Case Study: HCC Diagnosis, Treatment, and Patient Outcome Analysis
VerifiedAdded on 2022/11/19
|1
|1085
|72
Case Study
AI Summary
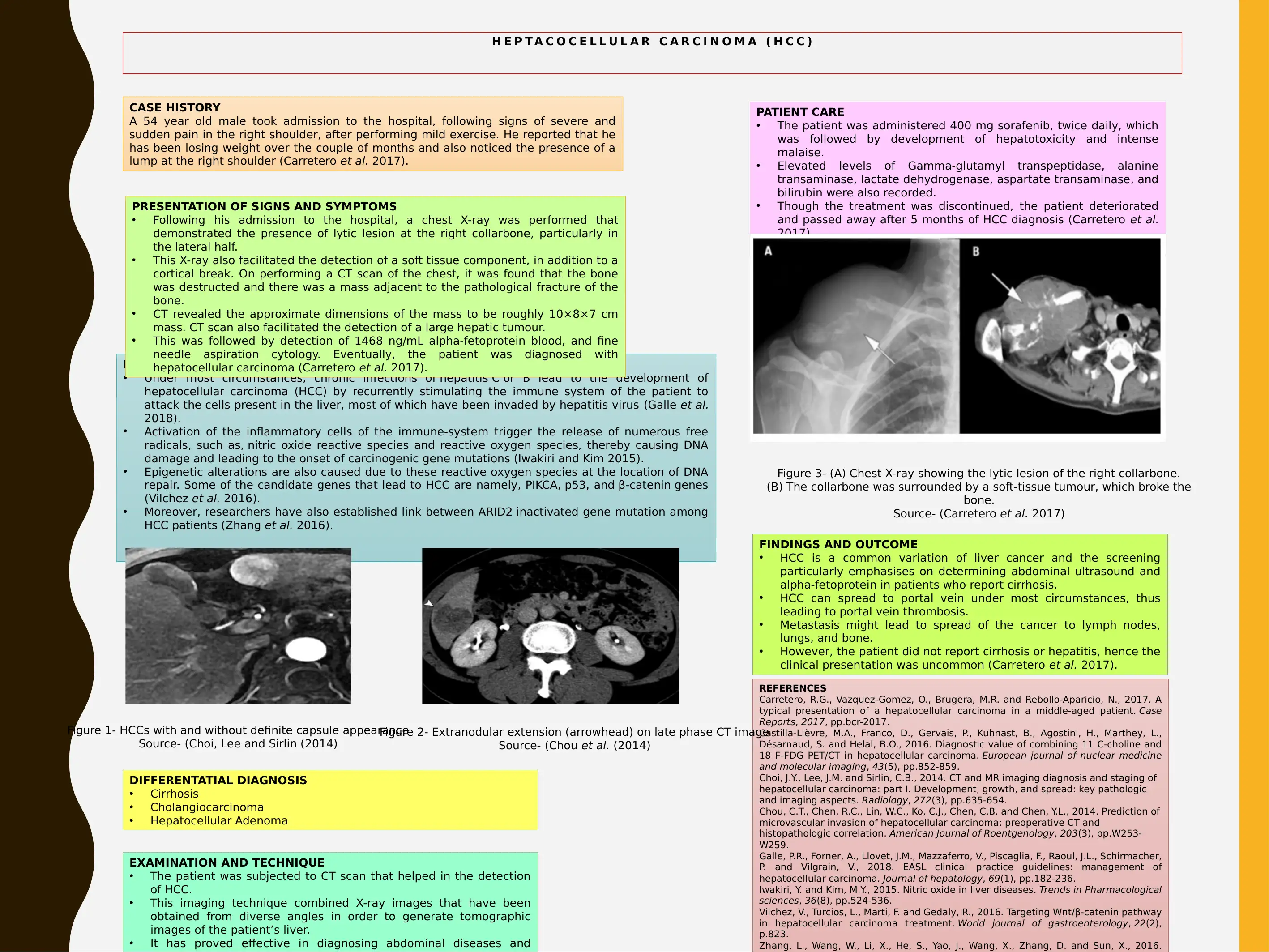
This case study details the diagnosis and treatment of a 54-year-old male patient diagnosed with hepatocellular carcinoma (HCC). The patient presented with right shoulder pain and weight loss, leading to the detection of a lump. Differential diagnoses included cirrhosis, cholangiocarcinoma, and hepatocellular adenoma. The study outlines the pathophysiology, emphasizing the role of chronic hepatitis infections and the resulting DNA damage. The patient's care involved sorafenib treatment, which was discontinued due to hepatotoxicity. Diagnostic methods included chest X-rays, CT scans, and alpha-fetoprotein blood tests. The findings revealed a lytic lesion in the right collarbone and a large hepatic tumor. The outcome was fatal, with the patient passing away five months after diagnosis. The case highlights the importance of imaging techniques like CT scans in diagnosing HCC and the challenges in treating advanced stages of the disease. References to relevant research papers are also included.

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.