Health Policy Analysis of the Bonded Medical Program (BMP) - 401363
VerifiedAdded on 2022/09/11
|6
|1370
|27
Report
AI Summary
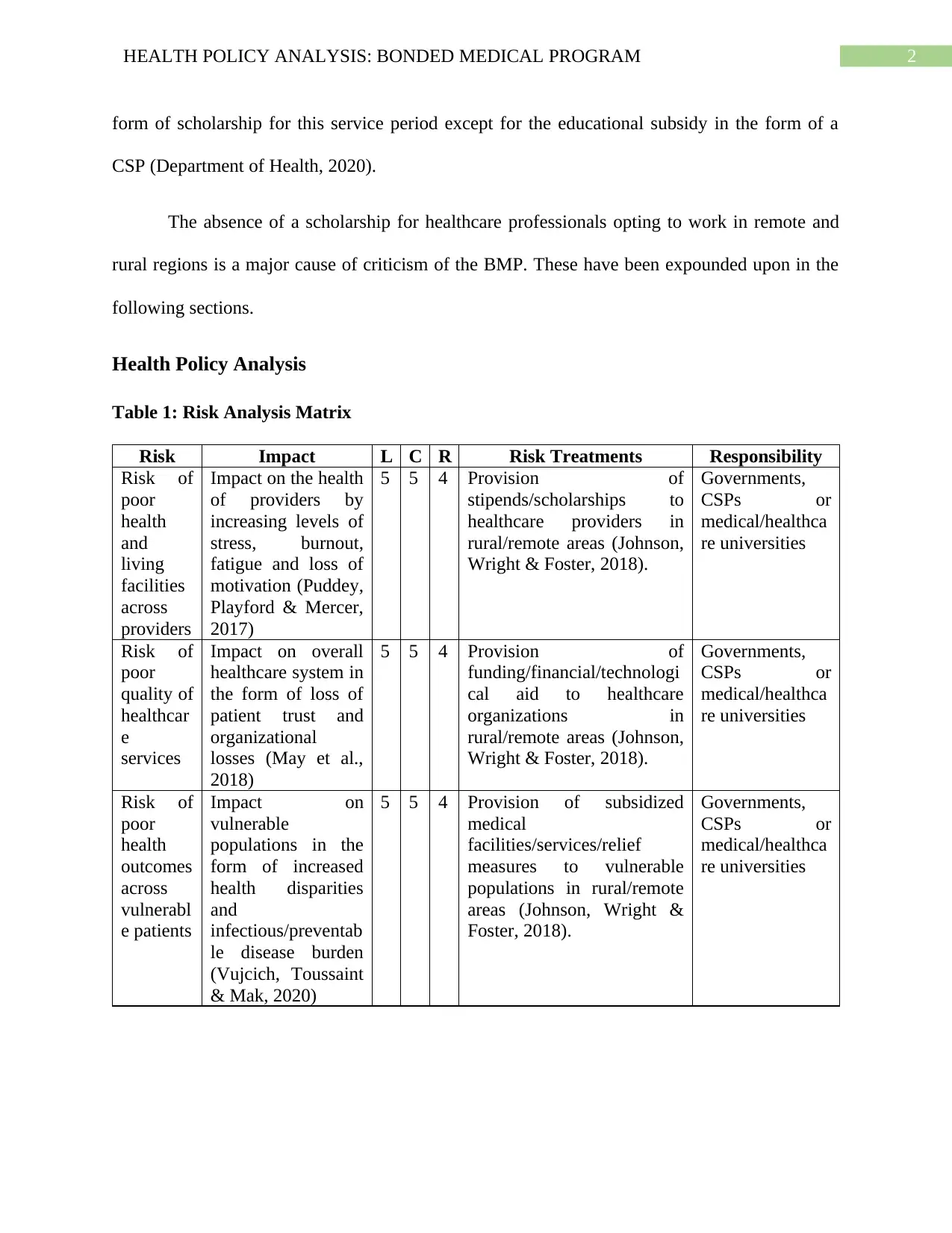
This report provides an in-depth analysis of the Bonded Medical Program (BMP), a health policy implemented in Australia to encourage healthcare professionals to work in rural and remote areas. The report examines the risks associated with the BMP, including the potential for poor health outcomes among providers and patients due to inadequate living conditions and limited resources. A risk analysis matrix is utilized to assess the impact and likelihood of these risks, along with proposed mitigation strategies such as stipends, funding, and subsidized medical facilities. The analysis further explores the BMP's impact on the overall healthcare system and vulnerable populations, highlighting potential violations of universal health coverage principles. The report concludes by emphasizing the need for government incentives and funding to address these risks and improve healthcare access and quality in rural and remote regions. References from the Department of Health and other scholarly articles are included to support the analysis.

1 out of 6
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.