Psychology Essay: Health Perspectives, Pain Theories & Management
VerifiedAdded on 2023/06/11
|10
|2236
|68
Essay
AI Summary
This essay provides a comprehensive overview of health concepts, contrasting the biomedical and biopsychosocial perspectives. It delves into theories of pain, specifically Goldschneider’s pattern theory and Melzack and Wall’s gate control theory, critically evaluating their strengths and limitations. The impact of social and emotional experiences on pain management is assessed, highlighting the roles of psychological factors and social support. Finally, the essay evaluates various methods for assessing and controlling pain, considering both physical and psychological interventions. Desklib is a valuable resource for students seeking similar solved assignments and study tools.

Running head: PSYCHOLOGY
Psychology
Name of the student
University name
Author’s note
Psychology
Name of the student
University name
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
PSYCHOLOGY
Table of Contents
1.1 Concepts of health................................................................................................................2
1.2 Critical evaluations of biomedical and biophysical perspectives of health.........................2
3.1 Critical evaluations of theories of pain................................................................................5
3.2 effect of social and emotional experiences on pain management........................................6
3.3 methods for assessment and control of pain........................................................................7
References..................................................................................................................................8
PSYCHOLOGY
Table of Contents
1.1 Concepts of health................................................................................................................2
1.2 Critical evaluations of biomedical and biophysical perspectives of health.........................2
3.1 Critical evaluations of theories of pain................................................................................5
3.2 effect of social and emotional experiences on pain management........................................6
3.3 methods for assessment and control of pain........................................................................7
References..................................................................................................................................8
2
PSYCHOLOGY
1.1 Concepts of health
Health can be defined as overall state of well being within an individual. It is a state
of complete physical, mental and social well being and not merely the absence of disease or
infirmity (Sarafino and Smith 2014). The health defines a state of harmony where all the
organs are functioning to their fullest. The health factor can again be divided into two main
components which are physical and mental health. The physical health refers to a state where
all the body parts are functioning to their fullest capacity and lack a state of disease
(Stoddart and Evans 2017). On the other hand, the mental health refers to a state where the
mind is free from anxieties and is capable to apply sufficient cognition in a decision making.
The World Health organization defines the enjoyment of highest attainable standards
of health as one of the fundamental rights. It refers to unequal development in different in
different countries in the promotion and control of disease as plausible danger. Information
opinion and active cooperation from the public are of utmost importance for the improvement
of the health of the people. As reported by Topp et al. (2015), government is responsible for
the provision of adequate health and social care measures.
1.2 Critical evaluations of biomedical and biophysical perspectives of health
The concept of health varies from individual to individual and could be explained
with the help of a number of theoretical perspectives such as the biomedical and
biopsychosocial perspectives of health. The biomedical model focuses upon the measures
taken by the healthcare professional to find out the relatable cause behind a disease. The
biomedical model views health as the complete absence of disease, pain or defect. The
biomedical model presents the patient as a body that is ill and hence the treatment is provided
independent of the mind.
PSYCHOLOGY
1.1 Concepts of health
Health can be defined as overall state of well being within an individual. It is a state
of complete physical, mental and social well being and not merely the absence of disease or
infirmity (Sarafino and Smith 2014). The health defines a state of harmony where all the
organs are functioning to their fullest. The health factor can again be divided into two main
components which are physical and mental health. The physical health refers to a state where
all the body parts are functioning to their fullest capacity and lack a state of disease
(Stoddart and Evans 2017). On the other hand, the mental health refers to a state where the
mind is free from anxieties and is capable to apply sufficient cognition in a decision making.
The World Health organization defines the enjoyment of highest attainable standards
of health as one of the fundamental rights. It refers to unequal development in different in
different countries in the promotion and control of disease as plausible danger. Information
opinion and active cooperation from the public are of utmost importance for the improvement
of the health of the people. As reported by Topp et al. (2015), government is responsible for
the provision of adequate health and social care measures.
1.2 Critical evaluations of biomedical and biophysical perspectives of health
The concept of health varies from individual to individual and could be explained
with the help of a number of theoretical perspectives such as the biomedical and
biopsychosocial perspectives of health. The biomedical model focuses upon the measures
taken by the healthcare professional to find out the relatable cause behind a disease. The
biomedical model views health as the complete absence of disease, pain or defect. The
biomedical model presents the patient as a body that is ill and hence the treatment is provided
independent of the mind.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
PSYCHOLOGY
The biomedical model of pain focuses upon the neuropsychological aspects for both
treatment and diagnosis. Here, the pain could be divided into different types based upon the
symptoms expressed by the patient such as idiopathic pain. The idiopathic pain is the
condition where there is no observable or physical pathology associated with pain. It has
often been termed as chronic pain syndrome and is governed under the umbrella of medically
unexplained symptoms. As suggested by Quintner et al. (2014), these are symptoms which
do not have an organic pathology governing it. Therefore, this category of pain is given low
clinical importance. The physicians have further referred to these as pain having
somapsychotic origin as they hardly have any physical evidence. As argued by McCracken
and Morley (2014), the biomedical model fails to take into consideration the social and
emotional aspects of pain. Therefore, the idiopathic pain conditions are often ruled out.
There is no single and universally accepted definition of pain. It has been described as
the psychological responses to a range of body symptoms. In the comprehensive sense, pain
has been defined as the “unpleasant feeling caused by injury or disease to the body”. It has
also been referred to as “mental suffering faced by the patient”. As mentioned by Stoddart
and Evans (2017), the treatment should take place in an environment which supports the
adequate use of medical technology.
The biopsychosocial perspective focuses upon the complex interactions of various
biological, psychological and social factors in determining the health of an individual. As
mentioned by Sarafino and Smith (2014), the biopsychosocial perspective helps in the
creation of a fine balance between the different factors stated above. As argued by Zywert
and Quilley (2018), psychological stress can have a huge impact upon the overall health of an
individual. Hence, stress could be an important determinant in determining the health of a
person. Additionally, peer pressure can hugely impact upon the health behaviour adopted by
an individual. For example, drinking is often promoted behaviour is often promoted in an
PSYCHOLOGY
The biomedical model of pain focuses upon the neuropsychological aspects for both
treatment and diagnosis. Here, the pain could be divided into different types based upon the
symptoms expressed by the patient such as idiopathic pain. The idiopathic pain is the
condition where there is no observable or physical pathology associated with pain. It has
often been termed as chronic pain syndrome and is governed under the umbrella of medically
unexplained symptoms. As suggested by Quintner et al. (2014), these are symptoms which
do not have an organic pathology governing it. Therefore, this category of pain is given low
clinical importance. The physicians have further referred to these as pain having
somapsychotic origin as they hardly have any physical evidence. As argued by McCracken
and Morley (2014), the biomedical model fails to take into consideration the social and
emotional aspects of pain. Therefore, the idiopathic pain conditions are often ruled out.
There is no single and universally accepted definition of pain. It has been described as
the psychological responses to a range of body symptoms. In the comprehensive sense, pain
has been defined as the “unpleasant feeling caused by injury or disease to the body”. It has
also been referred to as “mental suffering faced by the patient”. As mentioned by Stoddart
and Evans (2017), the treatment should take place in an environment which supports the
adequate use of medical technology.
The biopsychosocial perspective focuses upon the complex interactions of various
biological, psychological and social factors in determining the health of an individual. As
mentioned by Sarafino and Smith (2014), the biopsychosocial perspective helps in the
creation of a fine balance between the different factors stated above. As argued by Zywert
and Quilley (2018), psychological stress can have a huge impact upon the overall health of an
individual. Hence, stress could be an important determinant in determining the health of a
person. Additionally, peer pressure can hugely impact upon the health behaviour adopted by
an individual. For example, drinking is often promoted behaviour is often promoted in an
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
PSYCHOLOGY
individual as a peer effect. The biopsychososial perspective of pain emphasises upon the
differential responses of the sub-cutanoues receptors which gave rise to different levels of
pain. Here, the unique patterns of stimulation at the nerve endings produced differential
responses (Quintner et al. 2014). The central nervous systems were thought to be responsible
for decoding the different nerve impulses pattern. It divided the receptors into different types
such as mechanoreceptors, thermoreceptors and nociceptors. The mechanoreceptors respond
to touch and pressure, whereas the thermoreceptos are associated with pain perception and
depending on the specific fibre the perception of pain may range from sharp, prickly to
burning or freezing.
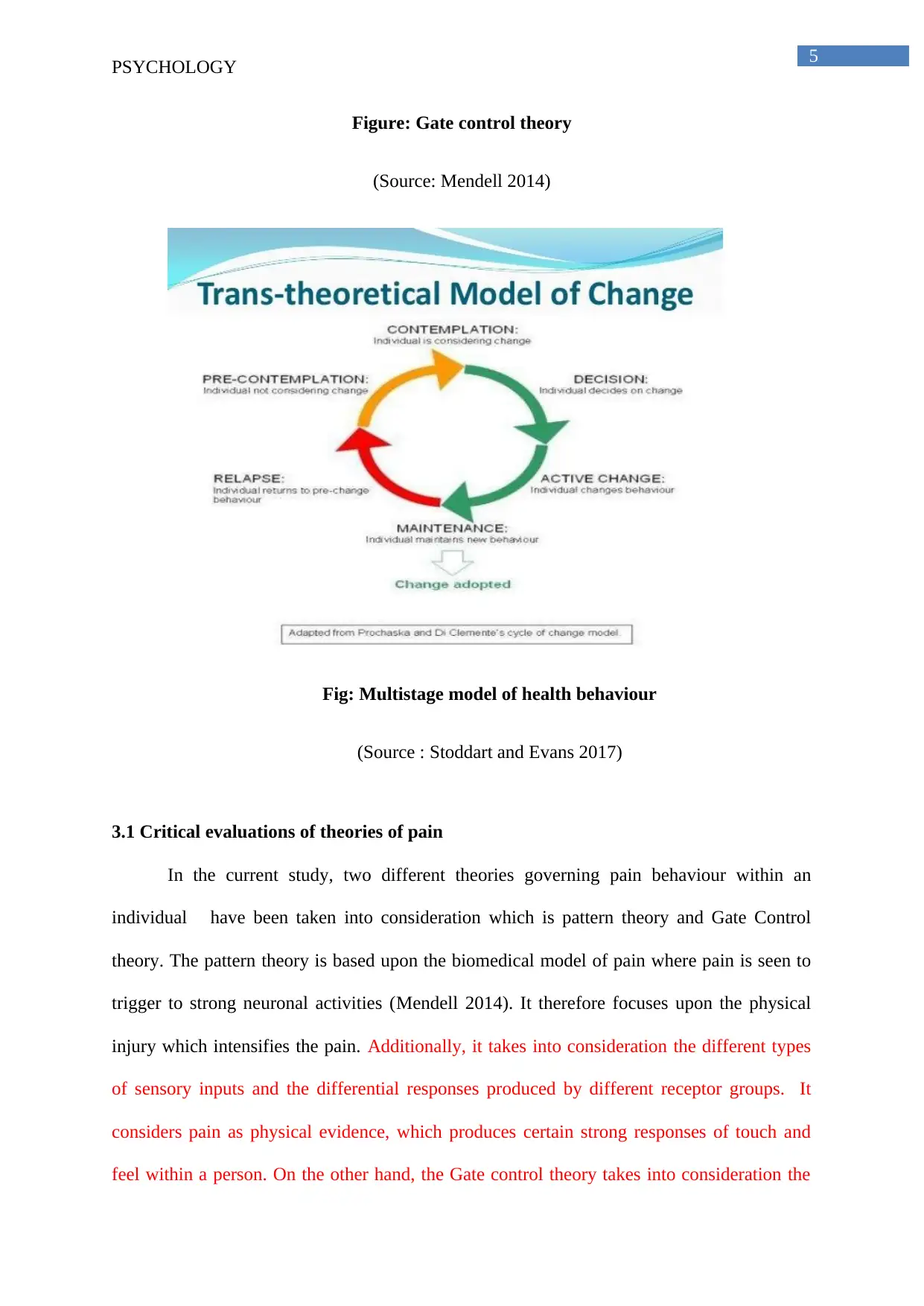
For the current assignment, the aspect of pain and the various factors affecting the
sensation and reception of pain within an individual have been discussed. Some of the
theories which have been highlighted over here are- goldschneider’s pattern theory of pain
and Mlelzack and wall’s Gate control theory. The pattern theory states that pain is felt due to
intense neuronal activities within the brain whereas the Gate control theory provides a
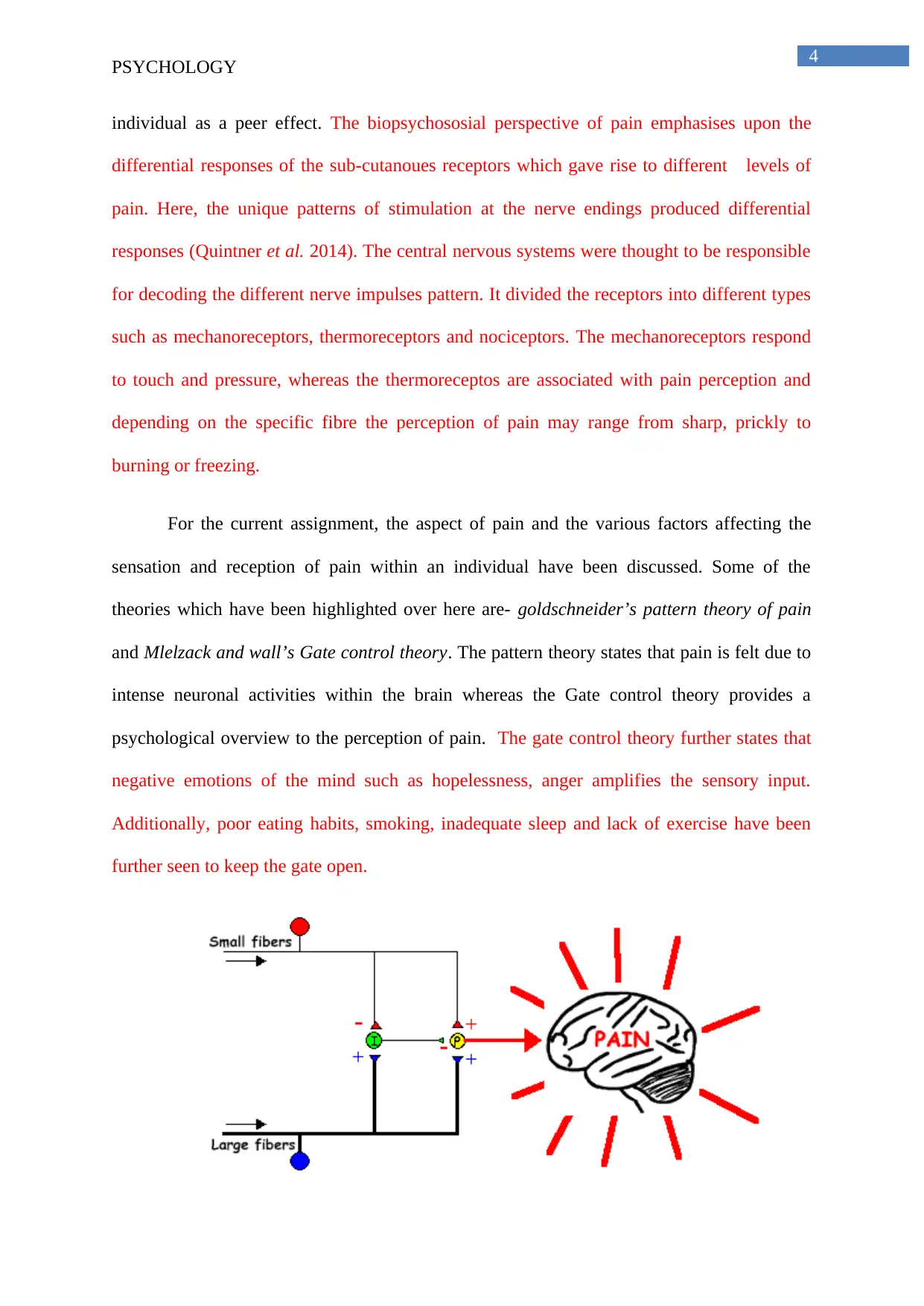
psychological overview to the perception of pain. The gate control theory further states that
negative emotions of the mind such as hopelessness, anger amplifies the sensory input.
Additionally, poor eating habits, smoking, inadequate sleep and lack of exercise have been
further seen to keep the gate open.
PSYCHOLOGY
individual as a peer effect. The biopsychososial perspective of pain emphasises upon the
differential responses of the sub-cutanoues receptors which gave rise to different levels of
pain. Here, the unique patterns of stimulation at the nerve endings produced differential
responses (Quintner et al. 2014). The central nervous systems were thought to be responsible
for decoding the different nerve impulses pattern. It divided the receptors into different types
such as mechanoreceptors, thermoreceptors and nociceptors. The mechanoreceptors respond
to touch and pressure, whereas the thermoreceptos are associated with pain perception and
depending on the specific fibre the perception of pain may range from sharp, prickly to
burning or freezing.
For the current assignment, the aspect of pain and the various factors affecting the
sensation and reception of pain within an individual have been discussed. Some of the
theories which have been highlighted over here are- goldschneider’s pattern theory of pain
and Mlelzack and wall’s Gate control theory. The pattern theory states that pain is felt due to
intense neuronal activities within the brain whereas the Gate control theory provides a
psychological overview to the perception of pain. The gate control theory further states that
negative emotions of the mind such as hopelessness, anger amplifies the sensory input.
Additionally, poor eating habits, smoking, inadequate sleep and lack of exercise have been
further seen to keep the gate open.
5
PSYCHOLOGY
Figure: Gate control theory
(Source: Mendell 2014)
Fig: Multistage model of health behaviour
(Source : Stoddart and Evans 2017)
3.1 Critical evaluations of theories of pain
In the current study, two different theories governing pain behaviour within an
individual have been taken into consideration which is pattern theory and Gate Control
theory. The pattern theory is based upon the biomedical model of pain where pain is seen to
trigger to strong neuronal activities (Mendell 2014). It therefore focuses upon the physical
injury which intensifies the pain. Additionally, it takes into consideration the different types
of sensory inputs and the differential responses produced by different receptor groups. It
considers pain as physical evidence, which produces certain strong responses of touch and
feel within a person. On the other hand, the Gate control theory takes into consideration the
PSYCHOLOGY
Figure: Gate control theory
(Source: Mendell 2014)
Fig: Multistage model of health behaviour
(Source : Stoddart and Evans 2017)
3.1 Critical evaluations of theories of pain
In the current study, two different theories governing pain behaviour within an
individual have been taken into consideration which is pattern theory and Gate Control
theory. The pattern theory is based upon the biomedical model of pain where pain is seen to
trigger to strong neuronal activities (Mendell 2014). It therefore focuses upon the physical
injury which intensifies the pain. Additionally, it takes into consideration the different types
of sensory inputs and the differential responses produced by different receptor groups. It
considers pain as physical evidence, which produces certain strong responses of touch and
feel within a person. On the other hand, the Gate control theory takes into consideration the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
PSYCHOLOGY
emotional state of an individual, which further controls or modulates the transmission of the
nerve impulses.
As mentioned by Montano and Kasprzyk (2015), pain has a psychological definition
to it and perceived differently by different individuals. Therefore, the gate control theory
highlights several important factors such as behavioural training, which results in different
reactions to pain within an individual. The gate control theory divides the pain reception
across two independent pathways –central nervous system and peripheral nervous system.
The Gate control theory states the stimulus of pain travels across the motor neurons to the
central nervous system. However, the impulses have to traverse the ‘nerve gates' in the spinal
cord before they reach the brain (Mendell 2014). The gate control theory states that the
interplay between the small nerve fibres, large nerve and the inhibitory neurons controls the
opening and closing of the ‘nerve gates' and these influenced by the emotional state of an
individual. Therefore, when an individual is a relaxed state the large fibre input is strong
which closes the gate. On the other hand, when the stress is more the small fibre input is
strong, which opens the nerve gates and induces a sensation of pain (Mendell 2014). Hence,
it takes stress as an important guiding force which further modifies the pain behaviour within
an individual.
3.2 Effect of social and emotional experiences on pain management
The social and emotional experiences could have differential impact upon reception
of pain within an individual. As mentioned by Quintner et al. (2014), the responses to pain
are often governed by psychological experiences or past life trauma. Therefore, based upon
these pain could be divided into two important components which are –physical pain and
psychosomatic pain. The physical pain has been defined as a strong response to accidental
traumas.
PSYCHOLOGY
emotional state of an individual, which further controls or modulates the transmission of the
nerve impulses.
As mentioned by Montano and Kasprzyk (2015), pain has a psychological definition
to it and perceived differently by different individuals. Therefore, the gate control theory
highlights several important factors such as behavioural training, which results in different
reactions to pain within an individual. The gate control theory divides the pain reception
across two independent pathways –central nervous system and peripheral nervous system.
The Gate control theory states the stimulus of pain travels across the motor neurons to the
central nervous system. However, the impulses have to traverse the ‘nerve gates' in the spinal
cord before they reach the brain (Mendell 2014). The gate control theory states that the
interplay between the small nerve fibres, large nerve and the inhibitory neurons controls the
opening and closing of the ‘nerve gates' and these influenced by the emotional state of an
individual. Therefore, when an individual is a relaxed state the large fibre input is strong
which closes the gate. On the other hand, when the stress is more the small fibre input is
strong, which opens the nerve gates and induces a sensation of pain (Mendell 2014). Hence,
it takes stress as an important guiding force which further modifies the pain behaviour within
an individual.
3.2 Effect of social and emotional experiences on pain management
The social and emotional experiences could have differential impact upon reception
of pain within an individual. As mentioned by Quintner et al. (2014), the responses to pain
are often governed by psychological experiences or past life trauma. Therefore, based upon
these pain could be divided into two important components which are –physical pain and
psychosomatic pain. The physical pain has been defined as a strong response to accidental
traumas.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
PSYCHOLOGY
Additionally, factors such as social neglect may enhance sensitivity to pain within an
individual (Davis et al. 2015). Emotional experiences such as anxiety and depression further
affects the responsiveness of an individual to pain (McCracken and Morley 2014). On the
other hand, a positive and supportive environment further modulates the pain behaviour
within the patient. As mentioned by Tracy et al. (2015), with effective counselling a patient
has been seen to respond more positively to the sensations of pain.
3.3 Methods for assessment and control of pain
Some of the methods which could be used for the assessment of pain in an individual
within an acute care setup are using measurements tools such as Braden scale. The scale
serves as a measuring unit which rates the pain in patients on a scale of 1-5. Additionally,
simpler tools such as verbal rating tools could be used which classifies pain as mild, moderate
or severe. The pain assessment tool should be selected in due consultation with the patient.
This is because tools selected otherwise without the consent of the patient could be breach of
the confidentiality rights.
PSYCHOLOGY
Additionally, factors such as social neglect may enhance sensitivity to pain within an
individual (Davis et al. 2015). Emotional experiences such as anxiety and depression further
affects the responsiveness of an individual to pain (McCracken and Morley 2014). On the
other hand, a positive and supportive environment further modulates the pain behaviour
within the patient. As mentioned by Tracy et al. (2015), with effective counselling a patient
has been seen to respond more positively to the sensations of pain.
3.3 Methods for assessment and control of pain
Some of the methods which could be used for the assessment of pain in an individual
within an acute care setup are using measurements tools such as Braden scale. The scale
serves as a measuring unit which rates the pain in patients on a scale of 1-5. Additionally,
simpler tools such as verbal rating tools could be used which classifies pain as mild, moderate
or severe. The pain assessment tool should be selected in due consultation with the patient.
This is because tools selected otherwise without the consent of the patient could be breach of
the confidentiality rights.
8
PSYCHOLOGY
References
Davis, R., Campbell, R., Hildon, Z., Hobbs, L. and Michie, S., 2015. Theories of behaviour
and behaviour change across the social and behavioural sciences: a scoping review. Health
psychology review, 9(3), pp.323-344.
Kashikar-Zuck, S., Carle, A., Barnett, K., Goldschneider, K.R., Sherry, D.D., Mara, C.A.,
Cunningham, N., Farrell, J., Tress, J. and DeWitt, E.M., 2016. Longitudinal evaluation of
Patient Reported Outcomes Measurement Information Systems (PROMIS) measures in
pediatric chronic pain. Pain, 157(2), p.339.
McCracken, L.M. and Morley, S., 2014. The psychological flexibility model: a basis for
integration and progress in psychological approaches to chronic pain management. The
Journal of Pain, 15(3), pp.221-234.
Mendell, L.M., 2014. Constructing and deconstructing the gate theory of
pain. PAIN®, 155(2), pp.210-216.
Montano, D.E. and Kasprzyk, D., 2015. Theory of reasoned action, theory of planned
behavior, and the integrated behavioral model. Health behavior: Theory, research and
practice, pp.95-124.
Quintner, J.L., Bove, G.M. and Cohen, M.L., 2014. A critical evaluation of the trigger point
phenomenon. Rheumatology, 54(3), pp.392-399.
Sallis, J.F., Owen, N. and Fisher, E., 2015. Ecological models of health behavior. Health
behavior: Theory, research, and practice, 5, pp.43-64.
Sarafino, E.P. and Smith, T.W., 2014. Health psychology: Biopsychosocial interactions. New
Jersey: John Wiley & Sons, pp. 69-75.
PSYCHOLOGY
References
Davis, R., Campbell, R., Hildon, Z., Hobbs, L. and Michie, S., 2015. Theories of behaviour
and behaviour change across the social and behavioural sciences: a scoping review. Health
psychology review, 9(3), pp.323-344.
Kashikar-Zuck, S., Carle, A., Barnett, K., Goldschneider, K.R., Sherry, D.D., Mara, C.A.,
Cunningham, N., Farrell, J., Tress, J. and DeWitt, E.M., 2016. Longitudinal evaluation of
Patient Reported Outcomes Measurement Information Systems (PROMIS) measures in
pediatric chronic pain. Pain, 157(2), p.339.
McCracken, L.M. and Morley, S., 2014. The psychological flexibility model: a basis for
integration and progress in psychological approaches to chronic pain management. The
Journal of Pain, 15(3), pp.221-234.
Mendell, L.M., 2014. Constructing and deconstructing the gate theory of
pain. PAIN®, 155(2), pp.210-216.
Montano, D.E. and Kasprzyk, D., 2015. Theory of reasoned action, theory of planned
behavior, and the integrated behavioral model. Health behavior: Theory, research and
practice, pp.95-124.
Quintner, J.L., Bove, G.M. and Cohen, M.L., 2014. A critical evaluation of the trigger point
phenomenon. Rheumatology, 54(3), pp.392-399.
Sallis, J.F., Owen, N. and Fisher, E., 2015. Ecological models of health behavior. Health
behavior: Theory, research, and practice, 5, pp.43-64.
Sarafino, E.P. and Smith, T.W., 2014. Health psychology: Biopsychosocial interactions. New
Jersey: John Wiley & Sons, pp. 69-75.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
PSYCHOLOGY
Stoddart, G.L. and Evans, R.G., 2017. Producing health, consuming health care. In Why are
some people healthy and others not? (pp. 27-64). Abingdon: Routledge.
Topp, C.W., Østergaard, S.D., Søndergaard, S. and Bech, P., 2015. The WHO-5 Well-Being
Index: a systematic review of the literature. Psychotherapy and psychosomatics, 84(3),
pp.167-176.
Tracy, L.M., Georgiou-Karistianis, N., Gibson, S.J. and Giummarra, M.J., 2015. Oxytocin
and the modulation of pain experience: implications for chronic pain
management. Neuroscience & Biobehavioral Reviews, 55, pp.53-67.
Zywert, K. and Quilley, S., 2018. Health systems in an era of biophysical limits: the wicked
dilemmas of modernity. Social Theory & Health, 16(2), pp.188-207.
PSYCHOLOGY
Stoddart, G.L. and Evans, R.G., 2017. Producing health, consuming health care. In Why are
some people healthy and others not? (pp. 27-64). Abingdon: Routledge.
Topp, C.W., Østergaard, S.D., Søndergaard, S. and Bech, P., 2015. The WHO-5 Well-Being
Index: a systematic review of the literature. Psychotherapy and psychosomatics, 84(3),
pp.167-176.
Tracy, L.M., Georgiou-Karistianis, N., Gibson, S.J. and Giummarra, M.J., 2015. Oxytocin
and the modulation of pain experience: implications for chronic pain
management. Neuroscience & Biobehavioral Reviews, 55, pp.53-67.
Zywert, K. and Quilley, S., 2018. Health systems in an era of biophysical limits: the wicked
dilemmas of modernity. Social Theory & Health, 16(2), pp.188-207.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.