Application of Public Health Tools to Analyze Health Inequality
VerifiedAdded on 2020/06/05
|12
|2830
|126
Report
AI Summary
This report delves into the tools employed by public health practitioners to address health inequality, focusing on health equity audits (HEA) and health impact assessments (HIA). It examines how HEAs assess determinants of health and health service access, aiming to reduce inequalities through policy and strategies. The report outlines the HEA cycle, including steps like partner agreement, equity profiling, and action prioritization, using data to inform decisions. Various tools and variables for success are discussed, alongside real-world examples of HEA implementation, such as in Southwark PCT and the Borough of Poole, demonstrating how these tools drive changes in resource allocation and service delivery to reduce disparities. The report also provides data analysis of population inequalities based on age, gender, and geographical area, and considers factors like smoking and socio-economic circumstances. The decision of theme for HEA will be affected by national what's more, neighbourhood needs, and might be picked through a procedure including the PCT board, proficient official advisory group, the executive of general well-being, and key accomplices in the LSP.
Knowledge of Health
Inequality through use of
Tool used by Public health
practitioners
Inequality through use of
Tool used by Public health
practitioners
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
INTRODUCTION...........................................................................................................................3
MAIN BODY...................................................................................................................................3
CONCLUSION..............................................................................................................................11
REFERENCES..............................................................................................................................12
INTRODUCTION...........................................................................................................................3
MAIN BODY...................................................................................................................................3
CONCLUSION..............................................................................................................................11
REFERENCES..............................................................................................................................12
INTRODUCTION
The main aims of National Health Service would be that of undertaking all audit which
are related to that of health equity audits (HEA). Under this process practitioner will be
examining how would all determinants of health will be carried on and also accessing health
service. It will also be carrying out the task of reducing health inequality within various sectors
by building up good governance policy and strategies. In this current topic where we would be
exploring the topic which says about what are tools that could be applied at time of addressing
health inequality. This will also be covering determination about the data which was made
available so that population health and inequality.
MAIN BODY
What is health equity audit?
Under this assessment it will be easy to assess the difference between resource which are
for health equalities and that of health inequality. Whole population could be under these
procedures which is meant to define the inequality that too under conditions like that of
employment, transport or housing. Various kinds of risk are to be included and analysed within
process like that of smoking or it could also be obesity these both are said to be lifestyle which is
followed by people. Health Impact Assessment (HIA) is also a tool that is adaptation of
proposals which could be before they are implemented (Brownson, Fielding & Green, 2018). In
this it could be noted that use of making the case that would be briefing about how would all
things be impacting health like that of all factors which are economic, social and environmental
one. These factors could be impacting both health equalities and inequalities of a person.
It could be said that health inequalities is the clear difference between population of
people who are living in various geographical area, age, disabilities or gender which is mainly
that of their equalities of health among them all. While on the other hand health inequity would
be defined to as if the people who are living under various geographical areas and are not getting
the specified health benefits or service then what kind of separate health outcomes could have
been arise (Green & Thorogood, 2018). The process of distributing benefits of health service on
equal basis which could be according to the need of specified group of people would be known
to as equity.
The main aims of National Health Service would be that of undertaking all audit which
are related to that of health equity audits (HEA). Under this process practitioner will be
examining how would all determinants of health will be carried on and also accessing health
service. It will also be carrying out the task of reducing health inequality within various sectors
by building up good governance policy and strategies. In this current topic where we would be
exploring the topic which says about what are tools that could be applied at time of addressing
health inequality. This will also be covering determination about the data which was made
available so that population health and inequality.
MAIN BODY
What is health equity audit?
Under this assessment it will be easy to assess the difference between resource which are
for health equalities and that of health inequality. Whole population could be under these
procedures which is meant to define the inequality that too under conditions like that of
employment, transport or housing. Various kinds of risk are to be included and analysed within
process like that of smoking or it could also be obesity these both are said to be lifestyle which is
followed by people. Health Impact Assessment (HIA) is also a tool that is adaptation of
proposals which could be before they are implemented (Brownson, Fielding & Green, 2018). In
this it could be noted that use of making the case that would be briefing about how would all
things be impacting health like that of all factors which are economic, social and environmental
one. These factors could be impacting both health equalities and inequalities of a person.
It could be said that health inequalities is the clear difference between population of
people who are living in various geographical area, age, disabilities or gender which is mainly
that of their equalities of health among them all. While on the other hand health inequity would
be defined to as if the people who are living under various geographical areas and are not getting
the specified health benefits or service then what kind of separate health outcomes could have
been arise (Green & Thorogood, 2018). The process of distributing benefits of health service on
equal basis which could be according to the need of specified group of people would be known
to as equity.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Scope of HEA-
There are various tools which are to be used in health equity audit and kinds of
inequalities like that of lifestyles (diet, smoking habits, physical activity or social network),
socio-economic or environmental circumstance (employment, housing, education or that of
transportation). This must be used because of reason like that to bring changes, improving health
under determinants of good health criteria and then reducing health inequalities among people of
same class and range.
Health equity audit cycle-
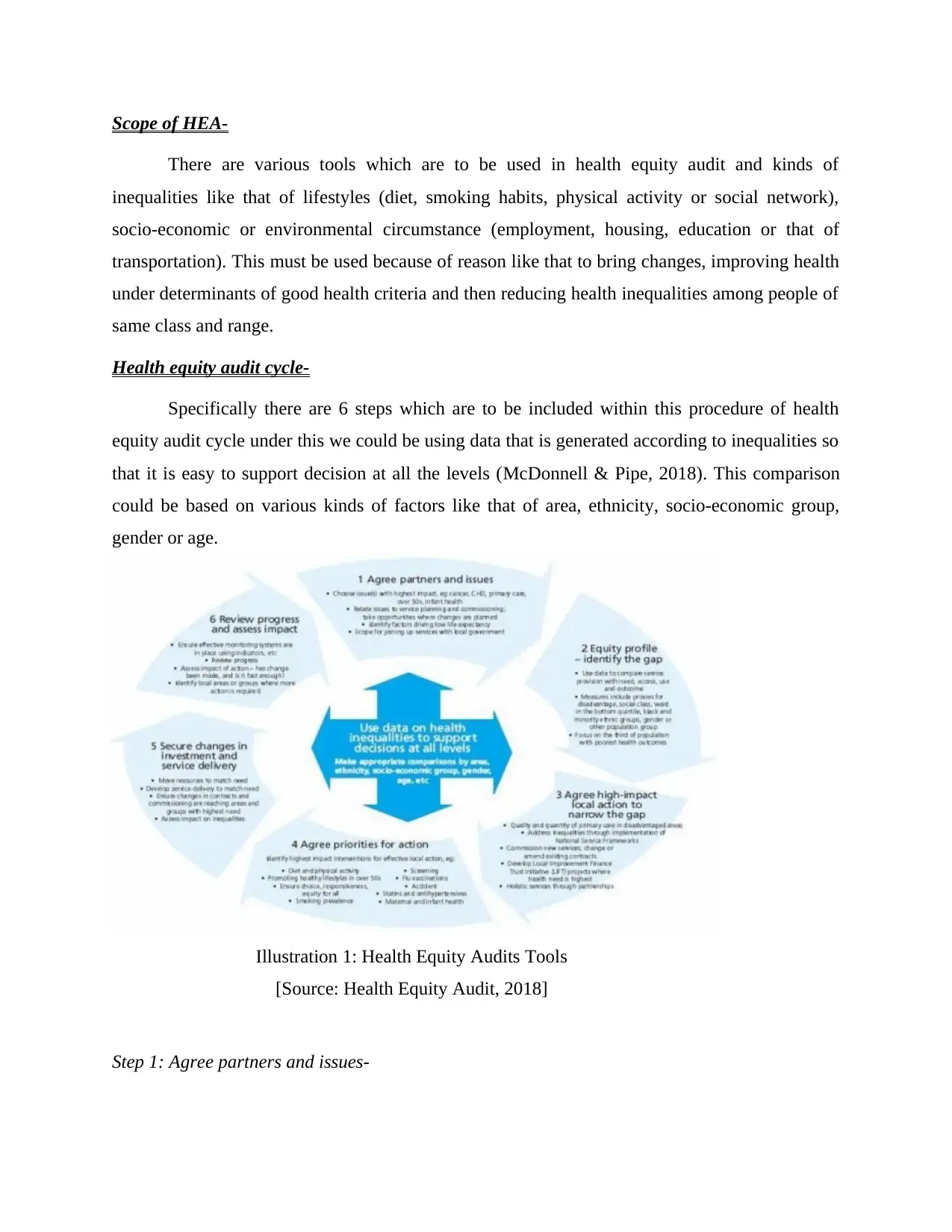
Specifically there are 6 steps which are to be included within this procedure of health
equity audit cycle under this we could be using data that is generated according to inequalities so
that it is easy to support decision at all the levels (McDonnell & Pipe, 2018). This comparison
could be based on various kinds of factors like that of area, ethnicity, socio-economic group,
gender or age.
Step 1: Agree partners and issues-
Illustration 1: Health Equity Audits Tools
[Source: Health Equity Audit, 2018]
There are various tools which are to be used in health equity audit and kinds of
inequalities like that of lifestyles (diet, smoking habits, physical activity or social network),
socio-economic or environmental circumstance (employment, housing, education or that of
transportation). This must be used because of reason like that to bring changes, improving health
under determinants of good health criteria and then reducing health inequalities among people of
same class and range.
Health equity audit cycle-
Specifically there are 6 steps which are to be included within this procedure of health
equity audit cycle under this we could be using data that is generated according to inequalities so
that it is easy to support decision at all the levels (McDonnell & Pipe, 2018). This comparison
could be based on various kinds of factors like that of area, ethnicity, socio-economic group,
gender or age.
Step 1: Agree partners and issues-
Illustration 1: Health Equity Audits Tools
[Source: Health Equity Audit, 2018]
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Pick issue(s) with most noteworthy effect, e.g. tumour, CHD, essential care, more than 50 s,
newborn child well-being
• Relate issues to benefit arranging and appointing; accept open doors where changes are
arranged
• Identify factors driving bastard hope
• Scope for signing up administrations with nearby government
Step 2: Equity profiles- identification of gap-
Utilize information to contrast benefit arrangement and need, access, utilize and result
• Measures incorporate intermediaries for drawback, social class, ward in the base quantile, dark
and minority ethnic gatherings, sex or other populace aggregate
• Focus on the third of populace with the poorest well-being results
Step 3: Agree high impact local action to narrow gap-
Quality and amount of essential care in impeded zones
• Address disparities through execution of National Service Frameworks Commission new
administrations; change or correct existing contracts
• Develop Local Improvement Finance Trust Initiative (LIFT) ventures where well being need is
most elevated
• Holistic administrations through associations
Step 4: Agree priorities for action-
Recognize on most elevated effect intercessions for powerful neighbourhood activity, e.g.: Diet
and physical movement
• Promoting sound ways of life in more than 50 s
• Ensure decision, responsiveness, value for all
• Smoking pervasiveness Screening
• Flu immunizations
newborn child well-being
• Relate issues to benefit arranging and appointing; accept open doors where changes are
arranged
• Identify factors driving bastard hope
• Scope for signing up administrations with nearby government
Step 2: Equity profiles- identification of gap-
Utilize information to contrast benefit arrangement and need, access, utilize and result
• Measures incorporate intermediaries for drawback, social class, ward in the base quantile, dark
and minority ethnic gatherings, sex or other populace aggregate
• Focus on the third of populace with the poorest well-being results
Step 3: Agree high impact local action to narrow gap-
Quality and amount of essential care in impeded zones
• Address disparities through execution of National Service Frameworks Commission new
administrations; change or correct existing contracts
• Develop Local Improvement Finance Trust Initiative (LIFT) ventures where well being need is
most elevated
• Holistic administrations through associations
Step 4: Agree priorities for action-
Recognize on most elevated effect intercessions for powerful neighbourhood activity, e.g.: Diet
and physical movement
• Promoting sound ways of life in more than 50 s
• Ensure decision, responsiveness, value for all
• Smoking pervasiveness Screening
• Flu immunizations
• Accident
• Stains and antihypertensive
• Maternal and baby well-being
Step 5: Secure changes in investment and service delivery-
Move assets to coordinate need
• Develop benefit conveyance to coordinate need
• Ensure changes in contracts and charging are achieving zones and gatherings with most
noteworthy need
• Assess effect imbalances
Step 6: Review progress and assess impact-
Guarantee viable checking frameworks are set up utilizing markers, and so on
• Review advance
• Assess effect of activity – has change been made, and is it sufficiently quick?
• Identify neighbourhoods bunches where more 6 Review advance and evaluate affect activity is
required.
All the available inequalities are to be classified into various groups which are majorly on
bases of age, gender, disabilities, geographical area and ethnicity (de Wit & Meijering, 2018). So
the data on which we would be working could be categorised into age from 0-85 years of age and
gender which could be both male and female. The sub zone or kingdom which is taken as 14 and
15. The term age standardisation could be one that is adjusting all rate so that difference of age
into whole population could be made according to various time period or geographical areas
could also be included within these criteria.
Population inequalities based on data available:
• Stains and antihypertensive
• Maternal and baby well-being
Step 5: Secure changes in investment and service delivery-
Move assets to coordinate need
• Develop benefit conveyance to coordinate need
• Ensure changes in contracts and charging are achieving zones and gatherings with most
noteworthy need
• Assess effect imbalances
Step 6: Review progress and assess impact-
Guarantee viable checking frameworks are set up utilizing markers, and so on
• Review advance
• Assess effect of activity – has change been made, and is it sufficiently quick?
• Identify neighbourhoods bunches where more 6 Review advance and evaluate affect activity is
required.
All the available inequalities are to be classified into various groups which are majorly on
bases of age, gender, disabilities, geographical area and ethnicity (de Wit & Meijering, 2018). So
the data on which we would be working could be categorised into age from 0-85 years of age and
gender which could be both male and female. The sub zone or kingdom which is taken as 14 and
15. The term age standardisation could be one that is adjusting all rate so that difference of age
into whole population could be made according to various time period or geographical areas
could also be included within these criteria.
Population inequalities based on data available:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
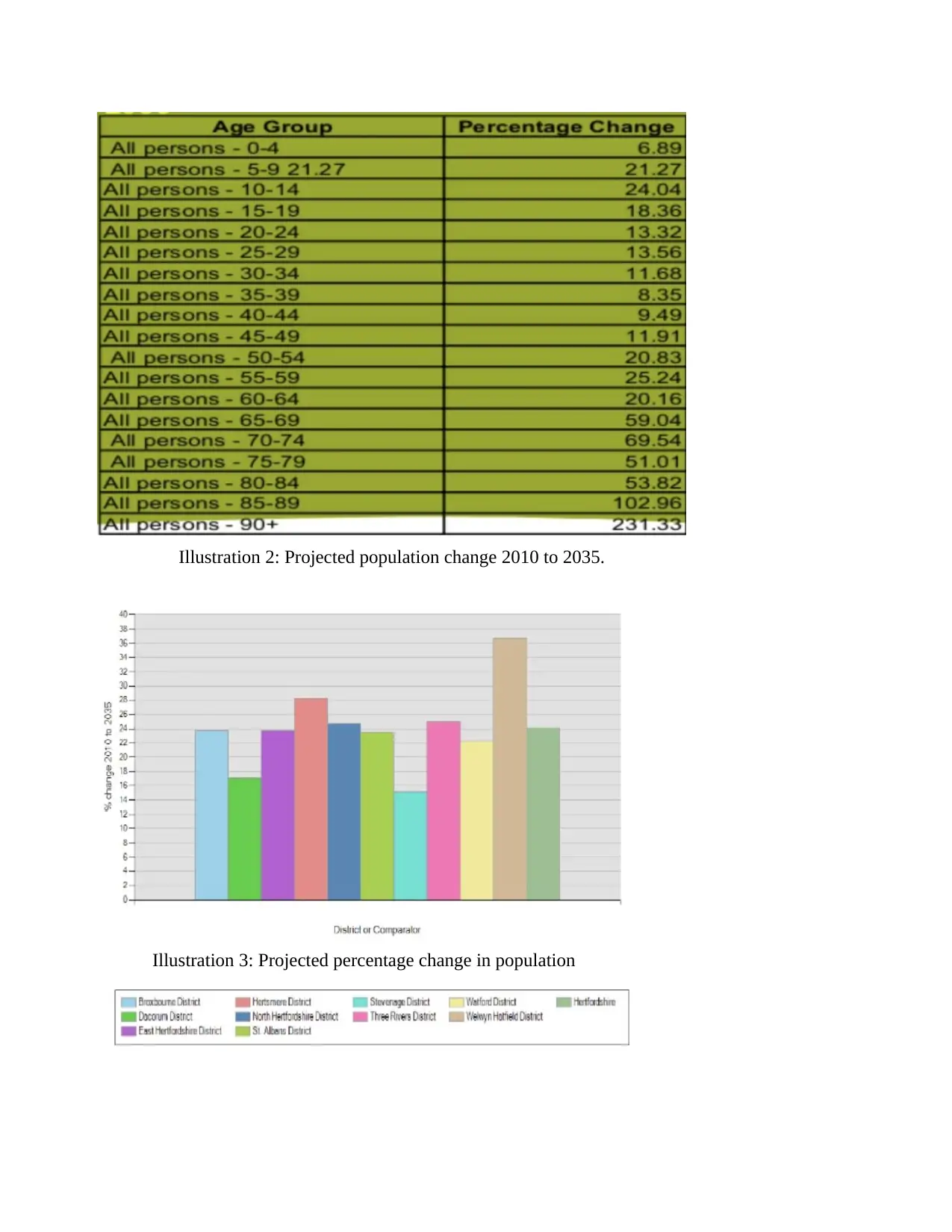
Illustration 2: Projected population change 2010 to 2035.
Illustration 3: Projected percentage change in population
Illustration 3: Projected percentage change in population
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
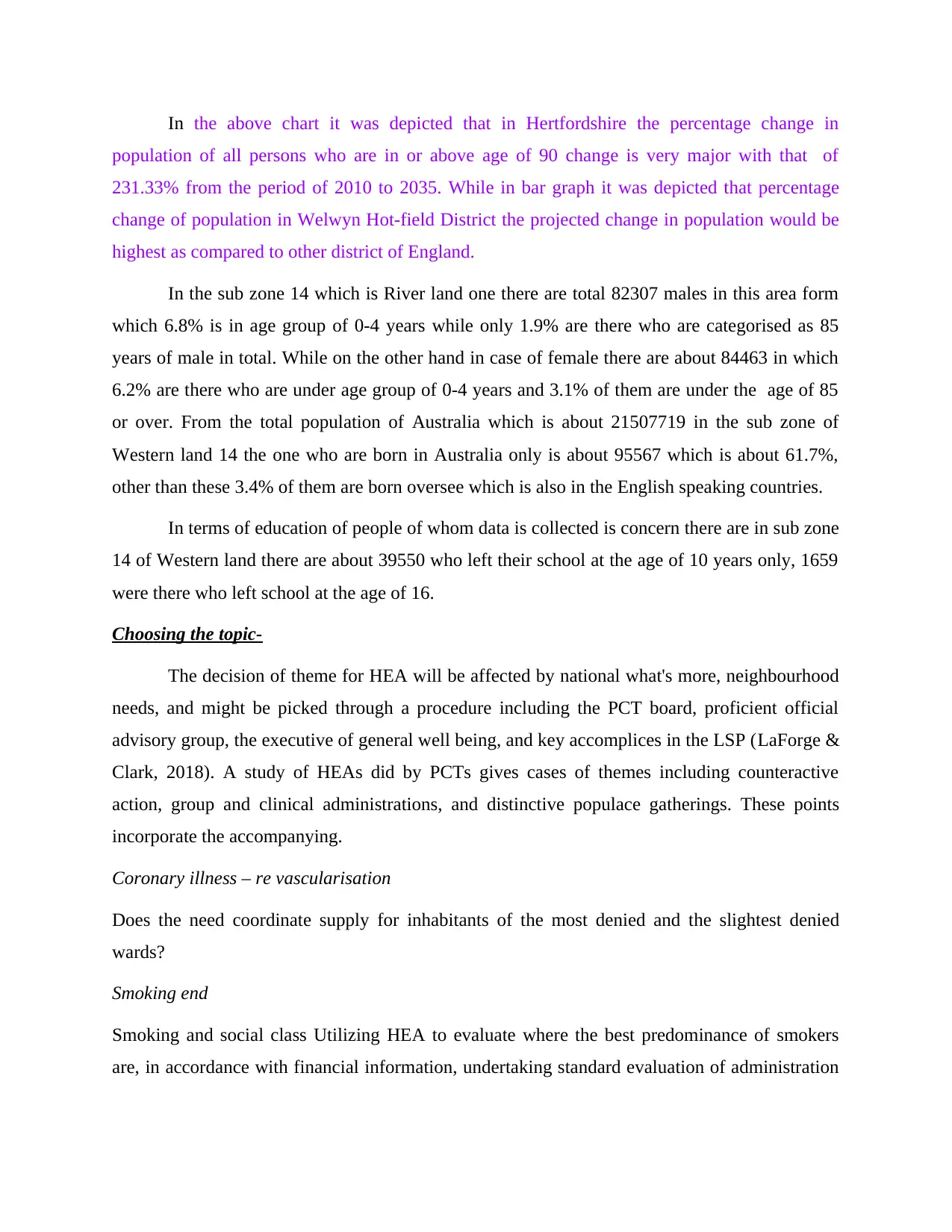
In the above chart it was depicted that in Hertfordshire the percentage change in
population of all persons who are in or above age of 90 change is very major with that of
231.33% from the period of 2010 to 2035. While in bar graph it was depicted that percentage
change of population in Welwyn Hot-field District the projected change in population would be
highest as compared to other district of England.
In the sub zone 14 which is River land one there are total 82307 males in this area form
which 6.8% is in age group of 0-4 years while only 1.9% are there who are categorised as 85
years of male in total. While on the other hand in case of female there are about 84463 in which
6.2% are there who are under age group of 0-4 years and 3.1% of them are under the age of 85
or over. From the total population of Australia which is about 21507719 in the sub zone of
Western land 14 the one who are born in Australia only is about 95567 which is about 61.7%,
other than these 3.4% of them are born oversee which is also in the English speaking countries.
In terms of education of people of whom data is collected is concern there are in sub zone
14 of Western land there are about 39550 who left their school at the age of 10 years only, 1659
were there who left school at the age of 16.
Choosing the topic-
The decision of theme for HEA will be affected by national what's more, neighbourhood
needs, and might be picked through a procedure including the PCT board, proficient official
advisory group, the executive of general well being, and key accomplices in the LSP (LaForge &
Clark, 2018). A study of HEAs did by PCTs gives cases of themes including counteractive
action, group and clinical administrations, and distinctive populace gatherings. These points
incorporate the accompanying.
Coronary illness – re vascularisation
Does the need coordinate supply for inhabitants of the most denied and the slightest denied
wards?
Smoking end
Smoking and social class Utilizing HEA to evaluate where the best predominance of smokers
are, in accordance with financial information, undertaking standard evaluation of administration
population of all persons who are in or above age of 90 change is very major with that of
231.33% from the period of 2010 to 2035. While in bar graph it was depicted that percentage
change of population in Welwyn Hot-field District the projected change in population would be
highest as compared to other district of England.
In the sub zone 14 which is River land one there are total 82307 males in this area form
which 6.8% is in age group of 0-4 years while only 1.9% are there who are categorised as 85
years of male in total. While on the other hand in case of female there are about 84463 in which
6.2% are there who are under age group of 0-4 years and 3.1% of them are under the age of 85
or over. From the total population of Australia which is about 21507719 in the sub zone of
Western land 14 the one who are born in Australia only is about 95567 which is about 61.7%,
other than these 3.4% of them are born oversee which is also in the English speaking countries.
In terms of education of people of whom data is collected is concern there are in sub zone
14 of Western land there are about 39550 who left their school at the age of 10 years only, 1659
were there who left school at the age of 16.
Choosing the topic-
The decision of theme for HEA will be affected by national what's more, neighbourhood
needs, and might be picked through a procedure including the PCT board, proficient official
advisory group, the executive of general well being, and key accomplices in the LSP (LaForge &
Clark, 2018). A study of HEAs did by PCTs gives cases of themes including counteractive
action, group and clinical administrations, and distinctive populace gatherings. These points
incorporate the accompanying.
Coronary illness – re vascularisation
Does the need coordinate supply for inhabitants of the most denied and the slightest denied
wards?
Smoking end
Smoking and social class Utilizing HEA to evaluate where the best predominance of smokers
are, in accordance with financial information, undertaking standard evaluation of administration
arrangement at both pro also, essential care level, and utilizing this data to design also,
commission future smoking suspension benefit arrangement (Wyatt, Cook & McKevitt, 2018).
Access issues – access to nearby well-being administrations
How are individuals from dark and minority ethnic groups utilizing essential and optional care
administrations?
Diabetes – podiatry
Using HEA to take a gander at access to dietetics and podiatry for South Asian people
group. Well-being going by and youngsters' administrations school nursing Is school nursing
time apportioned in connection to require and estimated by instructive achievement free school
dinners (Matwiejczyk & Coveney, 2018). Zone based arranging and advancement Using HEA to
take a gander at value of well-being and administration arrangement in one a player in the ward
to illuminate the improvement of an area administration pilot.
Other theme zones, distinguished amid the HDA's lord classes on HEA, are developing,
which are less NHS focused. An illustration may be a HEA taking a gander at clients of a
gathering's recreation administrations to evaluate which populace gatherings could profit most
from physical movement (contrasted and, for instance, the levels of coronary illness specifically
populace bunches in the precinct) – relaxation administrations would be retargeted thus.
Variables for progress The accompanying achievement factors have been distinguished (Making
the case: health equity audit, 2018).
• Availability of good quality information
• Knowledge and comprehension of accessible information (eg with help from general well-
being observatories)
• Training in HEA
• Capacity/staff and administration to do HEA
• Support and no more senior levels (PCT and vital well-being specialist)
• Support from partners outside to the PCT
commission future smoking suspension benefit arrangement (Wyatt, Cook & McKevitt, 2018).
Access issues – access to nearby well-being administrations
How are individuals from dark and minority ethnic groups utilizing essential and optional care
administrations?
Diabetes – podiatry
Using HEA to take a gander at access to dietetics and podiatry for South Asian people
group. Well-being going by and youngsters' administrations school nursing Is school nursing
time apportioned in connection to require and estimated by instructive achievement free school
dinners (Matwiejczyk & Coveney, 2018). Zone based arranging and advancement Using HEA to
take a gander at value of well-being and administration arrangement in one a player in the ward
to illuminate the improvement of an area administration pilot.
Other theme zones, distinguished amid the HDA's lord classes on HEA, are developing,
which are less NHS focused. An illustration may be a HEA taking a gander at clients of a
gathering's recreation administrations to evaluate which populace gatherings could profit most
from physical movement (contrasted and, for instance, the levels of coronary illness specifically
populace bunches in the precinct) – relaxation administrations would be retargeted thus.
Variables for progress The accompanying achievement factors have been distinguished (Making
the case: health equity audit, 2018).
• Availability of good quality information
• Knowledge and comprehension of accessible information (eg with help from general well-
being observatories)
• Training in HEA
• Capacity/staff and administration to do HEA
• Support and no more senior levels (PCT and vital well-being specialist)
• Support from partners outside to the PCT
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
• Understanding what execution will mean at the arranging stage (and tying in with charging
timetable)
• Sharing great practice, assets and support with others completing HEA.
Having any kind of effect – illustrations
The HEA cycle isn't finished until the point when something changes to decrease
imbalances certifiably (eg asset designation, dispatching, benefit arrangement or care results).
There are cases of HEA prompting an adjustment in benefit arrangement or on the other hand
asset portion and, therefore, disparities being decreased (NHS Health Checks in Nottingham City,
2018). The accompanying give great outlines of how the finish HEA cycle can work.
Case 1: Southwark PCT
A HEA for the number of inhabitants in South Bermondsey North Livesey
Neighbourhood Renewal Area was attempted by Southwark PCT Public Health. It was created in
association with the PCT's Locality Director and Southwark Committee's Area Renewal Officer.
A value profile of well-being what's more, access to administrations for the group was finished
what's more, displayed to the Neighbourhood Management Group what more, the Health and
Worklessness subgroup of Southwark Partnership LSP. To date, the value profile has been
utilized by the Neighbourhood Management Group for need setting. It has educated the
improvement of a Neighbourhood Health Advancement Team, and has been instrumental in the
choice to make the soundness of voyagers a point of convergence. The subsequent stages
incorporate refreshing the value profile as more data winds up accessible, and growing further
suggestions what's more, educating the anticipating activity process.
Illustration 2: Borough of Poole, Young
Individuals' HEA The Borough of Poole embraced a HEA for powerless youngsters and
youngsters to recognize needs and educate speculation decisions for the Children's Fund, the
Local Deterrent Strategy, Every Child Matters and the Children's Act. Organizations working
with kids and youngsters in Poole were associated with the HEA (Health Equity Audit, 2018).
Jan Sayers, Poole Local Government, states: territories where kids and youthful individuals have
the best needs were distinguished obviously from the HEA of both statistic data and execution
timetable)
• Sharing great practice, assets and support with others completing HEA.
Having any kind of effect – illustrations
The HEA cycle isn't finished until the point when something changes to decrease
imbalances certifiably (eg asset designation, dispatching, benefit arrangement or care results).
There are cases of HEA prompting an adjustment in benefit arrangement or on the other hand
asset portion and, therefore, disparities being decreased (NHS Health Checks in Nottingham City,
2018). The accompanying give great outlines of how the finish HEA cycle can work.
Case 1: Southwark PCT
A HEA for the number of inhabitants in South Bermondsey North Livesey
Neighbourhood Renewal Area was attempted by Southwark PCT Public Health. It was created in
association with the PCT's Locality Director and Southwark Committee's Area Renewal Officer.
A value profile of well-being what's more, access to administrations for the group was finished
what's more, displayed to the Neighbourhood Management Group what more, the Health and
Worklessness subgroup of Southwark Partnership LSP. To date, the value profile has been
utilized by the Neighbourhood Management Group for need setting. It has educated the
improvement of a Neighbourhood Health Advancement Team, and has been instrumental in the
choice to make the soundness of voyagers a point of convergence. The subsequent stages
incorporate refreshing the value profile as more data winds up accessible, and growing further
suggestions what's more, educating the anticipating activity process.
Illustration 2: Borough of Poole, Young
Individuals' HEA The Borough of Poole embraced a HEA for powerless youngsters and
youngsters to recognize needs and educate speculation decisions for the Children's Fund, the
Local Deterrent Strategy, Every Child Matters and the Children's Act. Organizations working
with kids and youngsters in Poole were associated with the HEA (Health Equity Audit, 2018).
Jan Sayers, Poole Local Government, states: territories where kids and youthful individuals have
the best needs were distinguished obviously from the HEA of both statistic data and execution
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

pointers.' accordingly, cross-organization targets have been concurred and advance is being made
towards sharing spending plans to complete work.
Case 3: Huddersfield Central, South Huddersfield and South West Yorkshire
Psychological well-being Trust – Mental HEA
A HEA was attempted crosswise over both Huddersfield PCTs for grown-ups and more
established individuals encountering mental sick well being. The measurements of imbalance
against which benefit arrangement was examined included age, sexual orientation, ethnicity and
geology. The administrations against which these measurements of imbalance were examined
included outpatients, post-natal sadness, confirmations, depression, GP endorsing rates and
suicides. Be that as it may, not all measurements of disparity were accounted for because of
varieties in information gathering between administrations (Making the case: health equity audit,
2018). The HEA meant to give information in an easy to understand organization to help
officials and specialist co-ops in the territories where value might be an issue, to help illuminate
choices with regard to asset appropriation in connection to needs
CONCLUSION
At the times when we are to apply various tools of health inequalities through using tools
which public health care practitioner could be using. The most important one could be that of
Health Equity audit tool which is majorly used in National Healthcare service of UK.
towards sharing spending plans to complete work.
Case 3: Huddersfield Central, South Huddersfield and South West Yorkshire
Psychological well-being Trust – Mental HEA
A HEA was attempted crosswise over both Huddersfield PCTs for grown-ups and more
established individuals encountering mental sick well being. The measurements of imbalance
against which benefit arrangement was examined included age, sexual orientation, ethnicity and
geology. The administrations against which these measurements of imbalance were examined
included outpatients, post-natal sadness, confirmations, depression, GP endorsing rates and
suicides. Be that as it may, not all measurements of disparity were accounted for because of
varieties in information gathering between administrations (Making the case: health equity audit,
2018). The HEA meant to give information in an easy to understand organization to help
officials and specialist co-ops in the territories where value might be an issue, to help illuminate
choices with regard to asset appropriation in connection to needs
CONCLUSION
At the times when we are to apply various tools of health inequalities through using tools
which public health care practitioner could be using. The most important one could be that of
Health Equity audit tool which is majorly used in National Healthcare service of UK.
REFERENCES
Books and Journals:
Brownson, R. C., Fielding, J. E., & Green, L. W. (2018). Building capacity for evidence-based
public health: reconciling the pulls of practice and the push of research. Annual review of
public health. (0).
de Wit, L., & Meijering, L. (2018). Community-based initiatives improving critical health
literacy: a systematic review and meta-synthesis of qualitative evidence. BMC public
health. 18(1). 40.
Green, J., & Thorogood, N. (2018). Qualitative methods for health research. Sage.
LaForge, K., & Clark, K. D. (2018). How 6 Organizations Developed Tools and Processes for
Social Determinants of Health Screening in Primary Care: An Overview. The Journal of
ambulatory care management. 41(1). 2.
Matwiejczyk, L., & Coveney, J. (2018). Characteristics of Effective Interventions Promoting
Healthy Eating for Pre-Schoolers in Childcare Settings: An Umbrella
Review. Nutrients. 10(3). 293.
McDonnell, L. A., & Pipe, A. L. (2018). Women's heart health: knowledge, beliefs, and
practices of Canadian physicians. Journal of women's health, 27(1). 72-82.
Wyatt, D., Cook, J., & McKevitt, C. (2018). Perceptions of the uses of routine general practice
data beyond individual care in England: a qualitative study. BMJ open. 8(1). e019378.
Online:
Health Equity Audit. 2018. [Online]. Accessed Through:
<http://www.health-inequalities.eu/tools/health-equity-audit/>.
Making the case: health equity audit. 2018. [Online]. Accessed Through:
<http://192.168.1.18/projectfiles/internal_cust_document/HealthEquityAuditMakingtheCas
e2_1521261841.pdf>.
NHS Health Checks in Nottingham City. 2018. [Online]. Accessed Through:
<file:///home/user/Downloads/Case%20study%20Health%20Equity%20Audit
%20NottinghamHC.pdf>.
Books and Journals:
Brownson, R. C., Fielding, J. E., & Green, L. W. (2018). Building capacity for evidence-based
public health: reconciling the pulls of practice and the push of research. Annual review of
public health. (0).
de Wit, L., & Meijering, L. (2018). Community-based initiatives improving critical health
literacy: a systematic review and meta-synthesis of qualitative evidence. BMC public
health. 18(1). 40.
Green, J., & Thorogood, N. (2018). Qualitative methods for health research. Sage.
LaForge, K., & Clark, K. D. (2018). How 6 Organizations Developed Tools and Processes for
Social Determinants of Health Screening in Primary Care: An Overview. The Journal of
ambulatory care management. 41(1). 2.
Matwiejczyk, L., & Coveney, J. (2018). Characteristics of Effective Interventions Promoting
Healthy Eating for Pre-Schoolers in Childcare Settings: An Umbrella
Review. Nutrients. 10(3). 293.
McDonnell, L. A., & Pipe, A. L. (2018). Women's heart health: knowledge, beliefs, and
practices of Canadian physicians. Journal of women's health, 27(1). 72-82.
Wyatt, D., Cook, J., & McKevitt, C. (2018). Perceptions of the uses of routine general practice
data beyond individual care in England: a qualitative study. BMJ open. 8(1). e019378.
Online:
Health Equity Audit. 2018. [Online]. Accessed Through:
<http://www.health-inequalities.eu/tools/health-equity-audit/>.
Making the case: health equity audit. 2018. [Online]. Accessed Through:
<http://192.168.1.18/projectfiles/internal_cust_document/HealthEquityAuditMakingtheCas
e2_1521261841.pdf>.
NHS Health Checks in Nottingham City. 2018. [Online]. Accessed Through:
<file:///home/user/Downloads/Case%20study%20Health%20Equity%20Audit
%20NottinghamHC.pdf>.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.