Exploring Guillain Barre Syndrome: Symptoms, Diagnosis, and Treatment
VerifiedAdded on 2023/06/05
|11
|2904
|104
Report
AI Summary
This report provides a comprehensive overview of Guillain Barre Syndrome (GBS), an acute infection affecting the peripheral nervous system. It discusses the increasing need for effective treatment techniques, including home-based physical therapy to enhance flexibility and muscle strength. The paper details the signs and symptoms of GBS, such as muscle weakness, impaired function, and potential paralysis, emphasizing the difficulty in recognizing the infection in its early stages. It covers the mechanism of GBS, its various forms, prevalence rates globally (including higher risk in the US military), risk factors like Campylobacter jejuni infection and HIV/AIDS, and diagnostic methods including spinal taps, electromyography, and nerve conduction studies. Management and treatment strategies such as plasma exchange, immunoglobulin therapy, and ventilator support for severe cases are also discussed, highlighting the importance of supportive care and complication management. The report concludes by noting that while many patients recover, fatigue can persist, and severe cases may result in long-term paralysis.

Running Head: GUILLAIN BARRE SYNDROME
Name:
Institution Affiliation:
Instructor:
Course:
Date:
Name:
Institution Affiliation:
Instructor:
Course:
Date:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
GUILLAIN BARRE SYNDROME 2
Abstract
The healthcare system across the world is faced with increased incidence and prevalence
of Guillain Barre Syndrome (GBS) which is an acute infection, and it mostly affects the
peripheral nervous system. There is an increasing need to make better utilization of the treatment
techniques which are available for treatment of this infection. Development of home-based
physical therapy which enhances flexibility and muscle strength can be used to reduce the
hospital burden but also deliver better medication and treatment outcomes. The purpose of this
paper is to help all individuals to be able to understand GBS infection, the signs deeply, and
symptoms which are patient may experience in case they are infected by this infection and
prevalence of the disease.
Introduction
Guillain Barre Syndrome is uncommon type of infection which occurs mostly to
individuals who were previously healthy. GBS is an acute infection that affects the peripheral
nervous and in rare cases it can affect the motor or cranial nerves. GBS does not produce any
warning and it is considered an inflammatory condition which can lead to progressive muscle
weakness and in case a patient does not seek medical attention it can lead paralysis. It is very
difficult to recognize this infection from viral infection mostly in its early stages (Willison,
Jacobs & Van Doorn, 2016). It is very rare to find patients suffering from this illness in
emergency departments. Inflammation of the peripheral nerves affect the legs and harms of a
patient resulting into weakness, impaired function and feeling of limb paralysis which can
happen with or without any pain (Ansar & Valadi, 2015). Though it is a rare infection it can
affect individual of all ages. GBS is not a single infection, this is because it is made up several
variations which can be differentiated by their signs and symptoms, severity and the extent of the
Abstract
The healthcare system across the world is faced with increased incidence and prevalence
of Guillain Barre Syndrome (GBS) which is an acute infection, and it mostly affects the
peripheral nervous system. There is an increasing need to make better utilization of the treatment
techniques which are available for treatment of this infection. Development of home-based
physical therapy which enhances flexibility and muscle strength can be used to reduce the
hospital burden but also deliver better medication and treatment outcomes. The purpose of this
paper is to help all individuals to be able to understand GBS infection, the signs deeply, and
symptoms which are patient may experience in case they are infected by this infection and
prevalence of the disease.
Introduction
Guillain Barre Syndrome is uncommon type of infection which occurs mostly to
individuals who were previously healthy. GBS is an acute infection that affects the peripheral
nervous and in rare cases it can affect the motor or cranial nerves. GBS does not produce any
warning and it is considered an inflammatory condition which can lead to progressive muscle
weakness and in case a patient does not seek medical attention it can lead paralysis. It is very
difficult to recognize this infection from viral infection mostly in its early stages (Willison,
Jacobs & Van Doorn, 2016). It is very rare to find patients suffering from this illness in
emergency departments. Inflammation of the peripheral nerves affect the legs and harms of a
patient resulting into weakness, impaired function and feeling of limb paralysis which can
happen with or without any pain (Ansar & Valadi, 2015). Though it is a rare infection it can
affect individual of all ages. GBS is not a single infection, this is because it is made up several
variations which can be differentiated by their signs and symptoms, severity and the extent of the
GUILLAIN BARRE SYNDROME 3
inflammatory phase. For healthcare professionals to be in position to handle this infection, they
should be familiar with the mimics and variants to effectively be able to diagnose this illness
(Wijdicks & Klein, 2017). This paper focuses on signs and symptoms of GBS, prevalence, risk
factor of the infection, pathophysiology, management and treatment of the illness.
Mechanism of the Guillain Barre Syndrome
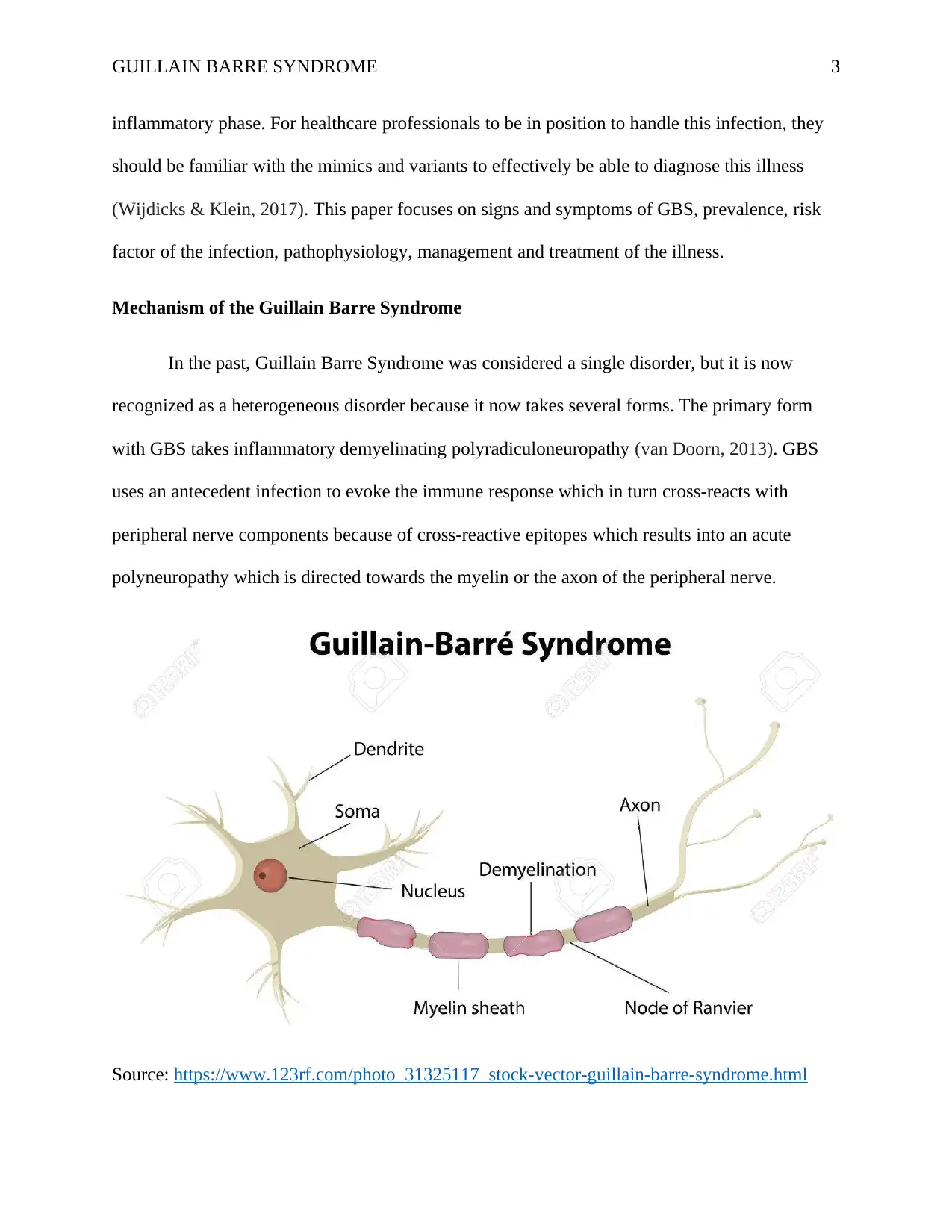
In the past, Guillain Barre Syndrome was considered a single disorder, but it is now
recognized as a heterogeneous disorder because it now takes several forms. The primary form
with GBS takes inflammatory demyelinating polyradiculoneuropathy (van Doorn, 2013). GBS
uses an antecedent infection to evoke the immune response which in turn cross-reacts with
peripheral nerve components because of cross-reactive epitopes which results into an acute
polyneuropathy which is directed towards the myelin or the axon of the peripheral nerve.
Source: https://www.123rf.com/photo_31325117_stock-vector-guillain-barre-syndrome.html
inflammatory phase. For healthcare professionals to be in position to handle this infection, they
should be familiar with the mimics and variants to effectively be able to diagnose this illness
(Wijdicks & Klein, 2017). This paper focuses on signs and symptoms of GBS, prevalence, risk
factor of the infection, pathophysiology, management and treatment of the illness.
Mechanism of the Guillain Barre Syndrome
In the past, Guillain Barre Syndrome was considered a single disorder, but it is now
recognized as a heterogeneous disorder because it now takes several forms. The primary form
with GBS takes inflammatory demyelinating polyradiculoneuropathy (van Doorn, 2013). GBS
uses an antecedent infection to evoke the immune response which in turn cross-reacts with
peripheral nerve components because of cross-reactive epitopes which results into an acute
polyneuropathy which is directed towards the myelin or the axon of the peripheral nerve.
Source: https://www.123rf.com/photo_31325117_stock-vector-guillain-barre-syndrome.html
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
GUILLAIN BARRE SYNDROME 4
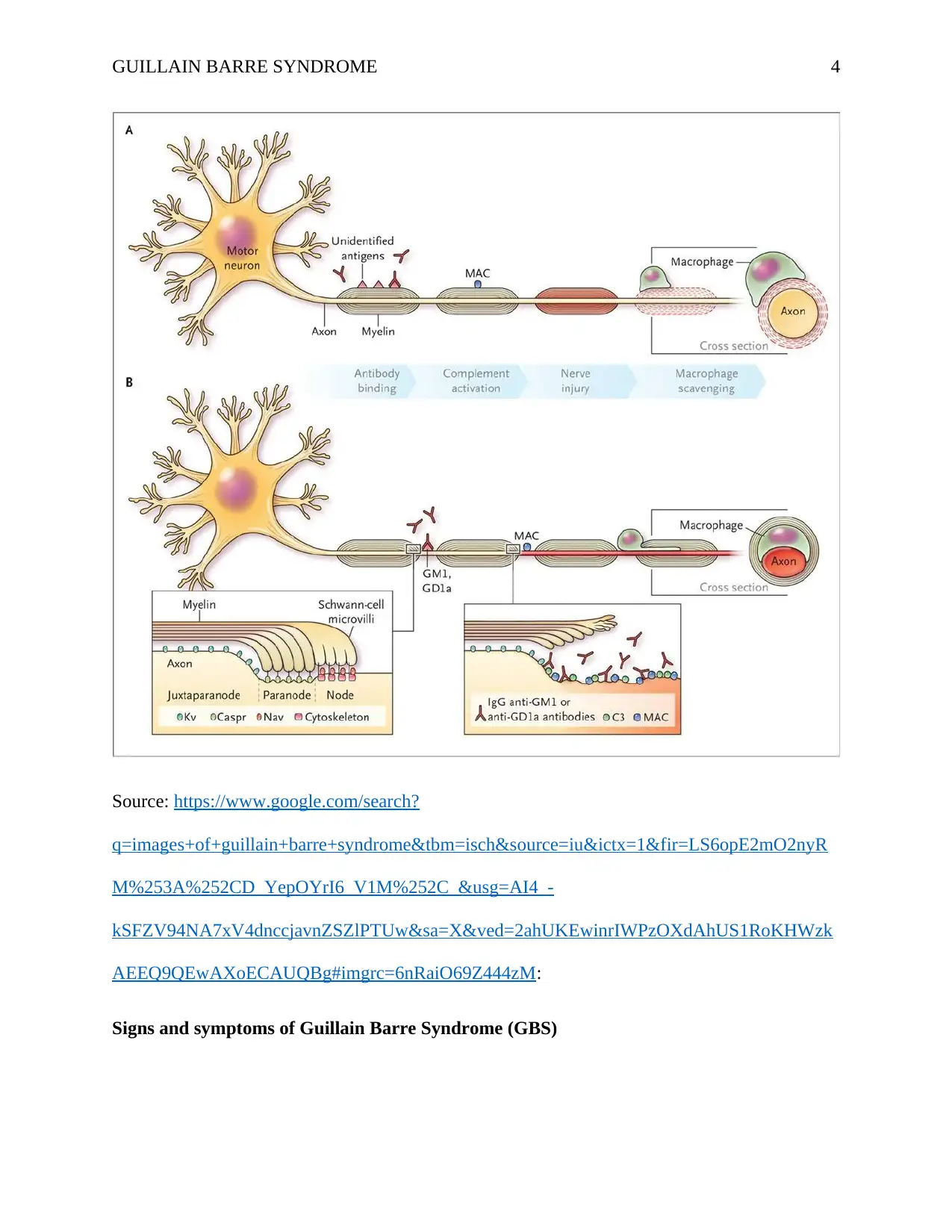
Source: https://www.google.com/search?
q=images+of+guillain+barre+syndrome&tbm=isch&source=iu&ictx=1&fir=LS6opE2mO2nyR
M%253A%252CD_YepOYrI6_V1M%252C_&usg=AI4_-
kSFZV94NA7xV4dnccjavnZSZlPTUw&sa=X&ved=2ahUKEwinrIWPzOXdAhUS1RoKHWzk
AEEQ9QEwAXoECAUQBg#imgrc=6nRaiO69Z444zM:
Signs and symptoms of Guillain Barre Syndrome (GBS)
Source: https://www.google.com/search?
q=images+of+guillain+barre+syndrome&tbm=isch&source=iu&ictx=1&fir=LS6opE2mO2nyR
M%253A%252CD_YepOYrI6_V1M%252C_&usg=AI4_-
kSFZV94NA7xV4dnccjavnZSZlPTUw&sa=X&ved=2ahUKEwinrIWPzOXdAhUS1RoKHWzk
AEEQ9QEwAXoECAUQBg#imgrc=6nRaiO69Z444zM:
Signs and symptoms of Guillain Barre Syndrome (GBS)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
GUILLAIN BARRE SYNDROME 5
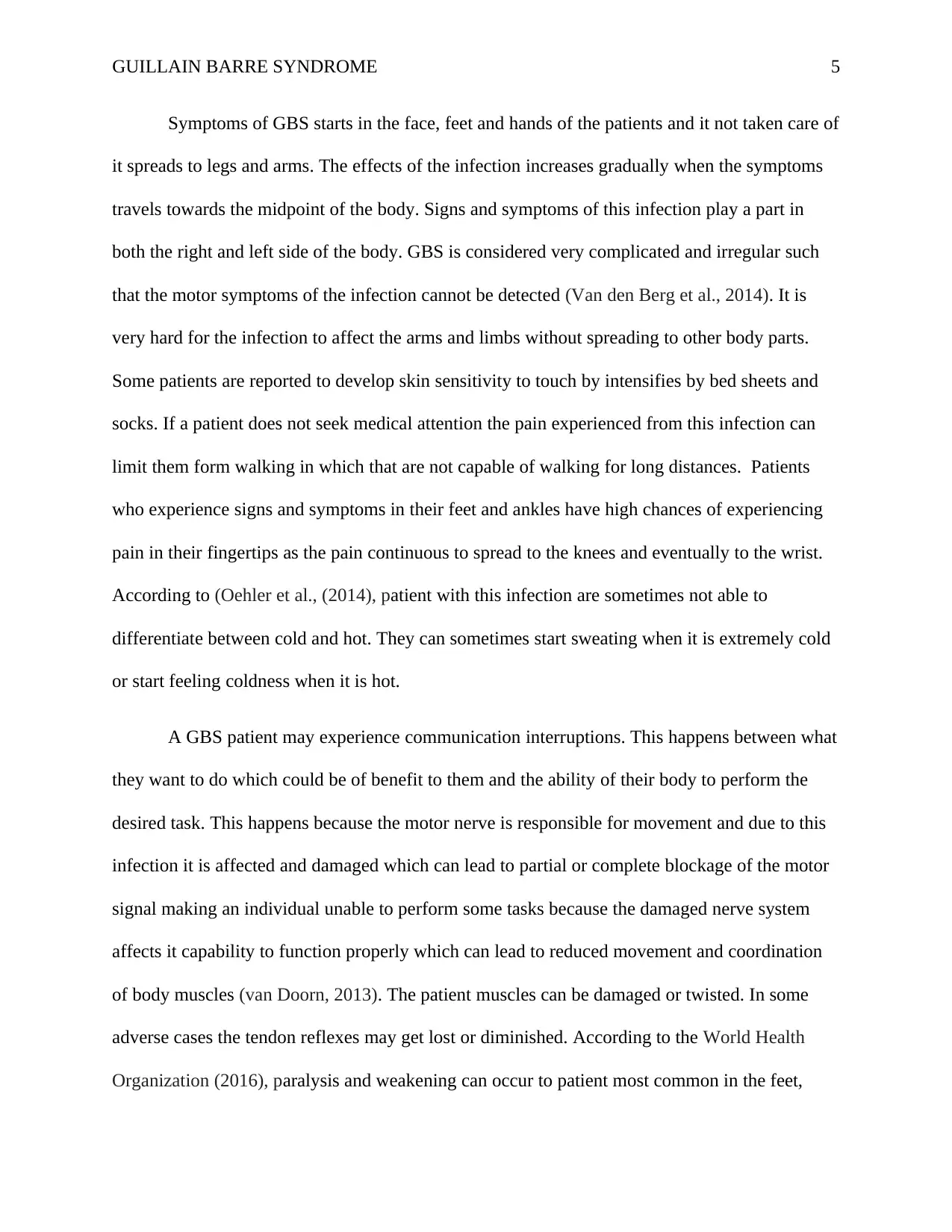
Symptoms of GBS starts in the face, feet and hands of the patients and it not taken care of
it spreads to legs and arms. The effects of the infection increases gradually when the symptoms
travels towards the midpoint of the body. Signs and symptoms of this infection play a part in
both the right and left side of the body. GBS is considered very complicated and irregular such
that the motor symptoms of the infection cannot be detected (Van den Berg et al., 2014). It is
very hard for the infection to affect the arms and limbs without spreading to other body parts.
Some patients are reported to develop skin sensitivity to touch by intensifies by bed sheets and
socks. If a patient does not seek medical attention the pain experienced from this infection can
limit them form walking in which that are not capable of walking for long distances. Patients
who experience signs and symptoms in their feet and ankles have high chances of experiencing
pain in their fingertips as the pain continuous to spread to the knees and eventually to the wrist.
According to (Oehler et al., (2014), patient with this infection are sometimes not able to
differentiate between cold and hot. They can sometimes start sweating when it is extremely cold
or start feeling coldness when it is hot.
A GBS patient may experience communication interruptions. This happens between what
they want to do which could be of benefit to them and the ability of their body to perform the
desired task. This happens because the motor nerve is responsible for movement and due to this
infection it is affected and damaged which can lead to partial or complete blockage of the motor
signal making an individual unable to perform some tasks because the damaged nerve system
affects it capability to function properly which can lead to reduced movement and coordination
of body muscles (van Doorn, 2013). The patient muscles can be damaged or twisted. In some
adverse cases the tendon reflexes may get lost or diminished. According to the World Health
Organization (2016), paralysis and weakening can occur to patient most common in the feet,
Symptoms of GBS starts in the face, feet and hands of the patients and it not taken care of
it spreads to legs and arms. The effects of the infection increases gradually when the symptoms
travels towards the midpoint of the body. Signs and symptoms of this infection play a part in
both the right and left side of the body. GBS is considered very complicated and irregular such
that the motor symptoms of the infection cannot be detected (Van den Berg et al., 2014). It is
very hard for the infection to affect the arms and limbs without spreading to other body parts.
Some patients are reported to develop skin sensitivity to touch by intensifies by bed sheets and
socks. If a patient does not seek medical attention the pain experienced from this infection can
limit them form walking in which that are not capable of walking for long distances. Patients
who experience signs and symptoms in their feet and ankles have high chances of experiencing
pain in their fingertips as the pain continuous to spread to the knees and eventually to the wrist.
According to (Oehler et al., (2014), patient with this infection are sometimes not able to
differentiate between cold and hot. They can sometimes start sweating when it is extremely cold
or start feeling coldness when it is hot.
A GBS patient may experience communication interruptions. This happens between what
they want to do which could be of benefit to them and the ability of their body to perform the
desired task. This happens because the motor nerve is responsible for movement and due to this
infection it is affected and damaged which can lead to partial or complete blockage of the motor
signal making an individual unable to perform some tasks because the damaged nerve system
affects it capability to function properly which can lead to reduced movement and coordination
of body muscles (van Doorn, 2013). The patient muscles can be damaged or twisted. In some
adverse cases the tendon reflexes may get lost or diminished. According to the World Health
Organization (2016), paralysis and weakening can occur to patient most common in the feet,
GUILLAIN BARRE SYNDROME 6
hands and face. The paralysis is persistent and keeps on rising to the patient and it can spread to
the rest of the limb (Musso, Nilles & Cao‐Lormeau, 2014). Arms of the patient becomes so weak
such that it becomes a problem for them to be able to lift objects. Weakness of the arms is
contributed by pain and involuntary muscle contractions. Constipation is another symptom of
this infection which happens due to condensed movement of the intestines.
Prevalence of Guillain Barre Syndrome (GBS)
GBS has been reported across the globe. The annual US incidence of GBS is 1 to 3
patient out of 100000 people (Willison, Jacobs & Van Doorn, 2016). The annual mean rate of
patients hospitalized in US has reported to be increasing with respect to age rarely affecting
young people below 15 years and highly in adult people. US military are at very high risk o been
infected by this infection as compared to the general population. Incidence of GBS occurrence in
the world is similar to US epidemiology without geographical clustering. AMAN and AMSON
type of GBS mostly occur in the northern part of china, Mexico am Japan which makes up to 5-
10% incidences of GBS reported in US. AIDP make up to 90% cases in Europe, North America
and developed countries. GBS infection has been reported throughout international community
across the globe (van den Berg, Bunschoten, van Doorn & Jacobs, 2013). GBS affects male
mostly as compared to female with a ratio of 1.5:1. For male victims then infection is mostly
common in older patients. Approximately 80% patients suffering from GBS have the capability
to walk independently for 6 months of the infection and 60% of the patients are able to recover
completely and attain motor strength in a period of 12 months. In 2008 epidemiology study
reported a 2-12% mortality rates of patients with GBS despite ICU management.
hands and face. The paralysis is persistent and keeps on rising to the patient and it can spread to
the rest of the limb (Musso, Nilles & Cao‐Lormeau, 2014). Arms of the patient becomes so weak
such that it becomes a problem for them to be able to lift objects. Weakness of the arms is
contributed by pain and involuntary muscle contractions. Constipation is another symptom of
this infection which happens due to condensed movement of the intestines.
Prevalence of Guillain Barre Syndrome (GBS)
GBS has been reported across the globe. The annual US incidence of GBS is 1 to 3
patient out of 100000 people (Willison, Jacobs & Van Doorn, 2016). The annual mean rate of
patients hospitalized in US has reported to be increasing with respect to age rarely affecting
young people below 15 years and highly in adult people. US military are at very high risk o been
infected by this infection as compared to the general population. Incidence of GBS occurrence in
the world is similar to US epidemiology without geographical clustering. AMAN and AMSON
type of GBS mostly occur in the northern part of china, Mexico am Japan which makes up to 5-
10% incidences of GBS reported in US. AIDP make up to 90% cases in Europe, North America
and developed countries. GBS infection has been reported throughout international community
across the globe (van den Berg, Bunschoten, van Doorn & Jacobs, 2013). GBS affects male
mostly as compared to female with a ratio of 1.5:1. For male victims then infection is mostly
common in older patients. Approximately 80% patients suffering from GBS have the capability
to walk independently for 6 months of the infection and 60% of the patients are able to recover
completely and attain motor strength in a period of 12 months. In 2008 epidemiology study
reported a 2-12% mortality rates of patients with GBS despite ICU management.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
GUILLAIN BARRE SYNDROME 7
Risk factors of Guillain Barre Syndrome (GBS)
The main cause of GBS is still unknown. However according to center for disease control
and prevention (CDC) about two-thirds of individual infected by GBS develop it after they have
been sick with respiratory problems or diarrhea. This suggests that people with poor immune
system are at very high risk of been infected by GBS (Salmon et al., 2013). Campylobacter jejuni
infection is another risk factor which is associated with GBS. This infection is the most cause of
diarrhea in many countries across the globe and it is termed as a major risk factor for GBS. The
bacteria of campylobacter is mostly found in undercooked food mostly poultry. Individuals
suffering from HIV/AIDS are highly exposed to GBS. This happens because AIDS makes their
immune system very weak making them susceptible to other infections and GBS can be one of
these infections (van den Berg et al., 2013). All people are capable of getting infected by GBs
but older adults and men are at very high risk of this infection. This happens to older people
because as individuals age, there immune system becomes weak and they are not in position to
fight infections (Nyati & Nyati, 2013). Healthcare professionals believes that viral and bacterial
infection are capable of changing the way in which nerve systems reacts to peripheral nerves
(Salmon et al., 2013).
Pathophysiology/diagnosis of Guillain Barre Syndrome
Guillain Barre Syndrome is very difficult to pathogenesis and diagnose at very early
stages. This happens because the sign and symptom of the infection are similar to those of other
neurological infection wand they may vary from person to person. Healthcare professionals
recommends the following to be done to patient infected by this disorder (McNair, 2013). Spinal
tap the first method in which healthcare professionals withdraws a small amount of fluid from
the patient’s lower back. Physicians then tests the fluid for a specific type of change which
Risk factors of Guillain Barre Syndrome (GBS)
The main cause of GBS is still unknown. However according to center for disease control
and prevention (CDC) about two-thirds of individual infected by GBS develop it after they have
been sick with respiratory problems or diarrhea. This suggests that people with poor immune
system are at very high risk of been infected by GBS (Salmon et al., 2013). Campylobacter jejuni
infection is another risk factor which is associated with GBS. This infection is the most cause of
diarrhea in many countries across the globe and it is termed as a major risk factor for GBS. The
bacteria of campylobacter is mostly found in undercooked food mostly poultry. Individuals
suffering from HIV/AIDS are highly exposed to GBS. This happens because AIDS makes their
immune system very weak making them susceptible to other infections and GBS can be one of
these infections (van den Berg et al., 2013). All people are capable of getting infected by GBs
but older adults and men are at very high risk of this infection. This happens to older people
because as individuals age, there immune system becomes weak and they are not in position to
fight infections (Nyati & Nyati, 2013). Healthcare professionals believes that viral and bacterial
infection are capable of changing the way in which nerve systems reacts to peripheral nerves
(Salmon et al., 2013).
Pathophysiology/diagnosis of Guillain Barre Syndrome
Guillain Barre Syndrome is very difficult to pathogenesis and diagnose at very early
stages. This happens because the sign and symptom of the infection are similar to those of other
neurological infection wand they may vary from person to person. Healthcare professionals
recommends the following to be done to patient infected by this disorder (McNair, 2013). Spinal
tap the first method in which healthcare professionals withdraws a small amount of fluid from
the patient’s lower back. Physicians then tests the fluid for a specific type of change which
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
GUILLAIN BARRE SYNDROME 8
occurs if the person is suffering from GBS. Healthcare professionals can also use
electromyography in which they insert thin needles electrodes in the muscles of the patient.
Electrodes plays are very major role of measuring if nerve activities in the muscles are working
properly. Nerve condition studies is the third test which healthcare professionals carry out to
examine if a patient is affected by GBS (Nyati & Nyati, 2013). This test includes sticking small
discs of electrodes to the body of the patients. Healthcare professionals use minor electric shocks
to activate the nerve and measure how faster the signals have traveled along them. Lumber
puncture is the last pathophysiology of GBS used to remove some fluids around the spinal cord
through a needle which is inserted in the lower part of the spine.
Management and treatment of Guillain Barre Syndrome
In most cases patients with vital signs and symptoms of GBS are hospitalized so that
healthcare professionals can carefully monitor their progress and respond to medication and
treatments they are administering to them. The duration in which the patient spend in the hospital
vary from days to weeks depending on how critical their health status is in. the first type of
treatment which healthcare professionals can give to patients is plasma exchange in which blood
is drawn and plasma which is part of the blood is removed from the patient (Cao-Lormeau et al.,
2016). Healthcare professional thereafter have to place back the cells into the body. Plasma
exchange is a very effective treatment method because it is capable of shortening the length and
effects of GBs symptoms. The second treatment method which is recommended by healthcare
professionals is immunoglobulin therapy in which the infected blood of the patient which is
weak and not able to fight back infections is removed and healthy blood which has the capability
of fighting infections is put in the body of the patient (Nomura, 2015).
occurs if the person is suffering from GBS. Healthcare professionals can also use
electromyography in which they insert thin needles electrodes in the muscles of the patient.
Electrodes plays are very major role of measuring if nerve activities in the muscles are working
properly. Nerve condition studies is the third test which healthcare professionals carry out to
examine if a patient is affected by GBS (Nyati & Nyati, 2013). This test includes sticking small
discs of electrodes to the body of the patients. Healthcare professionals use minor electric shocks
to activate the nerve and measure how faster the signals have traveled along them. Lumber
puncture is the last pathophysiology of GBS used to remove some fluids around the spinal cord
through a needle which is inserted in the lower part of the spine.
Management and treatment of Guillain Barre Syndrome
In most cases patients with vital signs and symptoms of GBS are hospitalized so that
healthcare professionals can carefully monitor their progress and respond to medication and
treatments they are administering to them. The duration in which the patient spend in the hospital
vary from days to weeks depending on how critical their health status is in. the first type of
treatment which healthcare professionals can give to patients is plasma exchange in which blood
is drawn and plasma which is part of the blood is removed from the patient (Cao-Lormeau et al.,
2016). Healthcare professional thereafter have to place back the cells into the body. Plasma
exchange is a very effective treatment method because it is capable of shortening the length and
effects of GBs symptoms. The second treatment method which is recommended by healthcare
professionals is immunoglobulin therapy in which the infected blood of the patient which is
weak and not able to fight back infections is removed and healthy blood which has the capability
of fighting infections is put in the body of the patient (Nomura, 2015).
GUILLAIN BARRE SYNDROME 9
Patients with severe GBS especially the ones experiencing respiratory problems are put
on ventilators which helps them to breath. With this treatment methods most people are able to
recover completely even the ones with severe GBs symptoms. However, in most cases fatigue
which is a major symptom of GBS persist even after the patient has recovered. The recovery
process of GBS sometimes tend to be very slow, and in severe cases this infection can leave a
patient almost completely paralyzed (McNair, 2013). GBS is considered a life threatening
infection because it is associated with respiratory problems which can interfere with breathing of
a patient. Management of GBS involves preventing and dealing with complications such as
breathing problems by providing supportive care until the symptoms of the patients begins to
improve (Salmon et al., 2013).
Conclusion
Guillain Barre Syndrome is a life threatening infection across the globe. The infection
affect people of all races and age. GBS is accompanied by a number of life threatening signs and
symptoms which if not taken good care of can lead to death. Therefore, it is the role of healthcare
professionals to ensure that they carefully monitor the progress of a patient with this infection
before it results in permanent conditions like paralysis. Healthcare institutions should ensure that
they have the best treatment methods in place which can be used to treat and prevent this
infection. GBS can be conducted from bacterial infection called Campylobacter jejuni infection
which is commonly found in undercooked food, therefore people are advised to make sure that
they take food which is properly cooked to reduce chances of them been infected by this
infection.
Patients with severe GBS especially the ones experiencing respiratory problems are put
on ventilators which helps them to breath. With this treatment methods most people are able to
recover completely even the ones with severe GBs symptoms. However, in most cases fatigue
which is a major symptom of GBS persist even after the patient has recovered. The recovery
process of GBS sometimes tend to be very slow, and in severe cases this infection can leave a
patient almost completely paralyzed (McNair, 2013). GBS is considered a life threatening
infection because it is associated with respiratory problems which can interfere with breathing of
a patient. Management of GBS involves preventing and dealing with complications such as
breathing problems by providing supportive care until the symptoms of the patients begins to
improve (Salmon et al., 2013).
Conclusion
Guillain Barre Syndrome is a life threatening infection across the globe. The infection
affect people of all races and age. GBS is accompanied by a number of life threatening signs and
symptoms which if not taken good care of can lead to death. Therefore, it is the role of healthcare
professionals to ensure that they carefully monitor the progress of a patient with this infection
before it results in permanent conditions like paralysis. Healthcare institutions should ensure that
they have the best treatment methods in place which can be used to treat and prevent this
infection. GBS can be conducted from bacterial infection called Campylobacter jejuni infection
which is commonly found in undercooked food, therefore people are advised to make sure that
they take food which is properly cooked to reduce chances of them been infected by this
infection.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
GUILLAIN BARRE SYNDROME 10
References
Ansar, V., & Valadi, N. (2015). Guillain-Barré syndrome. Primary Care: Clinics in Office
Practice, 42(2), 189-193.
Cao-Lormeau, V. M., Blake, A., Mons, S., Lastère, S., Roche, C., Vanhomwegen, J., ... & Vial,
A. L. (2016). Guillain-Barré Syndrome outbreak associated with Zika virus infection in
French Polynesia: a case-control study. The Lancet, 387(10027), 1531-1539.
McNair, N. D. (2013). Treatment of Guillain-Barre Syndrome. Journal of Infusion
Nursing, 36(6), 397-400.
Musso, D., Nilles, E. J., & Cao‐Lormeau, V. M. (2014). Rapid spread of emerging Z ika virus in
the P acific area. Clinical Microbiology and Infection, 20(10), O595-O596.
Nomura, K. (2015). Treatment of Guillain-Barré syndrome. Brain and nerve= Shinkei kenkyu no
shinpo, 67(11), 1397-1410.
Nyati, K. K., & Nyati, R. (2013). Role of Campylobacter jejuni infection in the pathogenesis of
Guillain-Barré syndrome: an update. BioMed research international, 2013.
Oehler, E., Watrin, L., Larre, P., Leparc-Goffart, I., Lastere, S., Valour, F., ... & Ghawche, F.
(2014). Zika virus infection complicated by Guillain-Barre syndrome–case report, French
Polynesia, December 2013. Eurosurveillance, 19(9), 20720.
Salmon, D. A., Proschan, M., Forshee, R., Gargiullo, P., Bleser, W., Burwen, D. R., ... &
Vellozzi, C. (2013). Association between Guillain-Barré syndrome and influenza A
(H1N1) 2009 monovalent inactivated vaccines in the USA: a meta-analysis. The
Lancet, 381(9876), 1461-1468.
References
Ansar, V., & Valadi, N. (2015). Guillain-Barré syndrome. Primary Care: Clinics in Office
Practice, 42(2), 189-193.
Cao-Lormeau, V. M., Blake, A., Mons, S., Lastère, S., Roche, C., Vanhomwegen, J., ... & Vial,
A. L. (2016). Guillain-Barré Syndrome outbreak associated with Zika virus infection in
French Polynesia: a case-control study. The Lancet, 387(10027), 1531-1539.
McNair, N. D. (2013). Treatment of Guillain-Barre Syndrome. Journal of Infusion
Nursing, 36(6), 397-400.
Musso, D., Nilles, E. J., & Cao‐Lormeau, V. M. (2014). Rapid spread of emerging Z ika virus in
the P acific area. Clinical Microbiology and Infection, 20(10), O595-O596.
Nomura, K. (2015). Treatment of Guillain-Barré syndrome. Brain and nerve= Shinkei kenkyu no
shinpo, 67(11), 1397-1410.
Nyati, K. K., & Nyati, R. (2013). Role of Campylobacter jejuni infection in the pathogenesis of
Guillain-Barré syndrome: an update. BioMed research international, 2013.
Oehler, E., Watrin, L., Larre, P., Leparc-Goffart, I., Lastere, S., Valour, F., ... & Ghawche, F.
(2014). Zika virus infection complicated by Guillain-Barre syndrome–case report, French
Polynesia, December 2013. Eurosurveillance, 19(9), 20720.
Salmon, D. A., Proschan, M., Forshee, R., Gargiullo, P., Bleser, W., Burwen, D. R., ... &
Vellozzi, C. (2013). Association between Guillain-Barré syndrome and influenza A
(H1N1) 2009 monovalent inactivated vaccines in the USA: a meta-analysis. The
Lancet, 381(9876), 1461-1468.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
GUILLAIN BARRE SYNDROME 11
van den Berg, B., Bunschoten, C., van Doorn, P. A., & Jacobs, B. C. (2013). Mortality in
guillain-barre syndrome. Neurology, 80(18), 1650-1654.
Van den Berg, B., Walgaard, C., Drenthen, J., Fokke, C., Jacobs, B. C., & Van Doorn, P. A.
(2014). Guillain–Barré syndrome: pathogenesis, diagnosis, treatment and
prognosis. Nature Reviews Neurology, 10(8), 469.
van Doorn, P. A. (2013). Diagnosis, treatment and prognosis of Guillain-Barré syndrome
(GBS). La Presse Médicale, 42(6), e193-e201.
Wijdicks, E. F., & Klein, C. J. (2017, March). Guillain-barre syndrome. In Mayo Clinic
Proceedings (Vol. 92, No. 3, pp. 467-479). Elsevier.
Willison, H. J., Jacobs, B. C., & Van Doorn, P. A. (2016). Guillain-barre syndrome. The
Lancet, 388(10045), 717-727.
World Health Organization. (2016). Zika virus, microcephaly and Guillain-Barré syndrome
situation report.
van den Berg, B., Bunschoten, C., van Doorn, P. A., & Jacobs, B. C. (2013). Mortality in
guillain-barre syndrome. Neurology, 80(18), 1650-1654.
Van den Berg, B., Walgaard, C., Drenthen, J., Fokke, C., Jacobs, B. C., & Van Doorn, P. A.
(2014). Guillain–Barré syndrome: pathogenesis, diagnosis, treatment and
prognosis. Nature Reviews Neurology, 10(8), 469.
van Doorn, P. A. (2013). Diagnosis, treatment and prognosis of Guillain-Barré syndrome
(GBS). La Presse Médicale, 42(6), e193-e201.
Wijdicks, E. F., & Klein, C. J. (2017, March). Guillain-barre syndrome. In Mayo Clinic
Proceedings (Vol. 92, No. 3, pp. 467-479). Elsevier.
Willison, H. J., Jacobs, B. C., & Van Doorn, P. A. (2016). Guillain-barre syndrome. The
Lancet, 388(10045), 717-727.
World Health Organization. (2016). Zika virus, microcephaly and Guillain-Barré syndrome
situation report.
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.