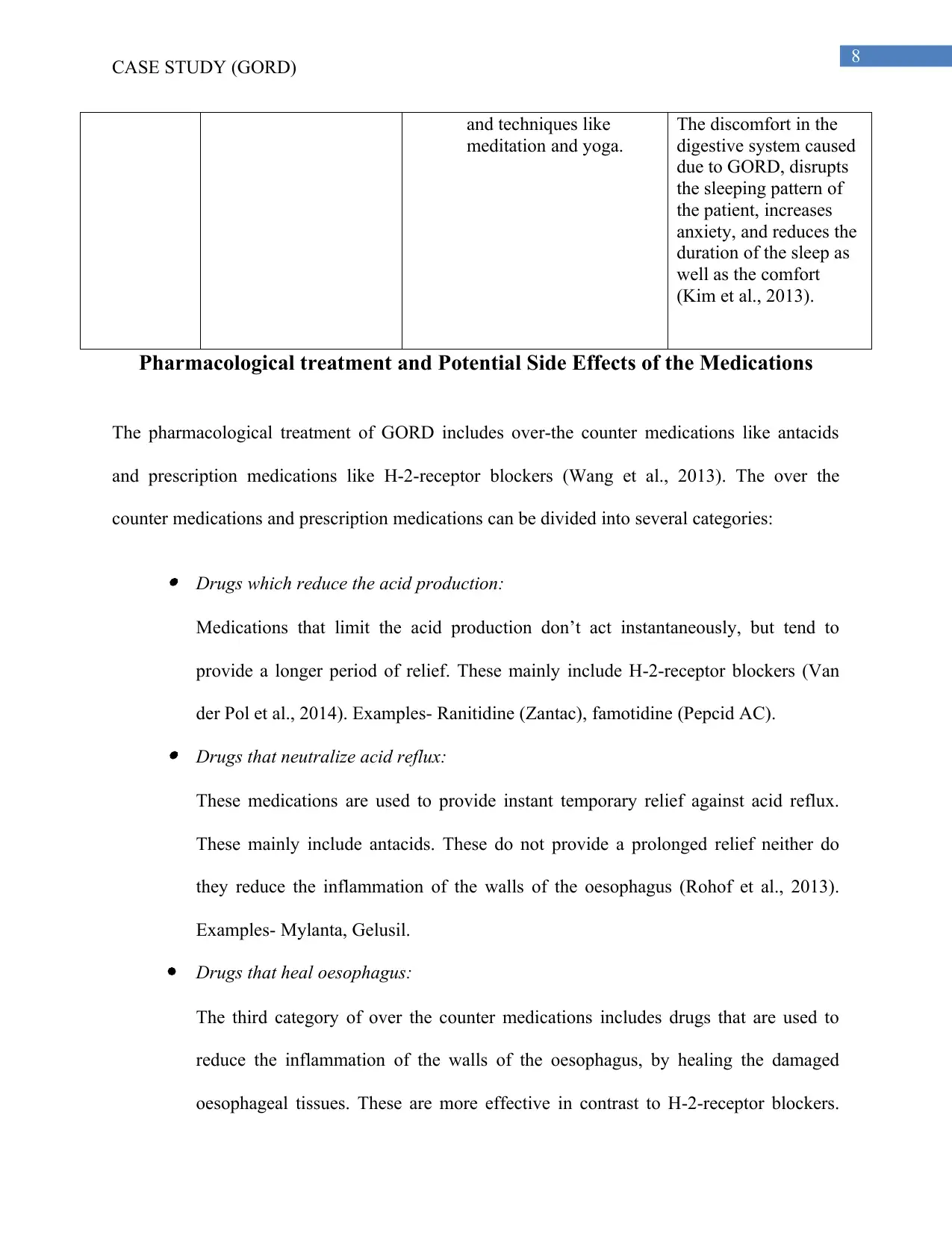
CASE STUDY (GORD)
and techniques like
meditation and yoga.
The discomfort in the
digestive system caused
due to GORD, disrupts
the sleeping pattern of
the patient, increases
anxiety, and reduces the
duration of the sleep as
well as the comfort
(Kim et al., 2013).
Pharmacological treatment and Potential Side Effects of the Medications
The pharmacological treatment of GORD includes over-the counter medications like antacids
and prescription medications like H-2-receptor blockers (Wang et al., 2013). The over the
counter medications and prescription medications can be divided into several categories:
Drugs which reduce the acid production:
Medications that limit the acid production don’t act instantaneously, but tend to
provide a longer period of relief. These mainly include H-2-receptor blockers (Van
der Pol et al., 2014). Examples- Ranitidine (Zantac), famotidine (Pepcid AC). Drugs that neutralize acid reflux:
These medications are used to provide instant temporary relief against acid reflux.
These mainly include antacids. These do not provide a prolonged relief neither do
they reduce the inflammation of the walls of the oesophagus (Rohof et al., 2013).
Examples- Mylanta, Gelusil.
Drugs that heal oesophagus:
The third category of over the counter medications includes drugs that are used to
reduce the inflammation of the walls of the oesophagus, by healing the damaged
oesophageal tissues. These are more effective in contrast to H-2-receptor blockers.
CASE STUDY (GORD)
and techniques like
meditation and yoga.
The discomfort in the
digestive system caused
due to GORD, disrupts
the sleeping pattern of
the patient, increases
anxiety, and reduces the
duration of the sleep as
well as the comfort
(Kim et al., 2013).
Pharmacological treatment and Potential Side Effects of the Medications
The pharmacological treatment of GORD includes over-the counter medications like antacids
and prescription medications like H-2-receptor blockers (Wang et al., 2013). The over the
counter medications and prescription medications can be divided into several categories:
Drugs which reduce the acid production:
Medications that limit the acid production don’t act instantaneously, but tend to
provide a longer period of relief. These mainly include H-2-receptor blockers (Van
der Pol et al., 2014). Examples- Ranitidine (Zantac), famotidine (Pepcid AC). Drugs that neutralize acid reflux:
These medications are used to provide instant temporary relief against acid reflux.
These mainly include antacids. These do not provide a prolonged relief neither do
they reduce the inflammation of the walls of the oesophagus (Rohof et al., 2013).
Examples- Mylanta, Gelusil.
Drugs that heal oesophagus:
The third category of over the counter medications includes drugs that are used to
reduce the inflammation of the walls of the oesophagus, by healing the damaged
oesophageal tissues. These are more effective in contrast to H-2-receptor blockers.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
CASE STUDY (GORD)
These mainly include proton pump inhibitors (Dean et al., 2004). Example-
lansoprazole, omeprazole.
Improving condition of lower oesophageal sphincter:
These medications help strengthen the lower oesophageal sphincter and help reduce
the frequency of the relaxations of the muscle. Example- Baclofen.
The potential side effects of these pharmacological means are as follows:
H-2-receptor blockers –
Prolonged use might increase the risk of bone fractures and vitamin –B12 deficiency. Antacids –
Extended use can cause side effects like diarrhoea, stomach discomfort, and even
kidney problems. Proton Pump Inhibitors –
These medications can lead to side effects like diarrhoea, nausea, increased risk of
bone fractures, headaches, and vitamin B-12 deficiency (Wang et al., 2013). Medications for strengthening lower oesophageal sphincter -
These muscle relaxers, if overused can lead to nausea and extreme fatigue (Wang et
al., 2013).
CASE STUDY (GORD)
These mainly include proton pump inhibitors (Dean et al., 2004). Example-
lansoprazole, omeprazole.
Improving condition of lower oesophageal sphincter:
These medications help strengthen the lower oesophageal sphincter and help reduce
the frequency of the relaxations of the muscle. Example- Baclofen.
The potential side effects of these pharmacological means are as follows:
H-2-receptor blockers –
Prolonged use might increase the risk of bone fractures and vitamin –B12 deficiency. Antacids –
Extended use can cause side effects like diarrhoea, stomach discomfort, and even
kidney problems. Proton Pump Inhibitors –
These medications can lead to side effects like diarrhoea, nausea, increased risk of
bone fractures, headaches, and vitamin B-12 deficiency (Wang et al., 2013). Medications for strengthening lower oesophageal sphincter -
These muscle relaxers, if overused can lead to nausea and extreme fatigue (Wang et
al., 2013).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
CASE STUDY (GORD)
Conclusion
It is concluded that burning sensation in chest, acid reflux, bloating, esophagitis, bad breath and
other symptoms can be seen among the patients affected by this disease.
The healthcare professionals thus are required to incorporate lifestyle modifications, balanced
diet plans, sleeping patterns and pharmaceutical means to help cope with the painful inflamed
esophagus and the increased acid reflux. Many pharmacological methods and medications can be
employed like antacids, proton and H-2-receptor blockers to treat GORD.
CASE STUDY (GORD)
Conclusion
It is concluded that burning sensation in chest, acid reflux, bloating, esophagitis, bad breath and
other symptoms can be seen among the patients affected by this disease.
The healthcare professionals thus are required to incorporate lifestyle modifications, balanced
diet plans, sleeping patterns and pharmaceutical means to help cope with the painful inflamed
esophagus and the increased acid reflux. Many pharmacological methods and medications can be
employed like antacids, proton and H-2-receptor blockers to treat GORD.
11
CASE STUDY (GORD)
Reference
Chen, J., & Brady, P. (2019). Gastroesophageal reflux disease: Pathophysiology, diagnosis, and
treatment. Gastroenterology Nursing, 42(1), 20-28. DOI:
10.1097/SGA.0000000000000359
Dean, B. B., Gano Jr, A. D., Knight, K., Ofman, J. J., & Fass, R. (2004). Effectiveness of proton
pump inhibitors in nonerosive reflux disease. Clinical Gastroenterology and
Hepatology, 2(8), 656-664. Retrieved from: https://doi.org/10.1016/S1542-
3565(04)00288-5
Del Grande, L. M., Herbella, F. A., Bigatao, A. M., Abrao, H., Jardim, J. R., & Patti, M. G.
(2016). Pathophysiology of gastroesophageal reflux in patients with chronic pulmonary
obstructive disease is linked to an increased transdiaphragmatic pressure gradient and not
to a defective esophagogastric barrier. Journal of Gastrointestinal Surgery, 20(1), 104-
110. DOI 10.1007/s11605-015-2955-4
Esmaillzadeh, A., Keshteli, A. H., Feizi, A., Zaribaf, F., Feinle‐Bisset, C., & Adibi, P. (2013).
Patterns of diet‐related practices and prevalence of gastro‐esophageal reflux
disease. Neurogastroenterology & Motility, 25(10), 831-e638. Retrieved from:
https://doi.org/10.1111/nmo.12192
Genco, A., Soricelli, E., Casella, G., Maselli, R., Castagneto-Gissey, L., Di Lorenzo, N., &
Basso, N. (2017). Gastroesophageal reflux disease and Barrett’s esophagus after
laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication.
Surgery for Obesity and Related Diseases, 13(4), 568-574. Retrieved from
http://dx.doi.org/10.1016/j.soard.2016.11.029
CASE STUDY (GORD)
Reference
Chen, J., & Brady, P. (2019). Gastroesophageal reflux disease: Pathophysiology, diagnosis, and
treatment. Gastroenterology Nursing, 42(1), 20-28. DOI:
10.1097/SGA.0000000000000359
Dean, B. B., Gano Jr, A. D., Knight, K., Ofman, J. J., & Fass, R. (2004). Effectiveness of proton
pump inhibitors in nonerosive reflux disease. Clinical Gastroenterology and
Hepatology, 2(8), 656-664. Retrieved from: https://doi.org/10.1016/S1542-
3565(04)00288-5
Del Grande, L. M., Herbella, F. A., Bigatao, A. M., Abrao, H., Jardim, J. R., & Patti, M. G.
(2016). Pathophysiology of gastroesophageal reflux in patients with chronic pulmonary
obstructive disease is linked to an increased transdiaphragmatic pressure gradient and not
to a defective esophagogastric barrier. Journal of Gastrointestinal Surgery, 20(1), 104-
110. DOI 10.1007/s11605-015-2955-4
Esmaillzadeh, A., Keshteli, A. H., Feizi, A., Zaribaf, F., Feinle‐Bisset, C., & Adibi, P. (2013).
Patterns of diet‐related practices and prevalence of gastro‐esophageal reflux
disease. Neurogastroenterology & Motility, 25(10), 831-e638. Retrieved from:
https://doi.org/10.1111/nmo.12192
Genco, A., Soricelli, E., Casella, G., Maselli, R., Castagneto-Gissey, L., Di Lorenzo, N., &
Basso, N. (2017). Gastroesophageal reflux disease and Barrett’s esophagus after
laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication.
Surgery for Obesity and Related Diseases, 13(4), 568-574. Retrieved from
http://dx.doi.org/10.1016/j.soard.2016.11.029
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.