Report on Hashimoto Disease: Pathophysiology and Diagnosis
VerifiedAdded on 2022/10/17
|8
|1600
|5
Report
AI Summary
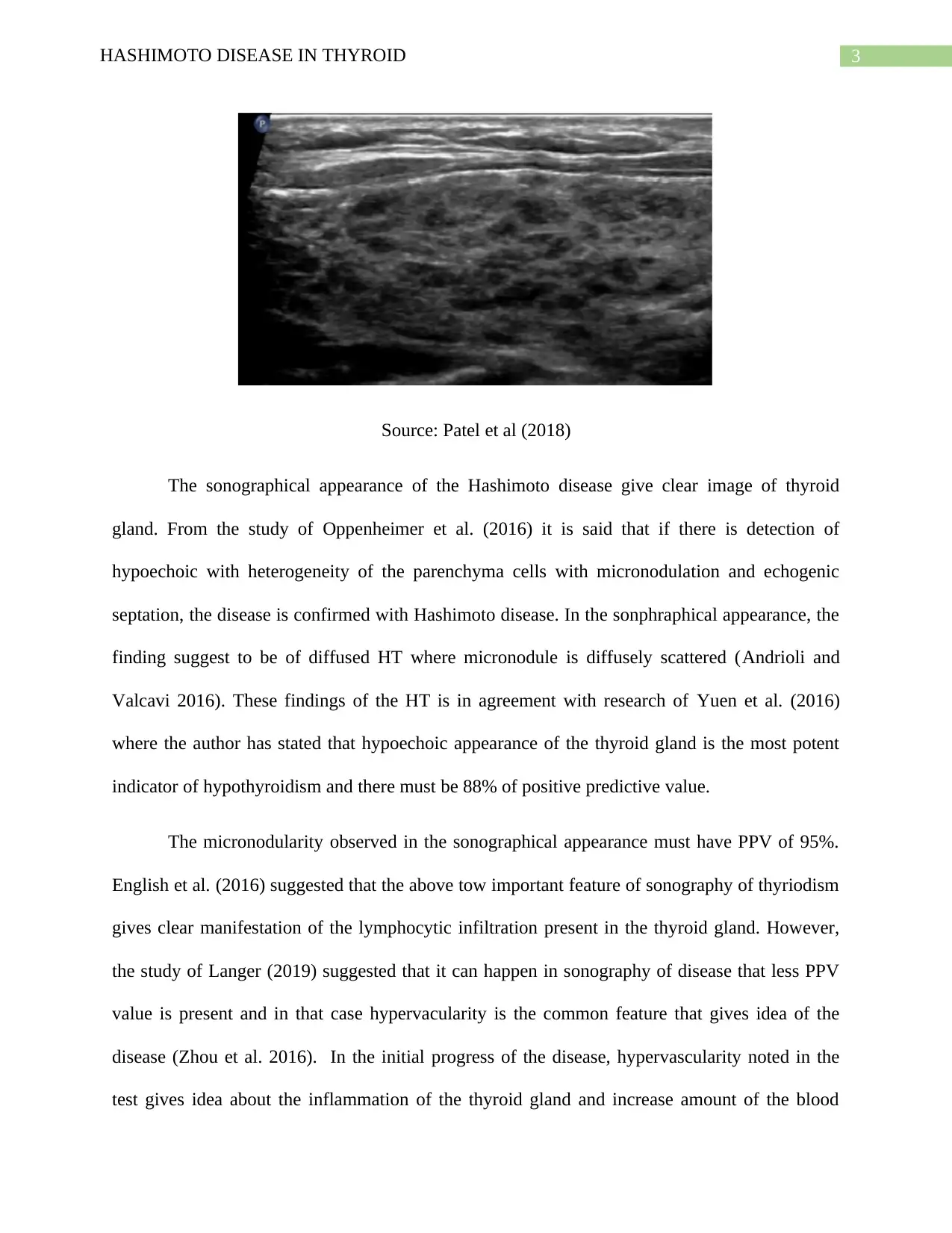
This report provides a comprehensive overview of Hashimoto's disease, a form of hypothyroidism characterized by low T3 and T4 hormone secretion and high TSH levels. It delves into the pathophysiology, explaining the autoimmune processes involving CD4 and T helper cells, the role of autoantibodies, and the destruction of thyroid gland parenchyma. The report also examines the sonographical appearance of Hashimoto's disease, detailing the significance of echogenicity, heterogeneity, micronodularity, and hypervascularity in diagnosis. It references key studies and findings related to these features, highlighting their importance in identifying the disease and understanding its progression. The report emphasizes the value of sonography in diagnosing Hashimoto's disease and the correlation between sonographical findings and the underlying lymphocytic infiltration of the thyroid gland.

1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.