Health Information Management Virtual Tour Worksheet - University Name
VerifiedAdded on 2022/08/16
|6
|903
|9
Homework Assignment
AI Summary
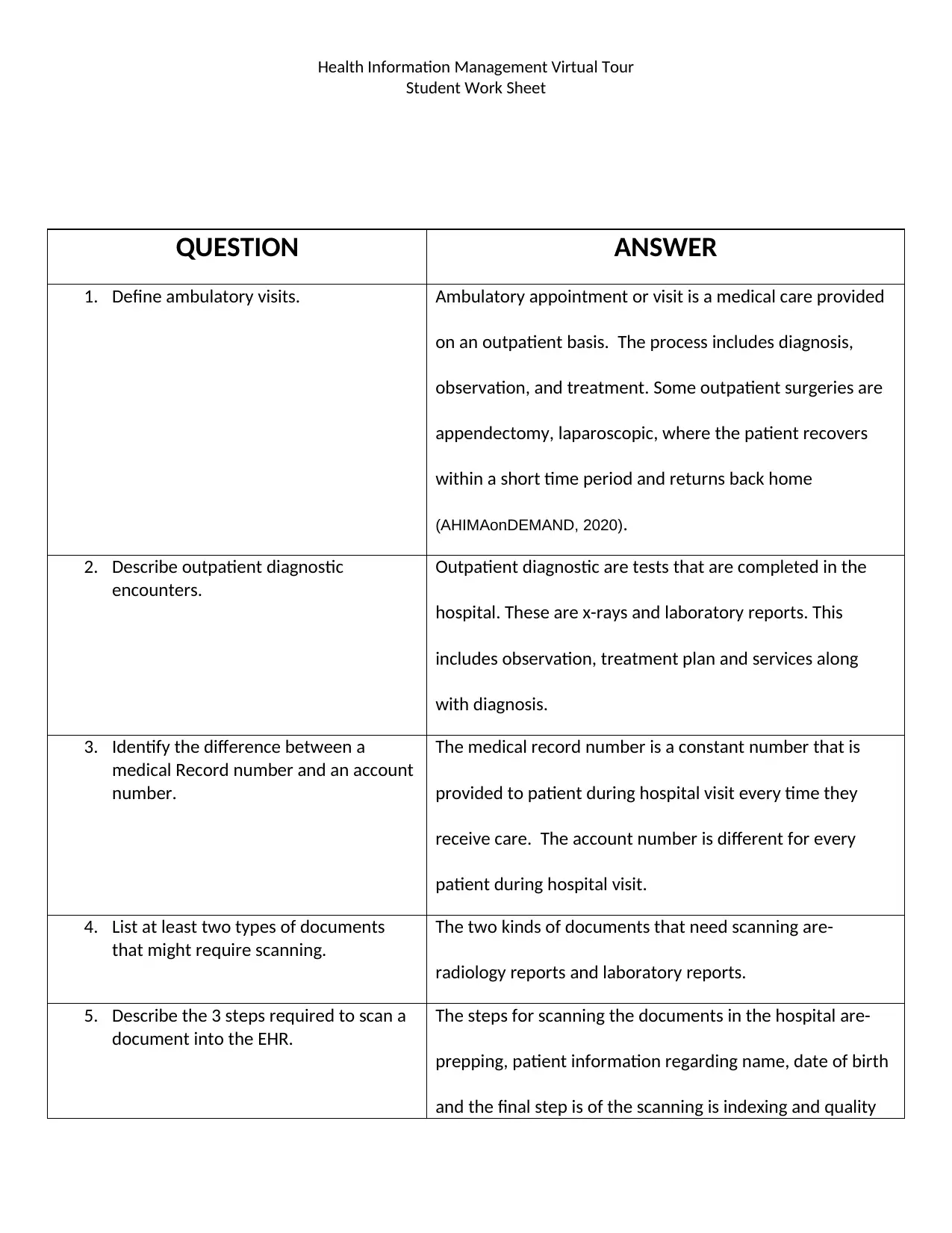
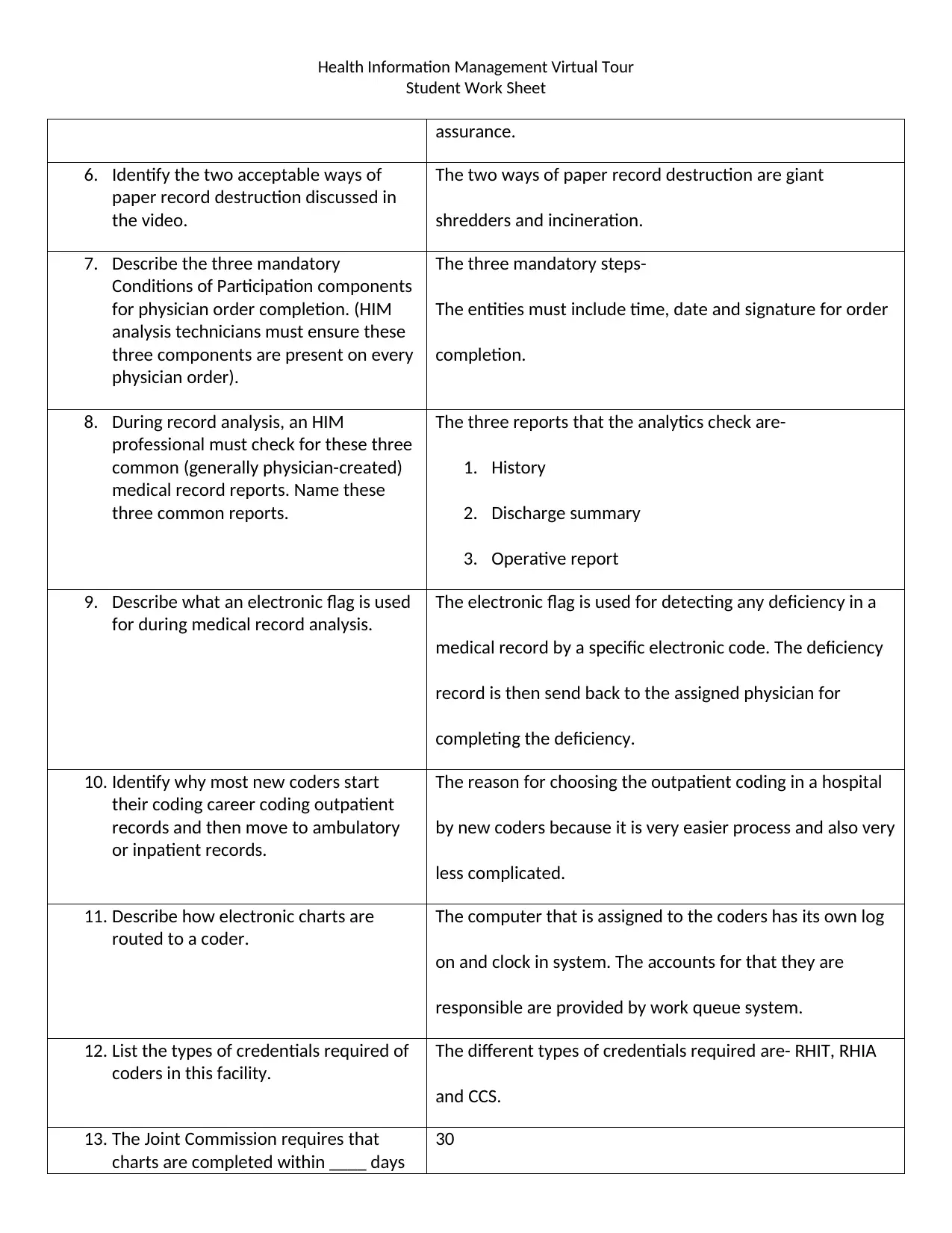
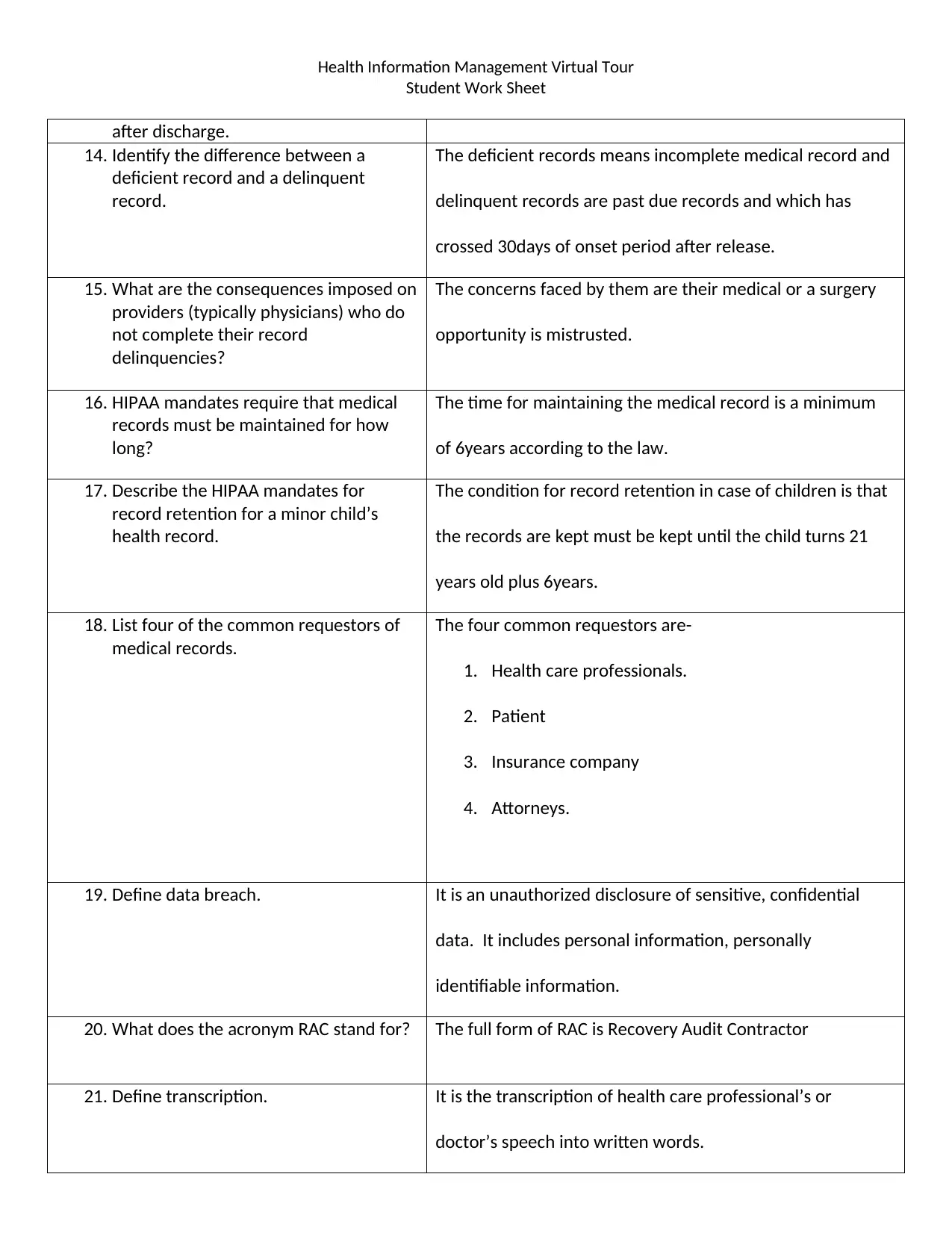
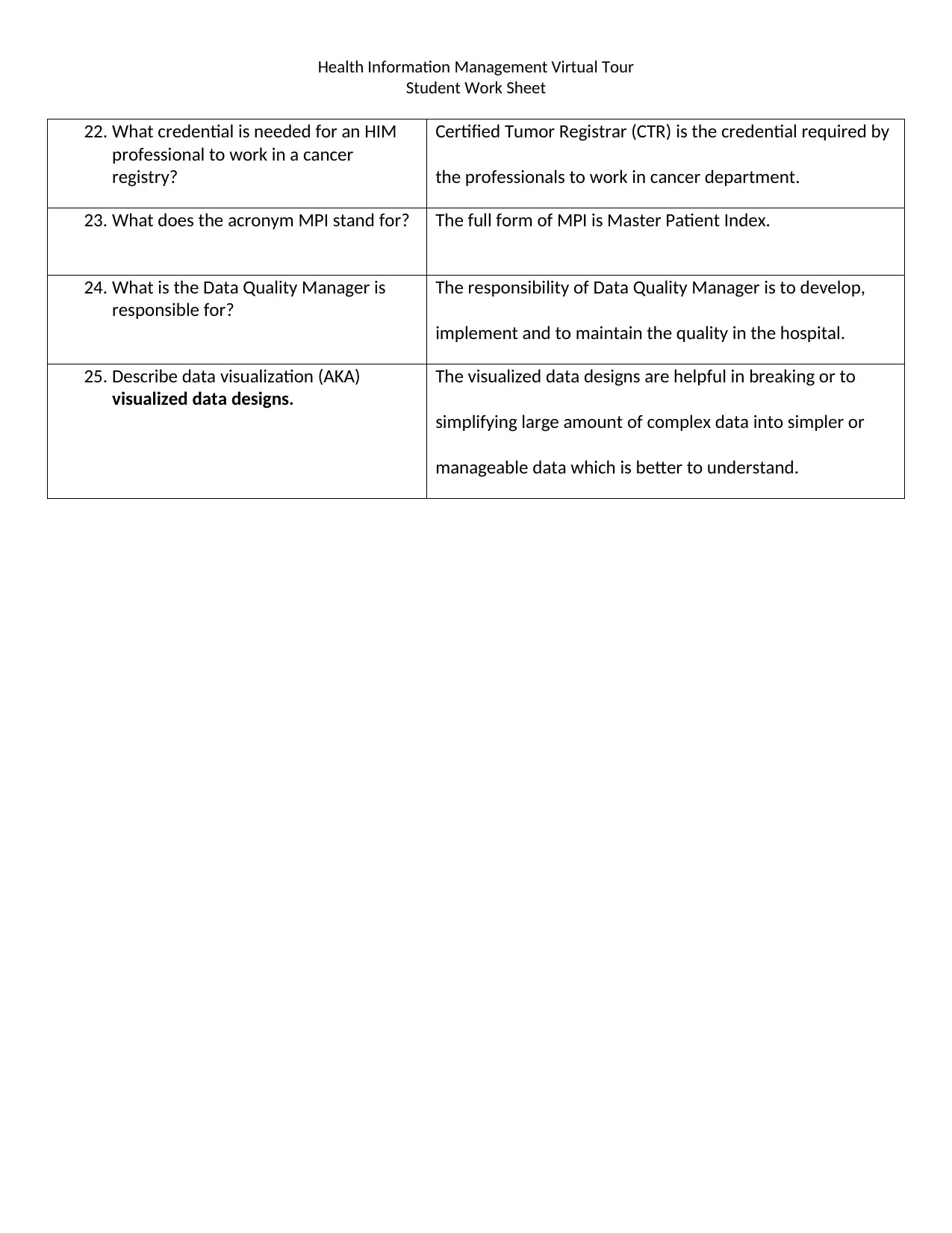
This homework assignment presents a completed worksheet based on a virtual tour of a Health Information Management (HIM) department at a hospital. The student answers questions regarding ambulatory visits, outpatient diagnostics, medical record numbers, document scanning, electronic health records (EHR), paper record destruction, physician order completion, common medical record reports, electronic flags, coding, and credentialing. The assignment also covers topics such as delinquent records, HIPAA mandates, data breaches, transcription, cancer registry requirements, the Master Patient Index (MPI), data quality management, and data visualization. The answers are derived from a video tour of the Sinclair Memorial Hospital HIM department, providing a practical understanding of HIM processes and terminology.

1 out of 6



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.