DSRS1206 Report: Health Issues, Disability, Down Syndrome, Obesity
VerifiedAdded on 2023/01/16
|12
|3285
|1
Report
AI Summary
This report provides a comprehensive overview of Down syndrome, a genetic disorder, and its association with obesity. It details the characteristics, causes, and the impact of Down syndrome, including developmental delays and intellectual disabilities. The report further explores obesity as a complex health issue, particularly prevalent in individuals with Down syndrome, and its contributing factors such as genetics, behavior, and lifestyle. It delves into the physical and psychological consequences of obesity, highlighting related health problems like diabetes and heart disease. The report then outlines various management approaches, including lifestyle interventions focused on increased physical activity and dietary changes. It also mentions the role of healthcare professionals, such as doctors, dietitians, and exercise physiologists, in providing counseling and support. The report emphasizes the importance of creating supportive environments and providing training to promote physical activity and healthy eating habits for individuals with Down syndrome and obesity.
Health issues and disability
Student’s Name: Stevie-Lee Semgreen
Student’s ID: 2221031
Subject: DSRS1206- Health issues and disability
Word Count: 2082
Student’s Name: Stevie-Lee Semgreen
Student’s ID: 2221031
Subject: DSRS1206- Health issues and disability
Word Count: 2082
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
Table of Contents
Introduction......................................................................................................................................2
Part A...............................................................................................................................................2
Description of Down syndrome that causes disability.................................................................2
Part B...............................................................................................................................................4
Description of obesity..................................................................................................................4
Part C...............................................................................................................................................6
Management approaches..............................................................................................................6
Conclusion.......................................................................................................................................9
References......................................................................................................................................10
Table of Contents
Introduction......................................................................................................................................2
Part A...............................................................................................................................................2
Description of Down syndrome that causes disability.................................................................2
Part B...............................................................................................................................................4
Description of obesity..................................................................................................................4
Part C...............................................................................................................................................6
Management approaches..............................................................................................................6
Conclusion.......................................................................................................................................9
References......................................................................................................................................10
2
Introduction
The primary purpose of the paper is to explain a condition or syndrome that causes disability and
health care issue. It will discuss Down syndrome that could also lead to obesity-related problems
among individuals. It will also discuss the features and causes of Down syndrome and obesity.
Based on the particular health care issue which is common in the population it will provide
relevant information about the management implications. Such management approaches will
help manage with health issue faced by the individuals within the society. It will also discuss the
professionals those who are involved in the management approach.
Part A
Description of Down syndrome that causes disability
Down syndrome is determined to be a genetic disorder occurring when abnormal cell division
results in a partial or full additional chromosome 21 (Skotko, Levine, Macklin & Goldstein,
2016). It is regarded as the additional chromosomal material that causes developmental delays
and intellectual disabilities to varying severity (Jeffery, Cunningham & Whiteside, 2018). It is
considered to be the most common genetic chromosomal disorder that causes learning
disabilities among children (de Graaf, Levine, Goldstein & Skotko, 2019). Usually, it causes
other medical abnormalities like gastrointestinal and heart disorders (Jansen, Desbrow & Ball,
2015).
Characteristics
Developmental as well as intellectual problems may be severe, moderate or mild for each person
who has Down syndrome. Some of the individuals are healthy whereas; others deal with
significant health problems like serious heart defects (Turner, Harris & Mazza, 2015). Adults and
children with Down syndrome share common facial features. The common physical
characteristics of Down syndrome includes short height, poor muscle tone, short neck, small
head, flattened face, excessive flexibility, relatively small feet, hands, and fingers, small or
unusual shaped ears, short, huge hands with a single crease in the palm, upward slanting eyelids
and protruding tongue. Individuals with Down syndrome have more in common with their
families as compared to another individual with Down syndrome. Similar to the rest of the
population they will inherit the characteristics of their families
Introduction
The primary purpose of the paper is to explain a condition or syndrome that causes disability and
health care issue. It will discuss Down syndrome that could also lead to obesity-related problems
among individuals. It will also discuss the features and causes of Down syndrome and obesity.
Based on the particular health care issue which is common in the population it will provide
relevant information about the management implications. Such management approaches will
help manage with health issue faced by the individuals within the society. It will also discuss the
professionals those who are involved in the management approach.
Part A
Description of Down syndrome that causes disability
Down syndrome is determined to be a genetic disorder occurring when abnormal cell division
results in a partial or full additional chromosome 21 (Skotko, Levine, Macklin & Goldstein,
2016). It is regarded as the additional chromosomal material that causes developmental delays
and intellectual disabilities to varying severity (Jeffery, Cunningham & Whiteside, 2018). It is
considered to be the most common genetic chromosomal disorder that causes learning
disabilities among children (de Graaf, Levine, Goldstein & Skotko, 2019). Usually, it causes
other medical abnormalities like gastrointestinal and heart disorders (Jansen, Desbrow & Ball,
2015).
Characteristics
Developmental as well as intellectual problems may be severe, moderate or mild for each person
who has Down syndrome. Some of the individuals are healthy whereas; others deal with
significant health problems like serious heart defects (Turner, Harris & Mazza, 2015). Adults and
children with Down syndrome share common facial features. The common physical
characteristics of Down syndrome includes short height, poor muscle tone, short neck, small
head, flattened face, excessive flexibility, relatively small feet, hands, and fingers, small or
unusual shaped ears, short, huge hands with a single crease in the palm, upward slanting eyelids
and protruding tongue. Individuals with Down syndrome have more in common with their
families as compared to another individual with Down syndrome. Similar to the rest of the
population they will inherit the characteristics of their families
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
An infant with Down syndrome remains shorter and grows slowly as compared to other children
of the same age (Sabin & Kiess, 2015). Majority of the children with Down syndrome possess
minor to reasonable mental impairment where long and short-term memory is exaggerated, and
language is delayed (Skotko et al., 2016). A child with Down syndrome possesses some degree
of learning disability that widely differs among different individuals (Heymsfield & Wadden,
2017).
Delayed development
A child with Down syndrome may be slower to acquire skills such as, talking, walking, standing
and sitting due to poor muscle tone. However, despite such delays children with Down syndrome
can participate in the activities related to physical exercise like other children. Eventually, they
are likely to develop these skills, but it takes more time. A few of the children with Down
syndrome may possess more complex requirements, for instance, they may have attention deficit
hyperactivity disorder or be on the autism spectrum.
Causes
Down syndrome occurs due to other mechanisms such as ring chromosome, isochromosome, and
Robertsonian translocation (Laws, Brown & Main, 2016). Such mechanisms may affect an
individual’s personal growth and cognitive ability that causes issues of moderate development
(Ying et al., 2019). It occurs when the body of an individual absorbs more calories than it burns.
Down syndrome causes due to any one of the three genetic variations are as follows:
Trisomy 21
Down syndrome is caused due to trisomy 21, about 95% of the time, where the individual
possesses three copies of chromosome 21 rather than two copies in every cell (Furukawa et al.,
2017). This is caused due to the abnormal cell division at the time of growth of the egg cell or
sperm cell.
Translocation Down syndrome
Down syndrome also causes when a part of chromosome 21 becomes translocated into another
chromosome after or before conception. These children possess two copies of chromosome 21,
An infant with Down syndrome remains shorter and grows slowly as compared to other children
of the same age (Sabin & Kiess, 2015). Majority of the children with Down syndrome possess
minor to reasonable mental impairment where long and short-term memory is exaggerated, and
language is delayed (Skotko et al., 2016). A child with Down syndrome possesses some degree
of learning disability that widely differs among different individuals (Heymsfield & Wadden,
2017).
Delayed development
A child with Down syndrome may be slower to acquire skills such as, talking, walking, standing
and sitting due to poor muscle tone. However, despite such delays children with Down syndrome
can participate in the activities related to physical exercise like other children. Eventually, they
are likely to develop these skills, but it takes more time. A few of the children with Down
syndrome may possess more complex requirements, for instance, they may have attention deficit
hyperactivity disorder or be on the autism spectrum.
Causes
Down syndrome occurs due to other mechanisms such as ring chromosome, isochromosome, and
Robertsonian translocation (Laws, Brown & Main, 2016). Such mechanisms may affect an
individual’s personal growth and cognitive ability that causes issues of moderate development
(Ying et al., 2019). It occurs when the body of an individual absorbs more calories than it burns.
Down syndrome causes due to any one of the three genetic variations are as follows:
Trisomy 21
Down syndrome is caused due to trisomy 21, about 95% of the time, where the individual
possesses three copies of chromosome 21 rather than two copies in every cell (Furukawa et al.,
2017). This is caused due to the abnormal cell division at the time of growth of the egg cell or
sperm cell.
Translocation Down syndrome
Down syndrome also causes when a part of chromosome 21 becomes translocated into another
chromosome after or before conception. These children possess two copies of chromosome 21,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
but they also contain supplementary genetic material from chromosome 21 translocated to
another chromosome (Leiter et al., 2015).
but they also contain supplementary genetic material from chromosome 21 translocated to
another chromosome (Leiter et al., 2015).
5
Mosaic Down syndrome
In this form of Down syndrome, an individual possesses few cells along with an additional copy
of chromosome 21. This mosaic of abnormal or normal cells is produced due to the division of
abnormal cell after conception (de Graaf et al., 2019). The cells having normal chromosomes
could restrain the effect of the trisomy 21 cells and change the effect on the mental and physical
development of a patient. There poses huge variability in phenotype in individuals with Down
syndrome.
Part B
Description of obesity
Obesity is determined to be a complex health issue that is common in this population of women
who possess huge amount of body fat of around 32%. It occurs when there is an influence of
hormonal, behavioral and genetic and social factors on body weight. It is a mixture of donating
factors and leads to individual features like, genetics as well as behavior. The diagnosis of Down
syndrome like additional genetic material creates the chances of being obese. It is a medical
condition with the accumulation of extreme body fat that results in serious health-related
consequences. Different lifestyle factors may involve medication use, inactivity, physical activity
and dietary patterns along with other exposures. However, additional contributing factors within
the community involve the food promotion and marketing, education and skills as well as
physical and food activity environment (Furukawa et al., 2017). Obesity is considered to be a
serious health concern as it is correlated with poorer outcomes of mental health, leading causes
of death and reduced quality of life. Obesity leads to an increased risk of health problems and
diseases like high blood pressure, diabetes and heart disease. Obesity also results in
psychological problems like the reduced quality of life, difficulty in finding employment,
discrimination and low self-esteem. On the other hand, childhood obesity results into higher
chances of disability in adulthood, premature death along with a greater chance of obesity
(Jansen et al., 2015). The other factors that are related to obesity are hormones, ethnicity and
childhood weight that influences the development of obesity.
Obesity-related health problems may have a major economic influence on the health care system
across the world (Turner et al., 2015). One of the common feature of obesity is appearances that
possess velvety and dark skin in other areas like cheek, chin and forehead and around the neck,
Mosaic Down syndrome
In this form of Down syndrome, an individual possesses few cells along with an additional copy
of chromosome 21. This mosaic of abnormal or normal cells is produced due to the division of
abnormal cell after conception (de Graaf et al., 2019). The cells having normal chromosomes
could restrain the effect of the trisomy 21 cells and change the effect on the mental and physical
development of a patient. There poses huge variability in phenotype in individuals with Down
syndrome.
Part B
Description of obesity
Obesity is determined to be a complex health issue that is common in this population of women
who possess huge amount of body fat of around 32%. It occurs when there is an influence of
hormonal, behavioral and genetic and social factors on body weight. It is a mixture of donating
factors and leads to individual features like, genetics as well as behavior. The diagnosis of Down
syndrome like additional genetic material creates the chances of being obese. It is a medical
condition with the accumulation of extreme body fat that results in serious health-related
consequences. Different lifestyle factors may involve medication use, inactivity, physical activity
and dietary patterns along with other exposures. However, additional contributing factors within
the community involve the food promotion and marketing, education and skills as well as
physical and food activity environment (Furukawa et al., 2017). Obesity is considered to be a
serious health concern as it is correlated with poorer outcomes of mental health, leading causes
of death and reduced quality of life. Obesity leads to an increased risk of health problems and
diseases like high blood pressure, diabetes and heart disease. Obesity also results in
psychological problems like the reduced quality of life, difficulty in finding employment,
discrimination and low self-esteem. On the other hand, childhood obesity results into higher
chances of disability in adulthood, premature death along with a greater chance of obesity
(Jansen et al., 2015). The other factors that are related to obesity are hormones, ethnicity and
childhood weight that influences the development of obesity.
Obesity-related health problems may have a major economic influence on the health care system
across the world (Turner et al., 2015). One of the common feature of obesity is appearances that
possess velvety and dark skin in other areas like cheek, chin and forehead and around the neck,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
stretch marks on abdomen and hips and disposition of fatty tissues. Another feature is
Orthopedic that leads to dislocated hip, knock-knees and flat fleet. Whereas Gastroenterological
feature possess Gastroesophageal reflux and constipation. One of the other feature is Pulmonary
Sleep that results into apnea and shortness of breath when physically active. While Psychological
Eating disorder is another feature that leads to poor self-esteem, abuse and teasing.
Individuals who are obese may possess the characteristics of medical conditions such as, joint
pain, breathing issues, increased cholesterol levels, and blood pressure are common within the
population (Sabin et al., 2015).
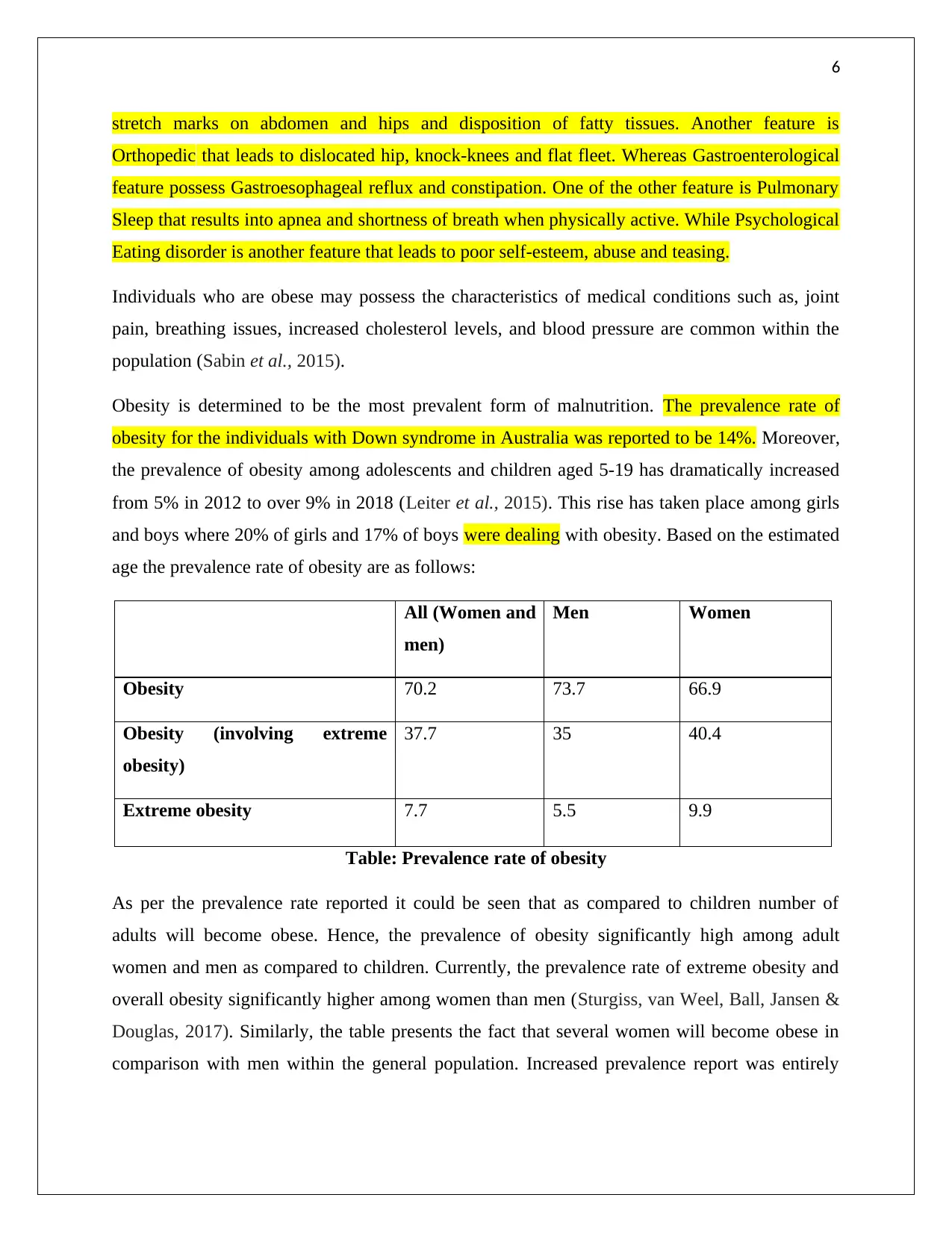
Obesity is determined to be the most prevalent form of malnutrition. The prevalence rate of
obesity for the individuals with Down syndrome in Australia was reported to be 14%. Moreover,
the prevalence of obesity among adolescents and children aged 5-19 has dramatically increased
from 5% in 2012 to over 9% in 2018 (Leiter et al., 2015). This rise has taken place among girls
and boys where 20% of girls and 17% of boys were dealing with obesity. Based on the estimated
age the prevalence rate of obesity are as follows:
All (Women and
men)
Men Women
Obesity 70.2 73.7 66.9
Obesity (involving extreme
obesity)
37.7 35 40.4
Extreme obesity 7.7 5.5 9.9
Table: Prevalence rate of obesity
As per the prevalence rate reported it could be seen that as compared to children number of
adults will become obese. Hence, the prevalence of obesity significantly high among adult
women and men as compared to children. Currently, the prevalence rate of extreme obesity and
overall obesity significantly higher among women than men (Sturgiss, van Weel, Ball, Jansen &
Douglas, 2017). Similarly, the table presents the fact that several women will become obese in
comparison with men within the general population. Increased prevalence report was entirely
stretch marks on abdomen and hips and disposition of fatty tissues. Another feature is
Orthopedic that leads to dislocated hip, knock-knees and flat fleet. Whereas Gastroenterological
feature possess Gastroesophageal reflux and constipation. One of the other feature is Pulmonary
Sleep that results into apnea and shortness of breath when physically active. While Psychological
Eating disorder is another feature that leads to poor self-esteem, abuse and teasing.
Individuals who are obese may possess the characteristics of medical conditions such as, joint
pain, breathing issues, increased cholesterol levels, and blood pressure are common within the
population (Sabin et al., 2015).
Obesity is determined to be the most prevalent form of malnutrition. The prevalence rate of
obesity for the individuals with Down syndrome in Australia was reported to be 14%. Moreover,
the prevalence of obesity among adolescents and children aged 5-19 has dramatically increased
from 5% in 2012 to over 9% in 2018 (Leiter et al., 2015). This rise has taken place among girls
and boys where 20% of girls and 17% of boys were dealing with obesity. Based on the estimated
age the prevalence rate of obesity are as follows:
All (Women and
men)
Men Women
Obesity 70.2 73.7 66.9
Obesity (involving extreme
obesity)
37.7 35 40.4
Extreme obesity 7.7 5.5 9.9
Table: Prevalence rate of obesity
As per the prevalence rate reported it could be seen that as compared to children number of
adults will become obese. Hence, the prevalence of obesity significantly high among adult
women and men as compared to children. Currently, the prevalence rate of extreme obesity and
overall obesity significantly higher among women than men (Sturgiss, van Weel, Ball, Jansen &
Douglas, 2017). Similarly, the table presents the fact that several women will become obese in
comparison with men within the general population. Increased prevalence report was entirely
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
based on different growth standards and cut-off points. It is also based on socio-economic
factors, eating habits as well as diet patterns of men, women, children, and adolescents.
Part C
Management approaches
The lifestyle management approach is determined to be the hierarchical approach that helps in
managing obesity. This includes increased physical activity and diet. Moreover, an individual
may access online dynamic models that predict how physical activity and diet impact on weight
loss over time. This model may be beneficial in setting a target energy intake for a person related
to their need for ongoing weight maintenance and loss. Such models have recognized multiple
lifestyle factors related to the maintenance of weight loss (Heymsfield et al., 2017). These
involve, eating a constant eating pattern throughout the year, self-monitoring weight, consuming
breakfast regularly, low-fat diet, adhering to a low-calorie and involving in increased levels of
physical activity. As a result, lifestyle changes are considered to be a major treatment and is
significant for the long-lasting maintenance of weight loss. However, lifestyle management
approach serves a structured treatment procedure which is designed to facilitate weight
maintenance. The lifestyle intervention also provides various programs such as the Diabetes
Prevention Program helps in reducing calories. The dual diagnosis of Down syndrome impacts
on the development of brain.
The changes are measured with the help of body mass index where the prevalence of obesity is
measured. The body mass index is determined to be a measure related to weight and height that
applies to adult women and men. It needs to enter the weight by using metric and standard
measures and then select compute BMI. Whereas, the body fat percentage can be measured by
using skinfold calipers, body circumstances measurement and hydrostatic weighing.
The individuals who are commonly involved in the lifestyle management approach are trained
interventionists who practices intervention, health-care professionals such as nurses, doctors,
exercise physiologist, behavioral psychologist along with a registered dietician. All these
professional are highly involved by counseling patients regarding long-term weight management
strategies, suitable physical activities, and nutrition. On the other hand, these professionals also
provide treatment through smartphone, internet, and telephone to a larger population to mitigate
the problem of obesity (Bray, Frühbeck, Ryan & Wilding, 2016). Moreover, various programs
based on different growth standards and cut-off points. It is also based on socio-economic
factors, eating habits as well as diet patterns of men, women, children, and adolescents.
Part C
Management approaches
The lifestyle management approach is determined to be the hierarchical approach that helps in
managing obesity. This includes increased physical activity and diet. Moreover, an individual
may access online dynamic models that predict how physical activity and diet impact on weight
loss over time. This model may be beneficial in setting a target energy intake for a person related
to their need for ongoing weight maintenance and loss. Such models have recognized multiple
lifestyle factors related to the maintenance of weight loss (Heymsfield et al., 2017). These
involve, eating a constant eating pattern throughout the year, self-monitoring weight, consuming
breakfast regularly, low-fat diet, adhering to a low-calorie and involving in increased levels of
physical activity. As a result, lifestyle changes are considered to be a major treatment and is
significant for the long-lasting maintenance of weight loss. However, lifestyle management
approach serves a structured treatment procedure which is designed to facilitate weight
maintenance. The lifestyle intervention also provides various programs such as the Diabetes
Prevention Program helps in reducing calories. The dual diagnosis of Down syndrome impacts
on the development of brain.
The changes are measured with the help of body mass index where the prevalence of obesity is
measured. The body mass index is determined to be a measure related to weight and height that
applies to adult women and men. It needs to enter the weight by using metric and standard
measures and then select compute BMI. Whereas, the body fat percentage can be measured by
using skinfold calipers, body circumstances measurement and hydrostatic weighing.
The individuals who are commonly involved in the lifestyle management approach are trained
interventionists who practices intervention, health-care professionals such as nurses, doctors,
exercise physiologist, behavioral psychologist along with a registered dietician. All these
professional are highly involved by counseling patients regarding long-term weight management
strategies, suitable physical activities, and nutrition. On the other hand, these professionals also
provide treatment through smartphone, internet, and telephone to a larger population to mitigate
the problem of obesity (Bray, Frühbeck, Ryan & Wilding, 2016). Moreover, various programs
8
are also involved for the patients dealing with obesity to help them to reduce their weight. For
example, the Diabetes Prevention Program also provides counseling to inform the patients
regarding low-fat diet (1100-1900 kcal/day) as well as physical activity. The diagnosis of Down
syndrome will develop mental and physical skills and will increase the chances of leading
meaningful lives and gaining abilities to do work.
To increase the participation of obese people in the home, community, educational or vocational
setting, it is suggested to enhance active living and healthy eating in various settings. Some of
the support that must be provided to the patients dealing with obesity are environment that
provides social and physical atmosphere that enables and encourages an enjoyable and safe
physical activity. Whereas, Health services is important to assess and counsel about physical
activity to young people. The health services must advocate people regarding physical activity
programs and instructions. While, Personnel training is also essential to provide recreation,
coaching, health-care and training for education and community personnel that helps in gaining
skills and knowledge necessary to promote physical activity among people dealing with obesity
and Down syndrome (Saltiel & Olefsky, 2017).
Moreover, extracurricular activities is another support that helps in creating programs based on
extracurricular physical activity that meets the interests and needs of the obsessed person.
Furthermore, Parental engagement is the support that involves guardians and parents in physical
activity instructions. They must also be involved in the community and extracurricular physical
activity programs that help in maintaining weight (Jain & Singh, 2015). Meanwhile, Health
education is also important to adopt physical education instruction and curricula that enhance the
enjoyable participation of obese people in the home, education, community or vocational
settings. While, Community programs is also significant to facilitate a huge range of relevant
recreation programs that helps in attracting people who deal with obesity and Down syndrome
(Sweeting & Caterson, 2017). However, based on this support the diagnosis of Down syndrome
will create a positive impact by overcoming the challenges and difficulties faced by the
individuals.
Conclusion
The paper demonstrated an understanding of Down syndrome that leads to disability. It discussed
the causes and characteristics of Down syndrome that affects an individual. Moreover, it can be
are also involved for the patients dealing with obesity to help them to reduce their weight. For
example, the Diabetes Prevention Program also provides counseling to inform the patients
regarding low-fat diet (1100-1900 kcal/day) as well as physical activity. The diagnosis of Down
syndrome will develop mental and physical skills and will increase the chances of leading
meaningful lives and gaining abilities to do work.
To increase the participation of obese people in the home, community, educational or vocational
setting, it is suggested to enhance active living and healthy eating in various settings. Some of
the support that must be provided to the patients dealing with obesity are environment that
provides social and physical atmosphere that enables and encourages an enjoyable and safe
physical activity. Whereas, Health services is important to assess and counsel about physical
activity to young people. The health services must advocate people regarding physical activity
programs and instructions. While, Personnel training is also essential to provide recreation,
coaching, health-care and training for education and community personnel that helps in gaining
skills and knowledge necessary to promote physical activity among people dealing with obesity
and Down syndrome (Saltiel & Olefsky, 2017).
Moreover, extracurricular activities is another support that helps in creating programs based on
extracurricular physical activity that meets the interests and needs of the obsessed person.
Furthermore, Parental engagement is the support that involves guardians and parents in physical
activity instructions. They must also be involved in the community and extracurricular physical
activity programs that help in maintaining weight (Jain & Singh, 2015). Meanwhile, Health
education is also important to adopt physical education instruction and curricula that enhance the
enjoyable participation of obese people in the home, education, community or vocational
settings. While, Community programs is also significant to facilitate a huge range of relevant
recreation programs that helps in attracting people who deal with obesity and Down syndrome
(Sweeting & Caterson, 2017). However, based on this support the diagnosis of Down syndrome
will create a positive impact by overcoming the challenges and difficulties faced by the
individuals.
Conclusion
The paper demonstrated an understanding of Down syndrome that leads to disability. It discussed
the causes and characteristics of Down syndrome that affects an individual. Moreover, it can be
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

9
seen that Down syndrome affects the language and communication skills of an individual. It is
recommended that physical therapy must be adopted that involves exercises and activities that
improves, balance and posture, increases muscle strength and build motor skills. Whereas,
speech language therapy improves language and communication skills effectively. It has been
observed that as compared to boys a greater number of girls in Australia are dealing with
obesity-related issues. Therefore, the paper discussed the lifestyle management approach that
helps reduce and maintain weight.
seen that Down syndrome affects the language and communication skills of an individual. It is
recommended that physical therapy must be adopted that involves exercises and activities that
improves, balance and posture, increases muscle strength and build motor skills. Whereas,
speech language therapy improves language and communication skills effectively. It has been
observed that as compared to boys a greater number of girls in Australia are dealing with
obesity-related issues. Therefore, the paper discussed the lifestyle management approach that
helps reduce and maintain weight.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
References
Bray, G. A., Frühbeck, G., Ryan, D. H., & Wilding, J. P. (2016). Management of obesity. The
Lancet, 387(10031), 1947-1956.
de Graaf, G., Levine, S. P., Goldstein, R., & Skotko, B. G. (2019). Parents' perceptions of
functional abilities in people with Down syndrome. American Journal of Medical
Genetics Part A, 179(2), 161-176.
Furukawa, S., Fujita, T., Shimabukuro, M., Iwaki, M., Yamada, Y., Nakajima, Y., ... &
Shimomura, I. (2017). Increased oxidative stress in obesity and its impact on metabolic
syndrome. The Journal of clinical investigation, 114(12), 1752-1761.
Heymsfield, S. B., & Wadden, T. A. (2017). Mechanisms, pathophysiology, and management of
obesity. New England Journal of Medicine, 376(3), 254-266.
Jain, S., & Singh, S. N. (2015). Calorie restriction â an approach towards obesity management. J
Nutr Disord Ther, 1, 2161-0509.
Jansen, S., Desbrow, B., & Ball, L. (2015). Obesity management by general practitioners: the
unavoidable necessity. Australian Journal of Primary Health, 21(4), 366-368.
Jeffery, T., Cunningham, S., & Whiteside, S. P. (2018). Analyses of sustained vowels in down
syndrome (DS): a case study using spectrograms and perturbation data to investigate
voice quality in four adults with DS. Journal of Voice, 32(5), 644-e11.
Laws, G., Brown, H., & Main, E. (2016). Reading comprehension in children with Down
syndrome. Reading and writing, 29(1), 21-45.
Leiter, L. A., Astrup, A., Andrews, R. C., Cuevas, A., Horn, D. B., Kunešová, M., ... & Finer, N.
(2015). Identification of educational needs in the management of overweight and obesity:
results of an international survey of attitudes and practice. Clinical obesity, 5(5), 245-255.
Sabin, M. A., & Kiess, W. (2015). Childhood obesity: Current and novel approaches. Best
Practice & Research Clinical Endocrinology & Metabolism, 29(3), 327-338.
Saltiel, A. R., & Olefsky, J. M. (2017). Inflammatory mechanisms linking obesity and metabolic
disease. The Journal of clinical investigation, 127(1), 1-4.
References
Bray, G. A., Frühbeck, G., Ryan, D. H., & Wilding, J. P. (2016). Management of obesity. The
Lancet, 387(10031), 1947-1956.
de Graaf, G., Levine, S. P., Goldstein, R., & Skotko, B. G. (2019). Parents' perceptions of
functional abilities in people with Down syndrome. American Journal of Medical
Genetics Part A, 179(2), 161-176.
Furukawa, S., Fujita, T., Shimabukuro, M., Iwaki, M., Yamada, Y., Nakajima, Y., ... &
Shimomura, I. (2017). Increased oxidative stress in obesity and its impact on metabolic
syndrome. The Journal of clinical investigation, 114(12), 1752-1761.
Heymsfield, S. B., & Wadden, T. A. (2017). Mechanisms, pathophysiology, and management of
obesity. New England Journal of Medicine, 376(3), 254-266.
Jain, S., & Singh, S. N. (2015). Calorie restriction â an approach towards obesity management. J
Nutr Disord Ther, 1, 2161-0509.
Jansen, S., Desbrow, B., & Ball, L. (2015). Obesity management by general practitioners: the
unavoidable necessity. Australian Journal of Primary Health, 21(4), 366-368.
Jeffery, T., Cunningham, S., & Whiteside, S. P. (2018). Analyses of sustained vowels in down
syndrome (DS): a case study using spectrograms and perturbation data to investigate
voice quality in four adults with DS. Journal of Voice, 32(5), 644-e11.
Laws, G., Brown, H., & Main, E. (2016). Reading comprehension in children with Down
syndrome. Reading and writing, 29(1), 21-45.
Leiter, L. A., Astrup, A., Andrews, R. C., Cuevas, A., Horn, D. B., Kunešová, M., ... & Finer, N.
(2015). Identification of educational needs in the management of overweight and obesity:
results of an international survey of attitudes and practice. Clinical obesity, 5(5), 245-255.
Sabin, M. A., & Kiess, W. (2015). Childhood obesity: Current and novel approaches. Best
Practice & Research Clinical Endocrinology & Metabolism, 29(3), 327-338.
Saltiel, A. R., & Olefsky, J. M. (2017). Inflammatory mechanisms linking obesity and metabolic
disease. The Journal of clinical investigation, 127(1), 1-4.
11
Skotko, B. G., Levine, S. P., Macklin, E. A., & Goldstein, R. D. (2016). Family perspectives
about Down syndrome. American Journal of Medical Genetics Part A, 170(4), 930-941.
Sturgiss, E. A., van Weel, C., Ball, L., Jansen, S., & Douglas, K. (2017). Obesity management in
Australian primary care: where has the general practitioner gone?. Australian journal of
primary health, 22(6), 473-476.
Sweeting, A. N., & Caterson, I. D. (2017). Approaches to obesity management. Internal
medicine journal, 47(7), 734-739.
Turner, L. R., Harris, M. F., & Mazza, D. (2015). Obesity management in general practice: does
current practice match guideline recommendations?. Medical Journal of
Australia, 202(7), 370-372.
Ying, J., Sato, Y., Im, E., Berg, M., Bordi, M., Darji, S., ... & Cuervo, A. M. (2019). Lysosomal
dysfunction in Down syndrome is APP-dependent and mediated by APP-βCTF
(C99). Journal of Neuroscience, 0578-19.
Skotko, B. G., Levine, S. P., Macklin, E. A., & Goldstein, R. D. (2016). Family perspectives
about Down syndrome. American Journal of Medical Genetics Part A, 170(4), 930-941.
Sturgiss, E. A., van Weel, C., Ball, L., Jansen, S., & Douglas, K. (2017). Obesity management in
Australian primary care: where has the general practitioner gone?. Australian journal of
primary health, 22(6), 473-476.
Sweeting, A. N., & Caterson, I. D. (2017). Approaches to obesity management. Internal
medicine journal, 47(7), 734-739.
Turner, L. R., Harris, M. F., & Mazza, D. (2015). Obesity management in general practice: does
current practice match guideline recommendations?. Medical Journal of
Australia, 202(7), 370-372.
Ying, J., Sato, Y., Im, E., Berg, M., Bordi, M., Darji, S., ... & Cuervo, A. M. (2019). Lysosomal
dysfunction in Down syndrome is APP-dependent and mediated by APP-βCTF
(C99). Journal of Neuroscience, 0578-19.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.