Master of Hospital Management Hand Hygiene Audit Project
VerifiedAdded on 2022/10/14
|22
|7086
|339
Project
AI Summary
This project, conducted as part of a Master of Hospital Management field practicum, investigates hand hygiene practices, attitudes, and barriers among healthcare providers at Zayed Military Hospital in Al Batayeh, Sharjah. The study, which included a cross-sectional observational survey of 100 healthcare professionals, aimed to determine compliance with hand hygiene protocols, identify factors influencing adherence, and assess the knowledge of healthcare staff regarding optimal hand hygiene. The findings revealed poor hand hygiene compliance, with partial adherence being surprisingly high. Significant differences were observed in attitudes towards hand hygiene between medical and nursing professionals. Key barriers to adherence included inconvenient placement of hand hygiene facilities, heavy patient workloads, understaffing, and the perception that hand hygiene is time-consuming. The project recommends improvements in hand hygiene facilities to enhance accessibility and encourage better practices, ultimately benefiting both healthcare workers and patients. The study also reviews the literature on hand hygiene, highlighting its importance in preventing healthcare-associated infections (HCAIs) and discussing the factors that contribute to poor compliance, as well as the guidelines and recommendations for hand hygiene practices.

0
Master of Hospital Management
Field Practicum Course (Summer 2019)
AUDIT PROJECT:
ATTITUDES AND BARRIERS FOR OPTIMAL HAND HYGIENE AMONG HEALTH CARE
PROVIDERS IN ZAYED MILITARY HOSPITAL AL BATAYEH, SHARJAH
Submitted By: Amna Aladwani 200104787
Submitted to: Prof. Awoniyi Awofeso
Date: 28/July/2019
Word Count: 2705 words
Abstract
Master of Hospital Management
Field Practicum Course (Summer 2019)
AUDIT PROJECT:
ATTITUDES AND BARRIERS FOR OPTIMAL HAND HYGIENE AMONG HEALTH CARE
PROVIDERS IN ZAYED MILITARY HOSPITAL AL BATAYEH, SHARJAH
Submitted By: Amna Aladwani 200104787
Submitted to: Prof. Awoniyi Awofeso
Date: 28/July/2019
Word Count: 2705 words
Abstract
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
Introduction: “Prevention is better than cure”. Therefore, proper hands hygiene practice stands
out to be one of the measures of reducing transmission of disease to patients and to health care
providers. The practice is considered to be in the front line in prevention of health care
associated infections (HCAI) and Nosocomial Infections/Hospital Acquired Infections (Kumar,
Gupta, Kapil, Vij & Singh, 2014). Washing hands is taking a second position from hand rub to
meet the recommended standards with optimum time considered to be between 30 seconds and
one minute. The alcohol antiseptics are recommended worldwide due to their broad-spectrum
antimicrobial effects, the application process is easy and they are tolerable to many people skins
(Zayed Military Hospital - Al Batayeh, 2016). The scope of hand hygiene includes hand
washing, use of antiseptics to wash hands or rub and surgical hand antisepsis. Health care
associated infection (HCAI) is one of the most significant, and current phenomena for
discussions in health care industry. Hand hygiene was thought to be a key factor in reducing
hospital acquired infection during the initial development of healthcare system (Ducell, Fabry &
Nicoll, 2002). The present study aimed to determine hand hygiene compliance, attitude and
barriers among health care workers (HCWs).
Material & Methods: A cross sectional observational survey was conducted in 100 health care
providers from different out-patient departments at Zayed Military Hospital Al Batayeh,
Sharjah Convenience consecutive sampling technique was used to enroll HCPs. Modified hand
hygiene checklist, interview for identification of barriers was used to ascertain compliance,
attitude and barriers. Appropriate descriptive statistics was applied to compute the results.
Results: Results shows higher adherence (10%) to hand hygiene practices among faculty
followed by consultants (7.14%) and specialists (6.71%). However, the partial adherence to
hand hygiene practices was surprisingly high (63.04%) among HCWs. There was significant
difference in attitude towards hand hygiene practices among medical and nursing professionals.
Further, findings revealed that inconvenient placement of hand hygiene facility was prime
reported (85.21%) barrier for poor adherence to hand hygiene practices followed by over
burden of patient (80.87%), understaffing/overcrowding (81.73%) and hand hygiene is time
consuming activity (80.86%) HCWs.
Introduction: “Prevention is better than cure”. Therefore, proper hands hygiene practice stands
out to be one of the measures of reducing transmission of disease to patients and to health care
providers. The practice is considered to be in the front line in prevention of health care
associated infections (HCAI) and Nosocomial Infections/Hospital Acquired Infections (Kumar,
Gupta, Kapil, Vij & Singh, 2014). Washing hands is taking a second position from hand rub to
meet the recommended standards with optimum time considered to be between 30 seconds and
one minute. The alcohol antiseptics are recommended worldwide due to their broad-spectrum
antimicrobial effects, the application process is easy and they are tolerable to many people skins
(Zayed Military Hospital - Al Batayeh, 2016). The scope of hand hygiene includes hand
washing, use of antiseptics to wash hands or rub and surgical hand antisepsis. Health care
associated infection (HCAI) is one of the most significant, and current phenomena for
discussions in health care industry. Hand hygiene was thought to be a key factor in reducing
hospital acquired infection during the initial development of healthcare system (Ducell, Fabry &
Nicoll, 2002). The present study aimed to determine hand hygiene compliance, attitude and
barriers among health care workers (HCWs).
Material & Methods: A cross sectional observational survey was conducted in 100 health care
providers from different out-patient departments at Zayed Military Hospital Al Batayeh,
Sharjah Convenience consecutive sampling technique was used to enroll HCPs. Modified hand
hygiene checklist, interview for identification of barriers was used to ascertain compliance,
attitude and barriers. Appropriate descriptive statistics was applied to compute the results.
Results: Results shows higher adherence (10%) to hand hygiene practices among faculty
followed by consultants (7.14%) and specialists (6.71%). However, the partial adherence to
hand hygiene practices was surprisingly high (63.04%) among HCWs. There was significant
difference in attitude towards hand hygiene practices among medical and nursing professionals.
Further, findings revealed that inconvenient placement of hand hygiene facility was prime
reported (85.21%) barrier for poor adherence to hand hygiene practices followed by over
burden of patient (80.87%), understaffing/overcrowding (81.73%) and hand hygiene is time
consuming activity (80.86%) HCWs.
2
Conclusion & recommendation: The study concluded poor hand hygiene compliance among
HCWs. Study findings recommend improvement in existing facilities for hand hygiene and
make them readily accessible for HCWs at their respective departments to enable them to
engage in good practices which will be beneficial for them and patients.
Introduction
The Health Care Associated Infections (HCAI) trigger the main challenges to the health care
provision. This is because of the burden put on the people, families as well as health services.
HCAI is described as the infection acquired by both patients and healthcare providers while
seeking and providing treatment in the healthcare facilities respectively. HCAIs are caused by a
range of microbes like parasites, fungi, viruses and remains readily associated with bacteria. The
routes for transmission include via endogenous or exogenous infection agents. The former agents
are the infections triggered by microorganisms present in the body of patients that spread from
one to another area often via the hands of the HCWs by touching the area infected. The latter
agents sources further act as the reservoir of infections and encompass nose, skin, mouth, vagina
and gastrointestinal tract (Kurtz, 2017).
HCWs with poor HH adherence who never wash their hands in between indirect or direct with
patients might rapidly transmit potential antimicrobial resistant bacteria to the rest of the patients.
HCWs hands slowly get exposed as well as colonized by the germs and feasibly microbes as they
tend to patients. Thus, there is a surged risk of HCAI acquisition from the HCW with augmented
amount of hand contamination specifically in the Hospital lacking HH (Schwartz, Schmitz,
Safdar & Pop-Vicas, 2018).
Exogenous infections get spread because of external sources often through direct contact with
infected patients or via the surrounding. Exogenous infections sources include HCWs, patient
care equipment, visitors, as well as medical devices. Thus, HCWs hands alongside patients
remain the major trigger for HCAI spread both exogenously and endogenously to fellow patients
and HCW and visitors. It is, thus, imperative to examine the HH behavior of health care workers
in the Hospital faced with the provision of quality health care as well as patient safety
irrespective of scarce health system facilities or systems.
Conclusion & recommendation: The study concluded poor hand hygiene compliance among
HCWs. Study findings recommend improvement in existing facilities for hand hygiene and
make them readily accessible for HCWs at their respective departments to enable them to
engage in good practices which will be beneficial for them and patients.
Introduction
The Health Care Associated Infections (HCAI) trigger the main challenges to the health care
provision. This is because of the burden put on the people, families as well as health services.
HCAI is described as the infection acquired by both patients and healthcare providers while
seeking and providing treatment in the healthcare facilities respectively. HCAIs are caused by a
range of microbes like parasites, fungi, viruses and remains readily associated with bacteria. The
routes for transmission include via endogenous or exogenous infection agents. The former agents
are the infections triggered by microorganisms present in the body of patients that spread from
one to another area often via the hands of the HCWs by touching the area infected. The latter
agents sources further act as the reservoir of infections and encompass nose, skin, mouth, vagina
and gastrointestinal tract (Kurtz, 2017).
HCWs with poor HH adherence who never wash their hands in between indirect or direct with
patients might rapidly transmit potential antimicrobial resistant bacteria to the rest of the patients.
HCWs hands slowly get exposed as well as colonized by the germs and feasibly microbes as they
tend to patients. Thus, there is a surged risk of HCAI acquisition from the HCW with augmented
amount of hand contamination specifically in the Hospital lacking HH (Schwartz, Schmitz,
Safdar & Pop-Vicas, 2018).
Exogenous infections get spread because of external sources often through direct contact with
infected patients or via the surrounding. Exogenous infections sources include HCWs, patient
care equipment, visitors, as well as medical devices. Thus, HCWs hands alongside patients
remain the major trigger for HCAI spread both exogenously and endogenously to fellow patients
and HCW and visitors. It is, thus, imperative to examine the HH behavior of health care workers
in the Hospital faced with the provision of quality health care as well as patient safety
irrespective of scarce health system facilities or systems.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
Hand Hygiene (HH) actions or practices remain cost-effective mechanisms towards the reduction
of the spread of HCAIs and have since proven extremely effective in the prevention of
transmission of microbes during the care for patients. It has since been verified that HCAIs hands
remain the major routes of HCAIs transmission. Despite this knowledge, HH remains overlooked
frequently among the HCWs specifically in the Hospitals with restricted resources. This current
study, hence, explores the HH knowledge and behaviors of private and public HCWs with focus
on the health belief model to understand the barriers and attitudes of the HCWs for optimal hand
hygiene in the Zayed Military Hospital.
The needed information or data was collected from the HCWs form the health care facility using
the structured questionnaires based on the WHO evaluation tool kit and the literature review on
the previous articles on the topic. HH knowledge of HCWs corresponded with their respective
HH behaviors and practices. Insufficient HH performance was observed in various HCWs
alongside limited HH resources availabilities from the Hospital. Private healthcare facilities
availed better HH opportunities for their HCWs, however, neither public nor private facilities
provided sufficient HH training alongside feedback on HH performance to their HCWs.
Problem Statement: HCAI remains a severe challenge which is presently faced by all Hospitals
globally irrespective of the economic state. Not solely does HCAI encompasses patient safety,
but also that of the health care workers. It remains in all HCWs interest to tackle this problem
and guarantee improved safety of patients alongside establishing suitable work surrounding for
all workers. Most specifically, since the adverse effects of HCAIs encompasses extra costs for
patients, surged resistance to the antimicrobials alongside a higher burden (financial) for the
society at large. Many HCWs in this Zayed Military Hospital are faced by the combination of
various determinants triggering a higher risk of HCAIs transmission. As noted above, such might
encompass understaffing, ineffective infrastructure with missing hygiene besides sanitation
conditions, shortage or lack of basic equipment, overcrowding of patients; all of which might be
connected to scarce financial resources.
Surveillance on health care workers HH actions and practices plays a key role towards
accomplishing safer alongside higher quality care for patients. Globally, campaigns have been
created to support prevention and control programs for infections including initiatives for HH.
Hand Hygiene (HH) actions or practices remain cost-effective mechanisms towards the reduction
of the spread of HCAIs and have since proven extremely effective in the prevention of
transmission of microbes during the care for patients. It has since been verified that HCAIs hands
remain the major routes of HCAIs transmission. Despite this knowledge, HH remains overlooked
frequently among the HCWs specifically in the Hospitals with restricted resources. This current
study, hence, explores the HH knowledge and behaviors of private and public HCWs with focus
on the health belief model to understand the barriers and attitudes of the HCWs for optimal hand
hygiene in the Zayed Military Hospital.
The needed information or data was collected from the HCWs form the health care facility using
the structured questionnaires based on the WHO evaluation tool kit and the literature review on
the previous articles on the topic. HH knowledge of HCWs corresponded with their respective
HH behaviors and practices. Insufficient HH performance was observed in various HCWs
alongside limited HH resources availabilities from the Hospital. Private healthcare facilities
availed better HH opportunities for their HCWs, however, neither public nor private facilities
provided sufficient HH training alongside feedback on HH performance to their HCWs.
Problem Statement: HCAI remains a severe challenge which is presently faced by all Hospitals
globally irrespective of the economic state. Not solely does HCAI encompasses patient safety,
but also that of the health care workers. It remains in all HCWs interest to tackle this problem
and guarantee improved safety of patients alongside establishing suitable work surrounding for
all workers. Most specifically, since the adverse effects of HCAIs encompasses extra costs for
patients, surged resistance to the antimicrobials alongside a higher burden (financial) for the
society at large. Many HCWs in this Zayed Military Hospital are faced by the combination of
various determinants triggering a higher risk of HCAIs transmission. As noted above, such might
encompass understaffing, ineffective infrastructure with missing hygiene besides sanitation
conditions, shortage or lack of basic equipment, overcrowding of patients; all of which might be
connected to scarce financial resources.
Surveillance on health care workers HH actions and practices plays a key role towards
accomplishing safer alongside higher quality care for patients. Globally, campaigns have been
created to support prevention and control programs for infections including initiatives for HH.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
Nonetheless, solely a few hospitals manage to offer functional evaluation alongside monitoring
systems. Likely rationale for this remain the demanding alongside intensive requirements of the
national surveillance system associated with scarce resource allocation towards HCAI in these
hospitals where additional emerging health concerns and illness are accorded preference
(Kingston, Slevin, O'Connell & Dunne, 2017).
This study will emphasize on HH adherence for HCWs in Zayed Military Hospital where the
lack of enough HH resources is dominant and also marred with various HH barriers and negative
attitude of HCWs to proper HH practices.
Literature review
The provision of healthcare worldwide is always associated with a potential range of safety
problems. Yet, despite advances in healthcare systems, patients remain vulnerable to
unintentional harm in hospitals. Health care associated infection (HCAI) is the most frequent
adverse event in health care delivery system worldwide. The overall prevalence of HCAI in
developed countries varies from 5.1% to 11.6% and in developing countries it is around 15.6%
(World Health Organization, 2001). Hand hygiene is an important healthcare issue globally and
is a single most cost-effective and practical measure to reduce the incidence of HCAI and the
spread of antimicrobial resistance across all settings-from advanced health care systems to
primary healthcare centers.
Adequate hand hygiene among hospital personal could prevent an estimated 15 to 30% of the
HCAI despite the relative simplicity of this procedure, compliance to hand hygiene practices
among health care providers is as low as 40% (Kumar, Gupta, Kapil, Vij & Singh, 2014).
However, there are certain factors which predispose poor compliance to hand hygiene among
health care providers. Some of these factors are present regardless of the resources available like
prolonged and inappropriate use of invasive devices and antibiotics, high risk and sophisticated
procedures, insufficient application of standard and isolation precautions, immuno-suppression
and other severe underlying patient conditions (Ducell, Fabry & Nicoll, 2002).
Nonetheless, solely a few hospitals manage to offer functional evaluation alongside monitoring
systems. Likely rationale for this remain the demanding alongside intensive requirements of the
national surveillance system associated with scarce resource allocation towards HCAI in these
hospitals where additional emerging health concerns and illness are accorded preference
(Kingston, Slevin, O'Connell & Dunne, 2017).
This study will emphasize on HH adherence for HCWs in Zayed Military Hospital where the
lack of enough HH resources is dominant and also marred with various HH barriers and negative
attitude of HCWs to proper HH practices.
Literature review
The provision of healthcare worldwide is always associated with a potential range of safety
problems. Yet, despite advances in healthcare systems, patients remain vulnerable to
unintentional harm in hospitals. Health care associated infection (HCAI) is the most frequent
adverse event in health care delivery system worldwide. The overall prevalence of HCAI in
developed countries varies from 5.1% to 11.6% and in developing countries it is around 15.6%
(World Health Organization, 2001). Hand hygiene is an important healthcare issue globally and
is a single most cost-effective and practical measure to reduce the incidence of HCAI and the
spread of antimicrobial resistance across all settings-from advanced health care systems to
primary healthcare centers.
Adequate hand hygiene among hospital personal could prevent an estimated 15 to 30% of the
HCAI despite the relative simplicity of this procedure, compliance to hand hygiene practices
among health care providers is as low as 40% (Kumar, Gupta, Kapil, Vij & Singh, 2014).
However, there are certain factors which predispose poor compliance to hand hygiene among
health care providers. Some of these factors are present regardless of the resources available like
prolonged and inappropriate use of invasive devices and antibiotics, high risk and sophisticated
procedures, insufficient application of standard and isolation precautions, immuno-suppression
and other severe underlying patient conditions (Ducell, Fabry & Nicoll, 2002).
5
Some of the guidelines provided by CDC in 2000 are in line with those released by WHO in
2009 and recommends that visible dirt is supposed to be washed with soap or antiseptic and
water since hand rubs do not clean soiled hands and rinsing is important in this case, routine
hand washing require a minimum of 60 seconds with antiseptics and water, those working in
health sectors are supposed to use hand cream to reduce skin damages since skin that is
destroyed inhabit many pathogens and microorganisms, health care workers should use cold
water to clean their hands since hot water leads to a drying effect that spoil the skin, after
alcohol- based hand rubs are applied, the hands should be rubbed together for complete drying,
paper towel should be used for drying of hands or single use towel, multiple use or hang roll
towel should not be used and Alcohol –based hand rubs should be applied in five moments of
hand wash and not on contaminated hands that have dirt that is visible. Also, before wearing
and after removing of sterile and non-sterile gloves (Zayed Military Hospital - Al Batayeh,
2019).
Several studies have shown there is reduction of healthcare acquired infections with hand
hygiene compliance. In 1847, Semmelwels demonstrated that decontaminating hands with
chlorine prior to delivering a baby would reduce child death from 11.4% to 3.05%. Backman,
Zoutman, and Marck reviewed 31 studies 18 of all the reviewed studies showed that intervention
on hand hygiene compliance lead to reduction of hospital acquired infections. Other studies that
showed reduction had a range between 0.37% in rotavirus to 57% in MRSA bacteria (Allegranzi
& Pittet, 2009).
Despite the evidence that complying with hand hygiene reduces hospital acquired infections,
CDC report shows that health care workers have only showed 40% compliance. Recent studies
in USA have shown even more dismal performance with a record of 26% in intensive care unit
and 36% in non–intensive care unit ("Hand Hygiene in Healthcare Settings | CDC", 2019).
Despite the much effort that has been put on finding out the factors that leads to poor hand
hygiene practice and the interventions put forward little seems to be happening. This study
sought to assess if the undergraduate medical student had knowledge on hand hygiene and what
were their attitude and barriers on the practice which has received minimal attention yet could be
Some of the guidelines provided by CDC in 2000 are in line with those released by WHO in
2009 and recommends that visible dirt is supposed to be washed with soap or antiseptic and
water since hand rubs do not clean soiled hands and rinsing is important in this case, routine
hand washing require a minimum of 60 seconds with antiseptics and water, those working in
health sectors are supposed to use hand cream to reduce skin damages since skin that is
destroyed inhabit many pathogens and microorganisms, health care workers should use cold
water to clean their hands since hot water leads to a drying effect that spoil the skin, after
alcohol- based hand rubs are applied, the hands should be rubbed together for complete drying,
paper towel should be used for drying of hands or single use towel, multiple use or hang roll
towel should not be used and Alcohol –based hand rubs should be applied in five moments of
hand wash and not on contaminated hands that have dirt that is visible. Also, before wearing
and after removing of sterile and non-sterile gloves (Zayed Military Hospital - Al Batayeh,
2019).
Several studies have shown there is reduction of healthcare acquired infections with hand
hygiene compliance. In 1847, Semmelwels demonstrated that decontaminating hands with
chlorine prior to delivering a baby would reduce child death from 11.4% to 3.05%. Backman,
Zoutman, and Marck reviewed 31 studies 18 of all the reviewed studies showed that intervention
on hand hygiene compliance lead to reduction of hospital acquired infections. Other studies that
showed reduction had a range between 0.37% in rotavirus to 57% in MRSA bacteria (Allegranzi
& Pittet, 2009).
Despite the evidence that complying with hand hygiene reduces hospital acquired infections,
CDC report shows that health care workers have only showed 40% compliance. Recent studies
in USA have shown even more dismal performance with a record of 26% in intensive care unit
and 36% in non–intensive care unit ("Hand Hygiene in Healthcare Settings | CDC", 2019).
Despite the much effort that has been put on finding out the factors that leads to poor hand
hygiene practice and the interventions put forward little seems to be happening. This study
sought to assess if the undergraduate medical student had knowledge on hand hygiene and what
were their attitude and barriers on the practice which has received minimal attention yet could be
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

6
a root cause of poor hand hygiene compliance in the healthcare settings (Basurrah & Madani,
2006).
Objectives
The aims and objectives of this project were to determine:
The prevalence of healthcare staff compliance in hand hygiene.
The attitude, factors and barriers affecting hand hygiene.
The knowledge of healthcare staff regarding optimal hand hygiene.
The suggested recommendations to improve the healthcare staff compliance. Excellent
outline and approach.
Methodology
A cross sectional observation was conducted among different kind of 100 HWPs working and
undergoing training at Zayed Military Hospital Al Batayeh, Sharjah. Convenience consecutive
sampling technique was adopted to enroll subjects over a period of 15 days. Data was collected
through a socio- demographic data sheet, Modified Hand hygiene performance from Zayed
Military Hospital, structured questionnaire and interview which is prepared with help of HICC
and approved by ethical committee. A group of trained nursing staffs observed hand hygiene
practices in respective area and questioned information on attitude and barriers. The detail of
instruments are given below:
Part A: Socio-demographic Profile Sheet:
This encompasses gender, age, level of education, religion, working experience year, kind
of educational institute finished, in-service training/education on hand-hygiene practices
exposure, and intern students’’ course. The tool’s validity was sought from the experts in
the general surgery, nursing, medicine and microbiology fields.
Part B: Hand Hygiene Observation Proforma in Zayed Military Hospital:
This is comprehensive proforma based on World Health Organization’s checklist for
hand hygiene from hospital and modified with the aid of professionals in infection control
and prevention department of Zayed Military Hospital Al Batayeh, Sharjah. It
a root cause of poor hand hygiene compliance in the healthcare settings (Basurrah & Madani,
2006).
Objectives
The aims and objectives of this project were to determine:
The prevalence of healthcare staff compliance in hand hygiene.
The attitude, factors and barriers affecting hand hygiene.
The knowledge of healthcare staff regarding optimal hand hygiene.
The suggested recommendations to improve the healthcare staff compliance. Excellent
outline and approach.
Methodology
A cross sectional observation was conducted among different kind of 100 HWPs working and
undergoing training at Zayed Military Hospital Al Batayeh, Sharjah. Convenience consecutive
sampling technique was adopted to enroll subjects over a period of 15 days. Data was collected
through a socio- demographic data sheet, Modified Hand hygiene performance from Zayed
Military Hospital, structured questionnaire and interview which is prepared with help of HICC
and approved by ethical committee. A group of trained nursing staffs observed hand hygiene
practices in respective area and questioned information on attitude and barriers. The detail of
instruments are given below:
Part A: Socio-demographic Profile Sheet:
This encompasses gender, age, level of education, religion, working experience year, kind
of educational institute finished, in-service training/education on hand-hygiene practices
exposure, and intern students’’ course. The tool’s validity was sought from the experts in
the general surgery, nursing, medicine and microbiology fields.
Part B: Hand Hygiene Observation Proforma in Zayed Military Hospital:
This is comprehensive proforma based on World Health Organization’s checklist for
hand hygiene from hospital and modified with the aid of professionals in infection control
and prevention department of Zayed Military Hospital Al Batayeh, Sharjah. It
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
encompasses information regarding the type of health care providers, number of
opportunities for hand hygiene faced in defined time, and hand hygiene practices (hand
wash and hand rub) etc. The tool validity was verified after submitting the tools to experts
in the field of nursing, surgery, medicine & Hospital Infection Control Committee
(HICC).
Part C: Attitude Scale: It is a self-develop five-point Likert Scale comprising eleven items
linked to the attitude towards the practices of hand-hygiene. Every item got measured on
five-point rating scale with Strongly Agree given 5; to Strong disagree given 1. The tool’s
reliability got conformed using the Cronbach‘s alpha and it stood at 0.830 for this present
study. The scale for attitude was discovered valid as well as reliable for this current study.
Part D- Structured Questionnaire:
It comprised of the factors hindering hand hygiene compliance among health care providers i.e.
availability of time, sink, soap and water which is prepared by the help of supervision from
HICC, on-site Supervisor and lack of knowledge of guidelines/ protocols etc. Validity of tool
was confirmed after submitting the tools to experts in the field of nursing, surgery, medicine &
HICC.
In addition, interview method also used like 10 selected open-ended questions approved by
hospital administration, ethical committee and HICC (appendix 2) to assess the staff knowledge,
factors, barriers and attitude in hand hygiene.
Ethical Consideration: The current study got the approval by the Institutional Ethical
Committee and information confidentiality as well as subjects’ anonymity stood
guaranteed both after and during the collection of data period. Such an ethical approval
wave-off requirement for consent for observation to eliminate bias and ensure best
outcomes regarding the compliance with hand-hygiene guidelines. Analysis of data was
through SPSS version twenty and both inferential and descriptive statistics were utilized.
encompasses information regarding the type of health care providers, number of
opportunities for hand hygiene faced in defined time, and hand hygiene practices (hand
wash and hand rub) etc. The tool validity was verified after submitting the tools to experts
in the field of nursing, surgery, medicine & Hospital Infection Control Committee
(HICC).
Part C: Attitude Scale: It is a self-develop five-point Likert Scale comprising eleven items
linked to the attitude towards the practices of hand-hygiene. Every item got measured on
five-point rating scale with Strongly Agree given 5; to Strong disagree given 1. The tool’s
reliability got conformed using the Cronbach‘s alpha and it stood at 0.830 for this present
study. The scale for attitude was discovered valid as well as reliable for this current study.
Part D- Structured Questionnaire:
It comprised of the factors hindering hand hygiene compliance among health care providers i.e.
availability of time, sink, soap and water which is prepared by the help of supervision from
HICC, on-site Supervisor and lack of knowledge of guidelines/ protocols etc. Validity of tool
was confirmed after submitting the tools to experts in the field of nursing, surgery, medicine &
HICC.
In addition, interview method also used like 10 selected open-ended questions approved by
hospital administration, ethical committee and HICC (appendix 2) to assess the staff knowledge,
factors, barriers and attitude in hand hygiene.
Ethical Consideration: The current study got the approval by the Institutional Ethical
Committee and information confidentiality as well as subjects’ anonymity stood
guaranteed both after and during the collection of data period. Such an ethical approval
wave-off requirement for consent for observation to eliminate bias and ensure best
outcomes regarding the compliance with hand-hygiene guidelines. Analysis of data was
through SPSS version twenty and both inferential and descriptive statistics were utilized.
8
Results and Recommended Improvements
Hand Hygiene Compliance
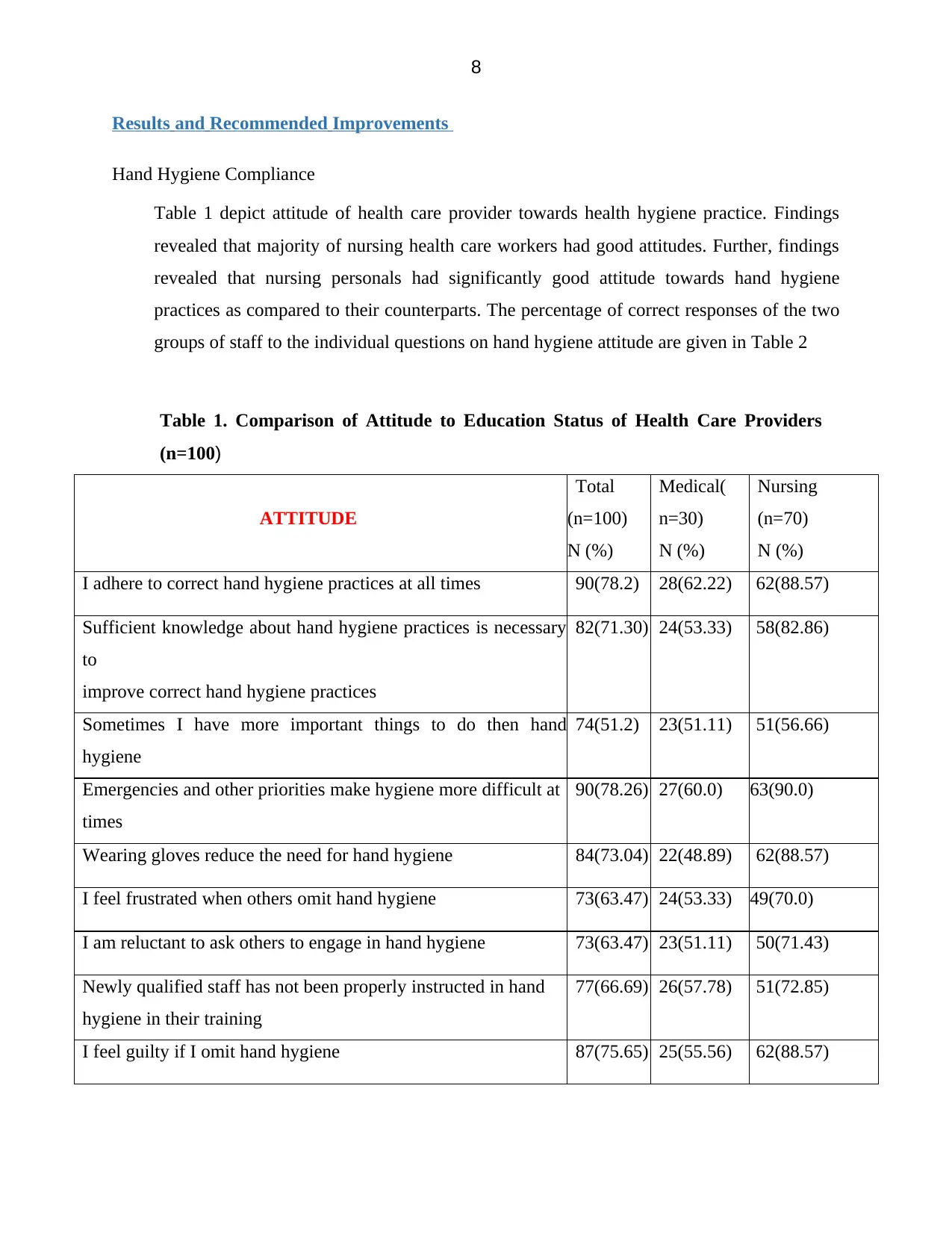
Table 1 depict attitude of health care provider towards health hygiene practice. Findings
revealed that majority of nursing health care workers had good attitudes. Further, findings
revealed that nursing personals had significantly good attitude towards hand hygiene
practices as compared to their counterparts. The percentage of correct responses of the two
groups of staff to the individual questions on hand hygiene attitude are given in Table 2
Table 1. Comparison of Attitude to Education Status of Health Care Providers
(n=100)
ATTITUDE
Total
(n=100)
N (%)
Medical(
n=30)
N (%)
Nursing
(n=70)
N (%)
I adhere to correct hand hygiene practices at all times 90(78.2) 28(62.22) 62(88.57)
Sufficient knowledge about hand hygiene practices is necessary
to
improve correct hand hygiene practices
82(71.30) 24(53.33) 58(82.86)
Sometimes I have more important things to do then hand
hygiene
74(51.2) 23(51.11) 51(56.66)
Emergencies and other priorities make hygiene more difficult at
times
90(78.26) 27(60.0) 63(90.0)
Wearing gloves reduce the need for hand hygiene 84(73.04) 22(48.89) 62(88.57)
I feel frustrated when others omit hand hygiene 73(63.47) 24(53.33) 49(70.0)
I am reluctant to ask others to engage in hand hygiene 73(63.47) 23(51.11) 50(71.43)
Newly qualified staff has not been properly instructed in hand
hygiene in their training
77(66.69) 26(57.78) 51(72.85)
I feel guilty if I omit hand hygiene 87(75.65) 25(55.56) 62(88.57)
Results and Recommended Improvements
Hand Hygiene Compliance
Table 1 depict attitude of health care provider towards health hygiene practice. Findings
revealed that majority of nursing health care workers had good attitudes. Further, findings
revealed that nursing personals had significantly good attitude towards hand hygiene
practices as compared to their counterparts. The percentage of correct responses of the two
groups of staff to the individual questions on hand hygiene attitude are given in Table 2
Table 1. Comparison of Attitude to Education Status of Health Care Providers
(n=100)
ATTITUDE
Total
(n=100)
N (%)
Medical(
n=30)
N (%)
Nursing
(n=70)
N (%)
I adhere to correct hand hygiene practices at all times 90(78.2) 28(62.22) 62(88.57)
Sufficient knowledge about hand hygiene practices is necessary
to
improve correct hand hygiene practices
82(71.30) 24(53.33) 58(82.86)
Sometimes I have more important things to do then hand
hygiene
74(51.2) 23(51.11) 51(56.66)
Emergencies and other priorities make hygiene more difficult at
times
90(78.26) 27(60.0) 63(90.0)
Wearing gloves reduce the need for hand hygiene 84(73.04) 22(48.89) 62(88.57)
I feel frustrated when others omit hand hygiene 73(63.47) 24(53.33) 49(70.0)
I am reluctant to ask others to engage in hand hygiene 73(63.47) 23(51.11) 50(71.43)
Newly qualified staff has not been properly instructed in hand
hygiene in their training
77(66.69) 26(57.78) 51(72.85)
I feel guilty if I omit hand hygiene 87(75.65) 25(55.56) 62(88.57)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
Adhering to hand hygiene practices is easy in the current setup 91(79.13) 27(60.0) 64(91.42)
Health care personnel should act as a role model for others 79(68.70) 28(62.22) 51(72.86)
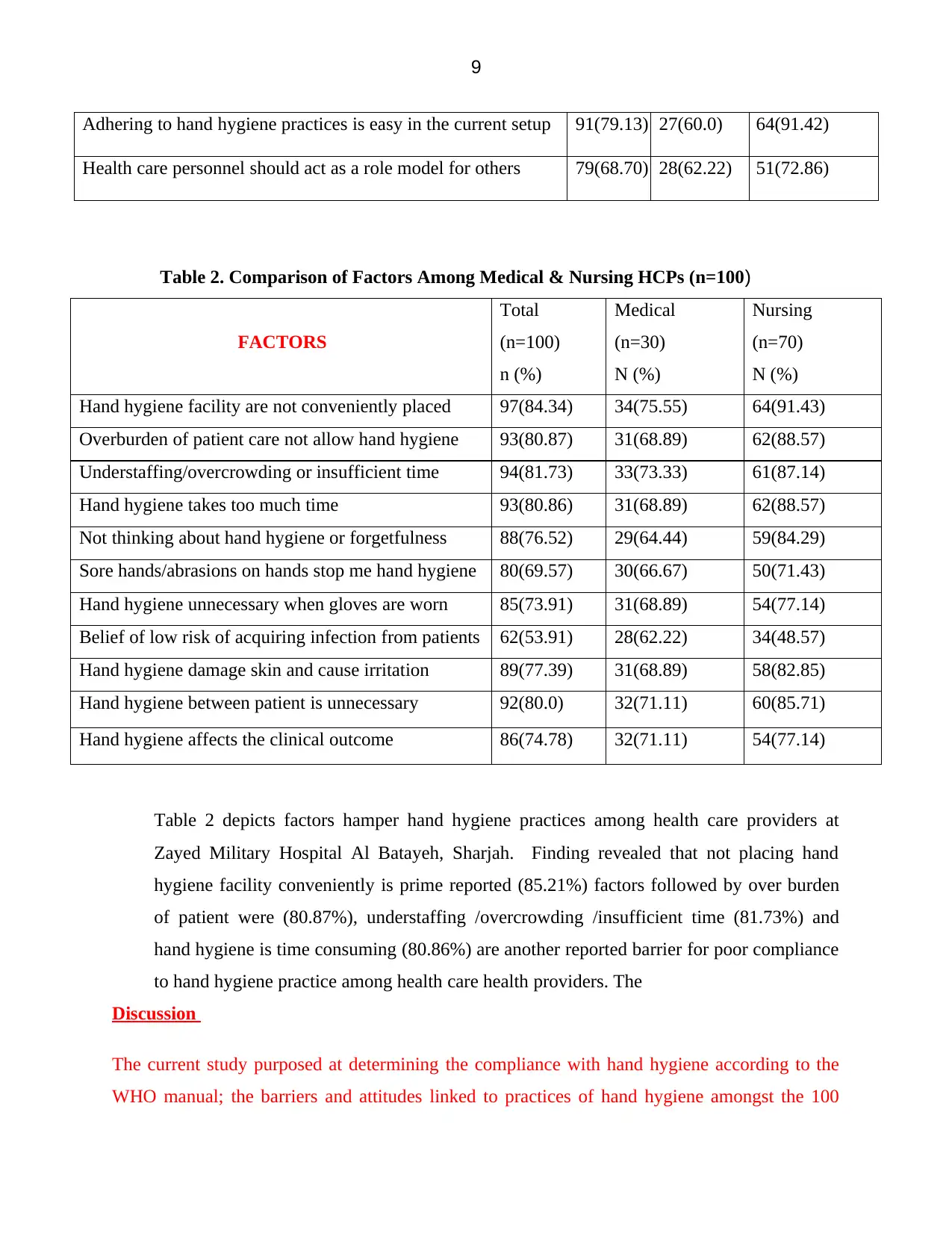
Table 2. Comparison of Factors Among Medical & Nursing HCPs (n=100)
FACTORS
Total
(n=100)
n (%)
Medical
(n=30)
N (%)
Nursing
(n=70)
N (%)
Hand hygiene facility are not conveniently placed 97(84.34) 34(75.55) 64(91.43)
Overburden of patient care not allow hand hygiene 93(80.87) 31(68.89) 62(88.57)
Understaffing/overcrowding or insufficient time 94(81.73) 33(73.33) 61(87.14)
Hand hygiene takes too much time 93(80.86) 31(68.89) 62(88.57)
Not thinking about hand hygiene or forgetfulness 88(76.52) 29(64.44) 59(84.29)
Sore hands/abrasions on hands stop me hand hygiene 80(69.57) 30(66.67) 50(71.43)
Hand hygiene unnecessary when gloves are worn 85(73.91) 31(68.89) 54(77.14)
Belief of low risk of acquiring infection from patients 62(53.91) 28(62.22) 34(48.57)
Hand hygiene damage skin and cause irritation 89(77.39) 31(68.89) 58(82.85)
Hand hygiene between patient is unnecessary 92(80.0) 32(71.11) 60(85.71)
Hand hygiene affects the clinical outcome 86(74.78) 32(71.11) 54(77.14)
Table 2 depicts factors hamper hand hygiene practices among health care providers at
Zayed Military Hospital Al Batayeh, Sharjah. Finding revealed that not placing hand
hygiene facility conveniently is prime reported (85.21%) factors followed by over burden
of patient were (80.87%), understaffing /overcrowding /insufficient time (81.73%) and
hand hygiene is time consuming (80.86%) are another reported barrier for poor compliance
to hand hygiene practice among health care health providers. The
Discussion
The current study purposed at determining the compliance with hand hygiene according to the
WHO manual; the barriers and attitudes linked to practices of hand hygiene amongst the 100
Adhering to hand hygiene practices is easy in the current setup 91(79.13) 27(60.0) 64(91.42)
Health care personnel should act as a role model for others 79(68.70) 28(62.22) 51(72.86)
Table 2. Comparison of Factors Among Medical & Nursing HCPs (n=100)
FACTORS
Total
(n=100)
n (%)
Medical
(n=30)
N (%)
Nursing
(n=70)
N (%)
Hand hygiene facility are not conveniently placed 97(84.34) 34(75.55) 64(91.43)
Overburden of patient care not allow hand hygiene 93(80.87) 31(68.89) 62(88.57)
Understaffing/overcrowding or insufficient time 94(81.73) 33(73.33) 61(87.14)
Hand hygiene takes too much time 93(80.86) 31(68.89) 62(88.57)
Not thinking about hand hygiene or forgetfulness 88(76.52) 29(64.44) 59(84.29)
Sore hands/abrasions on hands stop me hand hygiene 80(69.57) 30(66.67) 50(71.43)
Hand hygiene unnecessary when gloves are worn 85(73.91) 31(68.89) 54(77.14)
Belief of low risk of acquiring infection from patients 62(53.91) 28(62.22) 34(48.57)
Hand hygiene damage skin and cause irritation 89(77.39) 31(68.89) 58(82.85)
Hand hygiene between patient is unnecessary 92(80.0) 32(71.11) 60(85.71)
Hand hygiene affects the clinical outcome 86(74.78) 32(71.11) 54(77.14)
Table 2 depicts factors hamper hand hygiene practices among health care providers at
Zayed Military Hospital Al Batayeh, Sharjah. Finding revealed that not placing hand
hygiene facility conveniently is prime reported (85.21%) factors followed by over burden
of patient were (80.87%), understaffing /overcrowding /insufficient time (81.73%) and
hand hygiene is time consuming (80.86%) are another reported barrier for poor compliance
to hand hygiene practice among health care health providers. The
Discussion
The current study purposed at determining the compliance with hand hygiene according to the
WHO manual; the barriers and attitudes linked to practices of hand hygiene amongst the 100
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
healthcare providers at the Zayed Military Hospital. The present study outcomes unearthed that
faculty showcases higher compliance at ten percent to practise of hand hygiene followed by the
senior residents at 7.140 percent and the nursing and medical interns coming third at 6.71 percent
while the junior resident recording the least adherence at 1.03 percent. Among the HCWs, partial
compliance stood surprisingly high at 63.04 percent (Ataiyero, Dyson & Graham, 2018).
The current study outcomes remain in parallel to the research performed by Abdella MN at al. on
four hundred and sixty five heath care providers that showcased 16.5 percent full compliance
with hand hygiene requirements and practices. Nonetheless, in the research performed by Kumar
et al., a contradictory outcome stood unravelled since there remained a higher full adherence
levels at 76 percent to hand hygiene practices amongst the care providers working at the private
sector and the general compliance with practices of hand hygiene stood at 80.5 percent.
The study carried out by Shanu et al similarly discovered that observed adherence rates stood
higher at 67.08 percent as opposed to self-reported adherence at 90 percent among the
practitioners. In the past study performed in Saudi Arabia, sub-optimal adherence to practices of
hand hygiene was noted at 70, 18.8 as well as 9.10 percent among the students, nurses alongside
senior medical practitioners in that order. Such differences between the current and past studies
might be as a result of utilization of distinct methodologies, contexts/setting alongside use of
different instruments.
Additionally, 78.30 percent HCWs indicated the need for adherence with hand hygiene
requirements while 71.30 care providers held that full knowledge linked to practices of hand
hygiene remains the most significant to undertake hand-hygiene practices. Nonetheless, 78.260
percent of the HCWs held that these practices become challenging during the emergencies and
other priorities.
Nair et al. reported the similar outcomes in their study whereby 35.30 and 74.40 percent medical
alongside nursing students had assumed that they had better knowledge regarding practices of
hand hygiene in that order. An Indian study also discovered similar findings on staff nurses as
well as residents. Moreover, it was highlighted that solely 21.40 percent of medical students
alongside 61.80 percent of nursing students indicated adherence to correct practices of hand
healthcare providers at the Zayed Military Hospital. The present study outcomes unearthed that
faculty showcases higher compliance at ten percent to practise of hand hygiene followed by the
senior residents at 7.140 percent and the nursing and medical interns coming third at 6.71 percent
while the junior resident recording the least adherence at 1.03 percent. Among the HCWs, partial
compliance stood surprisingly high at 63.04 percent (Ataiyero, Dyson & Graham, 2018).
The current study outcomes remain in parallel to the research performed by Abdella MN at al. on
four hundred and sixty five heath care providers that showcased 16.5 percent full compliance
with hand hygiene requirements and practices. Nonetheless, in the research performed by Kumar
et al., a contradictory outcome stood unravelled since there remained a higher full adherence
levels at 76 percent to hand hygiene practices amongst the care providers working at the private
sector and the general compliance with practices of hand hygiene stood at 80.5 percent.
The study carried out by Shanu et al similarly discovered that observed adherence rates stood
higher at 67.08 percent as opposed to self-reported adherence at 90 percent among the
practitioners. In the past study performed in Saudi Arabia, sub-optimal adherence to practices of
hand hygiene was noted at 70, 18.8 as well as 9.10 percent among the students, nurses alongside
senior medical practitioners in that order. Such differences between the current and past studies
might be as a result of utilization of distinct methodologies, contexts/setting alongside use of
different instruments.
Additionally, 78.30 percent HCWs indicated the need for adherence with hand hygiene
requirements while 71.30 care providers held that full knowledge linked to practices of hand
hygiene remains the most significant to undertake hand-hygiene practices. Nonetheless, 78.260
percent of the HCWs held that these practices become challenging during the emergencies and
other priorities.
Nair et al. reported the similar outcomes in their study whereby 35.30 and 74.40 percent medical
alongside nursing students had assumed that they had better knowledge regarding practices of
hand hygiene in that order. An Indian study also discovered similar findings on staff nurses as
well as residents. Moreover, it was highlighted that solely 21.40 percent of medical students
alongside 61.80 percent of nursing students indicated adherence to correct practices of hand
11
hygiene at all points. Also, the past studies have indicated that staff nurses negate hand hygiene
because of fear of frightened skin challenges like dermatitis.
Additionally, in the current research, 85.210 percent of the HCWs held that facilities of hand
hygiene are never conveniently situated and 80.870 percent of the care workers indicated that
due to overburden of caring for patients, practices of hand hygiene are never adhered to
effectively. It is further unravelled that 81.730 percent of HCWs were either understaffed or
overcrowded or insufficient time, all of which culminate in poor compliance with these practices
of hand hygiene.
The current study outcomes remain aligned to the previous research performed by Segum et al.
which showed that 66.80 percent of HCWs were convinced that insufficient facilities for hand
hygiene existed. Similarly, nearly 35.70 percent of HCWs indicated that that time limitation was
a key obstacle to full adherence to hand hygiene practices. In the same manner, 14.30 percent of
HCWs felt that heavy patient workload or overburden as another key deterrence to full
adherence. The existing literature further indicate that hand rub solutions’ availability at patient
bedside makes the patients to increase their compliance to practices for hand hygiene.
Conclusion and Recommendation
Present study revealed a very poor adherence to hand hygiene practices among health care
providers at a tertiary care teaching hospital. However, study findings recommended a hand on
training or periodic in-service education programme to sensitize HCPs. Findings also suggest to
make it mandatory to undergo a training programme for newly joined HCPs to develop
understanding about the importance of hand hygiene practices.
Action Plan
There are two action plans for this study project. The first action plan is to perform a training
program for the healthcare providers in Zayed Military Hospital Al Batayeh by the infection
control department. The training program will consist of a lecture about the importance of hand
hygiene, types, technique, complication of the non-compliance of the hand hygiene in addition to
the hand hygiene practice. The training program will be conducted in Zayed Military Hospital
AL Batayeh, 4th floor, and lecture hall on Wednesday 31/Jul/2019.
hygiene at all points. Also, the past studies have indicated that staff nurses negate hand hygiene
because of fear of frightened skin challenges like dermatitis.
Additionally, in the current research, 85.210 percent of the HCWs held that facilities of hand
hygiene are never conveniently situated and 80.870 percent of the care workers indicated that
due to overburden of caring for patients, practices of hand hygiene are never adhered to
effectively. It is further unravelled that 81.730 percent of HCWs were either understaffed or
overcrowded or insufficient time, all of which culminate in poor compliance with these practices
of hand hygiene.
The current study outcomes remain aligned to the previous research performed by Segum et al.
which showed that 66.80 percent of HCWs were convinced that insufficient facilities for hand
hygiene existed. Similarly, nearly 35.70 percent of HCWs indicated that that time limitation was
a key obstacle to full adherence to hand hygiene practices. In the same manner, 14.30 percent of
HCWs felt that heavy patient workload or overburden as another key deterrence to full
adherence. The existing literature further indicate that hand rub solutions’ availability at patient
bedside makes the patients to increase their compliance to practices for hand hygiene.
Conclusion and Recommendation
Present study revealed a very poor adherence to hand hygiene practices among health care
providers at a tertiary care teaching hospital. However, study findings recommended a hand on
training or periodic in-service education programme to sensitize HCPs. Findings also suggest to
make it mandatory to undergo a training programme for newly joined HCPs to develop
understanding about the importance of hand hygiene practices.
Action Plan
There are two action plans for this study project. The first action plan is to perform a training
program for the healthcare providers in Zayed Military Hospital Al Batayeh by the infection
control department. The training program will consist of a lecture about the importance of hand
hygiene, types, technique, complication of the non-compliance of the hand hygiene in addition to
the hand hygiene practice. The training program will be conducted in Zayed Military Hospital
AL Batayeh, 4th floor, and lecture hall on Wednesday 31/Jul/2019.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 22
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.