Reporting and Record-keeping in Health and Social Care Analysis
VerifiedAdded on 2023/01/05
|18
|5887
|67
Report
AI Summary
This report delves into the critical aspects of reporting and record-keeping within health and social care settings. It begins by outlining the legal and regulatory frameworks governing these practices, emphasizing the importance of data protection and patient confidentiality as per the Data Protection Act 1998 and the Health and Social Care Act 2008. The report then explores internal and external recording requirements, highlighting the use of electronic and manual systems, and the significance of adherence to NHS code of practice. Furthermore, it examines the role of technology in enhancing record-keeping efficiency, including the use of digital tools and diagnostic technologies. The report also addresses the benefits of involving service users in record-keeping processes and analyzes the ethical and regulatory aspects of maintaining patient records. Finally, it identifies potential challenges in record management and offers recommendations for improvement, with a focus on compliance with national and local policies, and the importance of staff training. The report emphasizes the need for accurate, legible, and concise record-keeping to ensure patient safety and quality of care.
Effective Reporting and
Record-keeping in Health and
Social Care
Record-keeping in Health and
Social Care
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Table of Contents
Describe the legal and regulatory aspects of reporting and record keeping in a care setting..........3
Explore the internal and external recording requirements in a care setting.....................................4
Describe how technology is used in recording and reporting in own care setting..........................7
Explain the benefits of involving service users in record keeping processes..................................8
Review the use of digital technology in relation to own medical management procedures or care
plan..................................................................................................................................................9
Produce accurate, legible, concise and coherent records regarding service user care for different
service users following own setting’s guidelines..........................................................................11
Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines..........................................................14
Analyze the process of maintaining records in own setting, identifying any potential or actual
difficulties......................................................................................................................................15
Conclusion.....................................................................................................................................17
REFERENCES..............................................................................................................................18
Describe the legal and regulatory aspects of reporting and record keeping in a care setting..........3
Explore the internal and external recording requirements in a care setting.....................................4
Describe how technology is used in recording and reporting in own care setting..........................7
Explain the benefits of involving service users in record keeping processes..................................8
Review the use of digital technology in relation to own medical management procedures or care
plan..................................................................................................................................................9
Produce accurate, legible, concise and coherent records regarding service user care for different
service users following own setting’s guidelines..........................................................................11
Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines..........................................................14
Analyze the process of maintaining records in own setting, identifying any potential or actual
difficulties......................................................................................................................................15
Conclusion.....................................................................................................................................17
REFERENCES..............................................................................................................................18
Describe the legal and regulatory aspects of reporting and record keeping in a
care setting
There are several practices for reporting as well as recordkeeping which are very essential in
healthcare setting. These are the activities which are used in social care field in effective manner.
As this field is very delicate committed essential to manage the use of data source information
and ensured perfection and high level of effectiveness of several operation. This is also involved
in ensuring that recordkeeping within areas of health and social wellbeing are very impactful for
linking with external aspects (Akhigbe, Amyot, and Richards, 2019). There are several link
within the internal environment of a care setting that are managed properly. In context of
application within regulatory and legal aspects of practice, it is considered that implementation
of technology within recordkeeping practices and reporting mechanisms are very important for
providing services in care setting. It is very important for this type of organization to manage
laws and regulations properly for managing local as well as national policies.
Legal and regulatory aspects
When management is asked for preparing and compiling reports on data management and
process in health and social care, there is need to manage the legal and regulatory aspects
effectively. There is description within laws and regulations of healthcare for managing various
aspects of healthcare practice. There are several aspects of recordkeeping around regulations and
laws which are used for dealing with information in ethical and confidential manner. It is seen
that information sharing is very important while managing the data and information. In context
of care setting, there are several highly personal information regarding a patient and it is legal to
take protection of these regulatory requirements. It is also essential for maintaining level of trust
and loyal David patients and enhance the level of patient’s safety in organizational premises. In
the present scenario, recordkeeping is the most centrally organised way for the health and life of
patient (Char, Abràmoff, and Feudtner, 2020). There is need to manage the reporting of data
source information and take care of relevant people connected to the healthcare field. There is
need to manage regulatory obligation regarding patient and it is responsibility of authority and
management to share relevant and sufficient information with the 3rd party. In context of
individual neighbour, family, friend , professionals to take care of several individuals within
health and social care workers. There are legal and regulatory requirement that information has
to be handled and protective with care. It is also ensured that protection and authentic use of data
care setting
There are several practices for reporting as well as recordkeeping which are very essential in
healthcare setting. These are the activities which are used in social care field in effective manner.
As this field is very delicate committed essential to manage the use of data source information
and ensured perfection and high level of effectiveness of several operation. This is also involved
in ensuring that recordkeeping within areas of health and social wellbeing are very impactful for
linking with external aspects (Akhigbe, Amyot, and Richards, 2019). There are several link
within the internal environment of a care setting that are managed properly. In context of
application within regulatory and legal aspects of practice, it is considered that implementation
of technology within recordkeeping practices and reporting mechanisms are very important for
providing services in care setting. It is very important for this type of organization to manage
laws and regulations properly for managing local as well as national policies.
Legal and regulatory aspects
When management is asked for preparing and compiling reports on data management and
process in health and social care, there is need to manage the legal and regulatory aspects
effectively. There is description within laws and regulations of healthcare for managing various
aspects of healthcare practice. There are several aspects of recordkeeping around regulations and
laws which are used for dealing with information in ethical and confidential manner. It is seen
that information sharing is very important while managing the data and information. In context
of care setting, there are several highly personal information regarding a patient and it is legal to
take protection of these regulatory requirements. It is also essential for maintaining level of trust
and loyal David patients and enhance the level of patient’s safety in organizational premises. In
the present scenario, recordkeeping is the most centrally organised way for the health and life of
patient (Char, Abràmoff, and Feudtner, 2020). There is need to manage the reporting of data
source information and take care of relevant people connected to the healthcare field. There is
need to manage regulatory obligation regarding patient and it is responsibility of authority and
management to share relevant and sufficient information with the 3rd party. In context of
individual neighbour, family, friend , professionals to take care of several individuals within
health and social care workers. There are legal and regulatory requirement that information has
to be handled and protective with care. It is also ensured that protection and authentic use of data
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
and information associated with patient must be taken care in health and social care. There are
several practices for keeping as well as maintaining records in proper manner and providing
delivery to patients by concerning their personal practice activities. There are some legislations
as well as laws involved in maintaining records and reporting them. According to the Data
Protection Act 1998, there are proper guidelines provided to healthcare management 2 avoid
spreading of information regarding patient to other people (Crowley and et.al, 2020). This is
involved in general data protection regulation and it is ensured that data and information of any
patient is not provided to other people. The process of recording, holding, disclosing and using is
associated with whole process of data protection. In context of whole process, it is seen that the
Data Protection Act 1998 is associated with managing confidentiality of information and
managing need of information for data and protection of patient. In context of care setting, there
are several ways for registered person on protecting and making information safe from any kind
of misuse and exploitation. The health and social Care Act 2008 states that there are different
provisions that must be Provided to the management of healthcare in order to adopt favourable
practices within recordkeeping and reporting. In context of the present scenario individual
information is leaked and his records were not maintained effectively in the care setting. It is
responsibility of management to have non compliance with recordkeeping and reporting which
can lead to criticism within care setting. Consequences for avoidance of legal regulatory in
health and social care can even lead to death. Hence, it is essential for the medical organizations
to take care of patients safety in order to keep the trust and loyalty among patient and healthcare
setting.
Explore the internal and external recording requirements in a care setting
Requirements of internal and external recording
According to the scenario given in the case, it is clear that legal regulatory within healthcare
management must be adopted in order to have better consultation about patients. It is important
for all people to consult with legal regulations and protocols in order to know about internal and
external recording in care setting. There are several local hospitals which refuse to record
patients condition which can lead to problem in future. If a family member had a power of
attorney for the patient and refusal to provide access to record from the medical organization is a
proof for lack of compliance with law. It is also important to have the data and information from
several practices for keeping as well as maintaining records in proper manner and providing
delivery to patients by concerning their personal practice activities. There are some legislations
as well as laws involved in maintaining records and reporting them. According to the Data
Protection Act 1998, there are proper guidelines provided to healthcare management 2 avoid
spreading of information regarding patient to other people (Crowley and et.al, 2020). This is
involved in general data protection regulation and it is ensured that data and information of any
patient is not provided to other people. The process of recording, holding, disclosing and using is
associated with whole process of data protection. In context of whole process, it is seen that the
Data Protection Act 1998 is associated with managing confidentiality of information and
managing need of information for data and protection of patient. In context of care setting, there
are several ways for registered person on protecting and making information safe from any kind
of misuse and exploitation. The health and social Care Act 2008 states that there are different
provisions that must be Provided to the management of healthcare in order to adopt favourable
practices within recordkeeping and reporting. In context of the present scenario individual
information is leaked and his records were not maintained effectively in the care setting. It is
responsibility of management to have non compliance with recordkeeping and reporting which
can lead to criticism within care setting. Consequences for avoidance of legal regulatory in
health and social care can even lead to death. Hence, it is essential for the medical organizations
to take care of patients safety in order to keep the trust and loyalty among patient and healthcare
setting.
Explore the internal and external recording requirements in a care setting
Requirements of internal and external recording
According to the scenario given in the case, it is clear that legal regulatory within healthcare
management must be adopted in order to have better consultation about patients. It is important
for all people to consult with legal regulations and protocols in order to know about internal and
external recording in care setting. There are several local hospitals which refuse to record
patients condition which can lead to problem in future. If a family member had a power of
attorney for the patient and refusal to provide access to record from the medical organization is a
proof for lack of compliance with law. It is also important to have the data and information from
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
an identified individual associated with different aspect of health. This states that mental
wellbeing and physical conditions of a patient must be recorded by the healthcare setting (Fosch-
Villaronga, 2019). There are several ways of keeping the record so that patient can be
recognised immediately. A care setting is chosen for recording information in manual or
electronic form. According to NHS code of practice 2006, the record management is a
mandatory policy which focuses upon medical professionals to have record of every individual
within the healthcare setting. This policy is associated with jurisdiction of NHS in which
managing of both internal as well as external requirement are very important. Within internal and
external recording requirements, it is very important to manage data and information on
electronic as well as paper document. there are several ways for recording The information and
data related to patient. Some of the electronic documents consist of records of care plans,
nutrition, medicines and documents which are used for prescribing the associated medical tests.
Recording is associated with fulfilling of several tools and options which are available within the
healthcare setting for managing chart notes, referrals, history of patients and consultation letters
for managing the health records in care setting. In context of clinical forms, correspondence and
medication list , it is very important to fulfill records requirement in effective manner. There are
several external requirements of recording which are set in context of legal as well as regulatory
requirements for managing the work in proper manner. Aspar public records Act 2005, there is
need of governing and ensuring that medical organizations are keeping records of patients safely
and securely. There is always a keeper of records who has to answer to parliament or
representative of management of healthcare organization who has 2 focus upon increasing safety
of record keeping. It is role and obligation of each and every healthcare professional to manage
the accountability for producing as well as using records and data for several service users and
patients. For a care setting, it is very important to meet legal requirements and attempting to store
record of patients properly. When there is lack of storage or use of records of patient, it can even
lead to death. There are internal as well as external requirements for storing electronic as well as
manual records so that patients are getting appropriate medical treatment. When there is manual
record kept in a safe locker or maintaining electronic records within safety procedures then there
is possibility of fulfilling the obligations under the requirements. This is very important as a legal
or regulatory requirement for insure ceng that records of patients are safe. There are several
concerns regarding recording of patient and these can be linked with recordkeeping in healthcare
wellbeing and physical conditions of a patient must be recorded by the healthcare setting (Fosch-
Villaronga, 2019). There are several ways of keeping the record so that patient can be
recognised immediately. A care setting is chosen for recording information in manual or
electronic form. According to NHS code of practice 2006, the record management is a
mandatory policy which focuses upon medical professionals to have record of every individual
within the healthcare setting. This policy is associated with jurisdiction of NHS in which
managing of both internal as well as external requirement are very important. Within internal and
external recording requirements, it is very important to manage data and information on
electronic as well as paper document. there are several ways for recording The information and
data related to patient. Some of the electronic documents consist of records of care plans,
nutrition, medicines and documents which are used for prescribing the associated medical tests.
Recording is associated with fulfilling of several tools and options which are available within the
healthcare setting for managing chart notes, referrals, history of patients and consultation letters
for managing the health records in care setting. In context of clinical forms, correspondence and
medication list , it is very important to fulfill records requirement in effective manner. There are
several external requirements of recording which are set in context of legal as well as regulatory
requirements for managing the work in proper manner. Aspar public records Act 2005, there is
need of governing and ensuring that medical organizations are keeping records of patients safely
and securely. There is always a keeper of records who has to answer to parliament or
representative of management of healthcare organization who has 2 focus upon increasing safety
of record keeping. It is role and obligation of each and every healthcare professional to manage
the accountability for producing as well as using records and data for several service users and
patients. For a care setting, it is very important to meet legal requirements and attempting to store
record of patients properly. When there is lack of storage or use of records of patient, it can even
lead to death. There are internal as well as external requirements for storing electronic as well as
manual records so that patients are getting appropriate medical treatment. When there is manual
record kept in a safe locker or maintaining electronic records within safety procedures then there
is possibility of fulfilling the obligations under the requirements. This is very important as a legal
or regulatory requirement for insure ceng that records of patients are safe. There are several
concerns regarding recording of patient and these can be linked with recordkeeping in healthcare
setting. It is important to report the concerned managers of healthcare for providing assistance
and guidance.
Reviewing of technology use
There is use of technology within healthcare setting which is very important because By using
technology, there is efficient and perfect way for record keeping. In context of present case, there
is need to develop training program for healthcare staff healthcare staff for using the For using
the new technologies effectively. There is need to have an objective of program for using
technology full stop in this way obligation to record and report services within Healthcare setting
can be managed effectively as well as professionally. There are several employee's who have
taken local as well as national policies as well as guidelines for managing the regulation of
processes by Using the new technology. There are several new employees who have to
understand and analyse use of technology understand and analyse use of technology in order to
employ them in healthcare setting.
The national and local policy guidelines are very important for managing long term plan for
medical organization and this has to focus upon technology. There are several bodies who have
to pursue the policy and manage prioritising technology within healthcare setting. it is also
important to consider and discuss Barrio for recording and reporting services within healthcare
setting. There are several applications which have purpose of managing medical organization as
well as health management application like any app like Fitbit. When there is use of iPads,
computers as well as tablets while managing the record of patients then it is very effective and
convenient. There are several diagnostic technologies which help in making the convenience in
treatment. These are associated with computerised tomographic that is CT scans, EEG, ECG and
other technologies which help in recording and reporting patients data. There are several relevant
websites and these have to be assessed properly for managing the report and record. Digital
medicines are important for effectiveness of technology and using wireless sensors through
telecare as well as monitoring of technology are example of national and local guidelines for
technology enhancement. There are new employees who have to manage several options in
handling and managing technology for health care setting. This can be explained with an
example that medical organizations have to utilise referral service, electronic patient record,
image archive, writing a clinical letter, use of voice recognition as these technologies can help
staff to enhance their performance and keep the patients record properly. It is also inspiring for
and guidance.
Reviewing of technology use
There is use of technology within healthcare setting which is very important because By using
technology, there is efficient and perfect way for record keeping. In context of present case, there
is need to develop training program for healthcare staff healthcare staff for using the For using
the new technologies effectively. There is need to have an objective of program for using
technology full stop in this way obligation to record and report services within Healthcare setting
can be managed effectively as well as professionally. There are several employee's who have
taken local as well as national policies as well as guidelines for managing the regulation of
processes by Using the new technology. There are several new employees who have to
understand and analyse use of technology understand and analyse use of technology in order to
employ them in healthcare setting.
The national and local policy guidelines are very important for managing long term plan for
medical organization and this has to focus upon technology. There are several bodies who have
to pursue the policy and manage prioritising technology within healthcare setting. it is also
important to consider and discuss Barrio for recording and reporting services within healthcare
setting. There are several applications which have purpose of managing medical organization as
well as health management application like any app like Fitbit. When there is use of iPads,
computers as well as tablets while managing the record of patients then it is very effective and
convenient. There are several diagnostic technologies which help in making the convenience in
treatment. These are associated with computerised tomographic that is CT scans, EEG, ECG and
other technologies which help in recording and reporting patients data. There are several relevant
websites and these have to be assessed properly for managing the report and record. Digital
medicines are important for effectiveness of technology and using wireless sensors through
telecare as well as monitoring of technology are example of national and local guidelines for
technology enhancement. There are new employees who have to manage several options in
handling and managing technology for health care setting. This can be explained with an
example that medical organizations have to utilise referral service, electronic patient record,
image archive, writing a clinical letter, use of voice recognition as these technologies can help
staff to enhance their performance and keep the patients record properly. It is also inspiring for
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

organizations to handle policies and guidelines effectively by using the technology in care setting
properly. There is need to keep and maintain record within healthcare setting and managing the
consistency of various requirements of patients. There are 2 main considerations within law and
policy of regulatory requirements which are ethical and regulatory aspect of healthcare setting. In
context of ethical considerations, there is need to manage law and policy which will help in
moral and ethical empowerment. There is also regulatory requirement for insurance lack of
compliance and which will lead to punishment. There is CQC report which has to be made in
perfect manner by the employees. Recordkeeping is compilation of principles of nursing and
midwifery council and the implementation has to take in a local policy of the management.
Moreover, recordkeeping of nurses has to be properly managed in order to present them in front
of any authority. there is ethical consideration of recordkeeping which is associated with
maintaining ethical practices as well as confidentiality for keeping a good record. There are
personal experiences which are very necessary for focusing upon confidentiality and security of
patients record. It is also important to keep and maintain record in electronic as well as manual
form for managing the concerned members within healthcare setting.
Describe how technology is used in recording and reporting in own care
setting
Lately, computation of patient medical records has expanded to a moderate level and this
model appears to continue, particularly as innovation develops and proves more rational. and like
the interest in increasing data on medical services. On the off chance that in the future, patient
medical records are just mechanical changes to most routine records, however, an event will
occur that will cause significant medical care funding to be lost. For example, in the Patient
Registry of Upcoming Events, the board looks for quick access to a range of current cases,
clinical philosophy journey, patient well-being status, and up-to-date data on different treatment
options for the patient's condition. Simple and well-connected computerized information can be
accessed through a computerized medical record, but the accessibility of information
components depends on whether such information is collected and recorded by specialists. In
addition, access to the database and information datasets is required to access new features not
provided by standard patient records.
Thus, the automation of patient record retrieval, maintenance and use of the patient record
are important, though not appropriate, for improving registration. Given the current and growing
properly. There is need to keep and maintain record within healthcare setting and managing the
consistency of various requirements of patients. There are 2 main considerations within law and
policy of regulatory requirements which are ethical and regulatory aspect of healthcare setting. In
context of ethical considerations, there is need to manage law and policy which will help in
moral and ethical empowerment. There is also regulatory requirement for insurance lack of
compliance and which will lead to punishment. There is CQC report which has to be made in
perfect manner by the employees. Recordkeeping is compilation of principles of nursing and
midwifery council and the implementation has to take in a local policy of the management.
Moreover, recordkeeping of nurses has to be properly managed in order to present them in front
of any authority. there is ethical consideration of recordkeeping which is associated with
maintaining ethical practices as well as confidentiality for keeping a good record. There are
personal experiences which are very necessary for focusing upon confidentiality and security of
patients record. It is also important to keep and maintain record in electronic as well as manual
form for managing the concerned members within healthcare setting.
Describe how technology is used in recording and reporting in own care
setting
Lately, computation of patient medical records has expanded to a moderate level and this
model appears to continue, particularly as innovation develops and proves more rational. and like
the interest in increasing data on medical services. On the off chance that in the future, patient
medical records are just mechanical changes to most routine records, however, an event will
occur that will cause significant medical care funding to be lost. For example, in the Patient
Registry of Upcoming Events, the board looks for quick access to a range of current cases,
clinical philosophy journey, patient well-being status, and up-to-date data on different treatment
options for the patient's condition. Simple and well-connected computerized information can be
accessed through a computerized medical record, but the accessibility of information
components depends on whether such information is collected and recorded by specialists. In
addition, access to the database and information datasets is required to access new features not
provided by standard patient records.
Thus, the automation of patient record retrieval, maintenance and use of the patient record
are important, though not appropriate, for improving registration. Given the current and growing
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

nature of the PC and the growing perception of medical care, the committee accepts that it can,
and will, create a record the patient to meet growing needs in the field of medical care. This
section identifies the symptoms of future patient medical records needed to address these issues,
examining some of them in detail to determine the extent and inconsistency of cases you may be
looking out for.
In general, continuous records are coordinated with the sources and order of the
information (Feinstein, 1970), although some selective table designs have been created. For
example, the problem medical record (POMR) is collated from the patient’s complications to
help provide a more coordinated approach to clinical critical thinking and counseling. The
Chronological Synopsis (STOR) is an outpatient medical record framework that contains an
accurate collection of patient medical information that can be used both in relation to the routine
medical record or without anyone else. .
Explain the benefits of involving service users in record keeping processes
The nature of a patient registry or medical record framework depends on its ability to
address user problems and needs. These clients include, however, not only doctors and surgeons
who care for patients. The council followed three standards recommended by the Relentless
Quality Improvement Model to build its vision of a better patient registration and registration
framework: (1) customer identification; (2) understand their needs; and (3) define these
prerequisites in the practical merits of the framework.
The advisory group has strongly identified patient record users as those who enter, verify,
correct, break down or retrieve data from the registry, either directly or through an intermediary.
Each client of the last patient record helps to understand the consideration. However, they differ
in how and why they use the card.
Some customers will have a daily connection to the register, others will access the list on
an irregular basis, and still others will not manage the register, but are dependent on it. the
information obtained from it. An in-depth collection of medical record clients would be
fundamentally similar to a number of individuals and associations that are legitimately or
indirectly connected to the organization of medical care. Persistent messengers provide, monitor,
review or restore routines of silent deliberation; researching clinical or welfare administrations;
educating medical care specialists or patients; creating or managing the progress of medical
services; authorize health care specialists or provider foundations; and deciding on strategic
and will, create a record the patient to meet growing needs in the field of medical care. This
section identifies the symptoms of future patient medical records needed to address these issues,
examining some of them in detail to determine the extent and inconsistency of cases you may be
looking out for.
In general, continuous records are coordinated with the sources and order of the
information (Feinstein, 1970), although some selective table designs have been created. For
example, the problem medical record (POMR) is collated from the patient’s complications to
help provide a more coordinated approach to clinical critical thinking and counseling. The
Chronological Synopsis (STOR) is an outpatient medical record framework that contains an
accurate collection of patient medical information that can be used both in relation to the routine
medical record or without anyone else. .
Explain the benefits of involving service users in record keeping processes
The nature of a patient registry or medical record framework depends on its ability to
address user problems and needs. These clients include, however, not only doctors and surgeons
who care for patients. The council followed three standards recommended by the Relentless
Quality Improvement Model to build its vision of a better patient registration and registration
framework: (1) customer identification; (2) understand their needs; and (3) define these
prerequisites in the practical merits of the framework.
The advisory group has strongly identified patient record users as those who enter, verify,
correct, break down or retrieve data from the registry, either directly or through an intermediary.
Each client of the last patient record helps to understand the consideration. However, they differ
in how and why they use the card.
Some customers will have a daily connection to the register, others will access the list on
an irregular basis, and still others will not manage the register, but are dependent on it. the
information obtained from it. An in-depth collection of medical record clients would be
fundamentally similar to a number of individuals and associations that are legitimately or
indirectly connected to the organization of medical care. Persistent messengers provide, monitor,
review or restore routines of silent deliberation; researching clinical or welfare administrations;
educating medical care specialists or patients; creating or managing the progress of medical
services; authorize health care specialists or provider foundations; and deciding on strategic
medical care options. These types of clients are "messengers" of the patient's medical record, and
their needs should be met by documenting patient structures about what is to come.
Customers are people, but they usually use their skills to interest the premises. The user
summary is an example of the broad summary and shows the wide reach of clients and situations
where silent records are used.
Full publication of client medical records and individual requirements for each was too
expensive for the board. As a result, it identified five important customer classes that it
considered to be the largest and largest producers.
The first step towards improved registration is a close assessment of users on the patient’s
record, accessible progress to create and maintain it, and the barriers to updating. With this in
mind, the Institute of Medicine of the National Academy of Sciences (IOM) has conducted a
study to prescribe improvements to silent records as a result of expanding application needs and
mechanical advances. This report is the result of the multidisciplinary council’s 18-month review
of how you can improve patient medical records to meet the multiple and modified demands for
ongoing data and to improve the nature of patient observation and the appropriateness and
capacity of patients and transfer of medical care.
Review the use of digital technology in relation to own medical management
procedures or care plan.
Development is clinically driven, fueled by new innovations, which change the behavior
of medical care and the management of the wellbeing of our population. However, critical
choices about clinical change and the associated interest in data and information technology
innovation could often be the culmination of NHS board discussions. This must change. These
choices must shift important attention.
Medical care is known around the world to lag at least 10 years behind many industries in
the use of data innovation. It may be a long way from understanding the profitability and value
of improvements seen elsewhere as a retrospective of data innovation. Obvious frustrations in
implementing data innovations have increased pressure on leading employees and neglected to
reduce costs. Follow the basic approach to managing profit margins outside of various businesses
and include improving trade, eliminating duplicates, expanding back office efficiency, and
conducting special visits. These are important and there is still more to be done, but the main
their needs should be met by documenting patient structures about what is to come.
Customers are people, but they usually use their skills to interest the premises. The user
summary is an example of the broad summary and shows the wide reach of clients and situations
where silent records are used.
Full publication of client medical records and individual requirements for each was too
expensive for the board. As a result, it identified five important customer classes that it
considered to be the largest and largest producers.
The first step towards improved registration is a close assessment of users on the patient’s
record, accessible progress to create and maintain it, and the barriers to updating. With this in
mind, the Institute of Medicine of the National Academy of Sciences (IOM) has conducted a
study to prescribe improvements to silent records as a result of expanding application needs and
mechanical advances. This report is the result of the multidisciplinary council’s 18-month review
of how you can improve patient medical records to meet the multiple and modified demands for
ongoing data and to improve the nature of patient observation and the appropriateness and
capacity of patients and transfer of medical care.
Review the use of digital technology in relation to own medical management
procedures or care plan.
Development is clinically driven, fueled by new innovations, which change the behavior
of medical care and the management of the wellbeing of our population. However, critical
choices about clinical change and the associated interest in data and information technology
innovation could often be the culmination of NHS board discussions. This must change. These
choices must shift important attention.
Medical care is known around the world to lag at least 10 years behind many industries in
the use of data innovation. It may be a long way from understanding the profitability and value
of improvements seen elsewhere as a retrospective of data innovation. Obvious frustrations in
implementing data innovations have increased pressure on leading employees and neglected to
reduce costs. Follow the basic approach to managing profit margins outside of various businesses
and include improving trade, eliminating duplicates, expanding back office efficiency, and
conducting special visits. These are important and there is still more to be done, but the main
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
gains lie in longer rationalization and changes in clinical practice. Data frames are a much more
comprehensive tool for change.
Computerized advancements won't convey enhancements in efficiency all alone. For
sure, without cautious usage they can make failures and staff dissatisfaction and even
compromise the nature of care. We have recognized seven exercises that fill in as conditions for
progress from the individuals who have effectively actualized a powerful computerized
methodology.
The impact of clinical data digitization will be further enhanced by clinical advances in
areas such as genomics and diagnostics. The UK is particularly keen to take advantage of
genomic disturbances. The 100,000 Genomes Project expects success of 100,000 whole genomes
from NHS patients by 2017 (Genomics England, 2015). The NHS administration must be the
leading welfare administration on the planet to offer genomic drugs as a standard feature of NHS
patients.
Another view of global medical services is changing rapidly where advanced tactics are
changing the standards of the game. Along with changes within healthcare providers,
development is customer-centric. People generally analyze their wellbeing data effectively and
show a desire to use positive improvements to address their wellbeing and talk to their medical
service provider.
Moving to a carefully enhanced medical service provider does not mean replacing plain
or paper-based ones with advanced ones. Where mechanical centralization has declined,
innovation has been fundamentally grounded on the surface of existing structures and work
projects, making available a unique and additional task for medical care specialists. The
advances that have yielded the best immediate benefits have been carefully designed to simplify
the individual’s situation or connect the patient, with great interest in the plan cycle. Likewise,
those we met on a regular basis have talked about the importance of using innovation to
reconsider the steps of routine work.
Information analysis can drive improvement in a number of areas, including operational
and clinical cycles even as the board is delivered and treatment is streamlined. Sharing
information across a number of key scenarios to support informed thinking and a full
understanding of the benefits of innovation in medical services is outlined in this report. In any
case, there has recently been the power to share and link information between different frames.
comprehensive tool for change.
Computerized advancements won't convey enhancements in efficiency all alone. For
sure, without cautious usage they can make failures and staff dissatisfaction and even
compromise the nature of care. We have recognized seven exercises that fill in as conditions for
progress from the individuals who have effectively actualized a powerful computerized
methodology.
The impact of clinical data digitization will be further enhanced by clinical advances in
areas such as genomics and diagnostics. The UK is particularly keen to take advantage of
genomic disturbances. The 100,000 Genomes Project expects success of 100,000 whole genomes
from NHS patients by 2017 (Genomics England, 2015). The NHS administration must be the
leading welfare administration on the planet to offer genomic drugs as a standard feature of NHS
patients.
Another view of global medical services is changing rapidly where advanced tactics are
changing the standards of the game. Along with changes within healthcare providers,
development is customer-centric. People generally analyze their wellbeing data effectively and
show a desire to use positive improvements to address their wellbeing and talk to their medical
service provider.
Moving to a carefully enhanced medical service provider does not mean replacing plain
or paper-based ones with advanced ones. Where mechanical centralization has declined,
innovation has been fundamentally grounded on the surface of existing structures and work
projects, making available a unique and additional task for medical care specialists. The
advances that have yielded the best immediate benefits have been carefully designed to simplify
the individual’s situation or connect the patient, with great interest in the plan cycle. Likewise,
those we met on a regular basis have talked about the importance of using innovation to
reconsider the steps of routine work.
Information analysis can drive improvement in a number of areas, including operational
and clinical cycles even as the board is delivered and treatment is streamlined. Sharing
information across a number of key scenarios to support informed thinking and a full
understanding of the benefits of innovation in medical services is outlined in this report. In any
case, there has recently been the power to share and link information between different frames.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
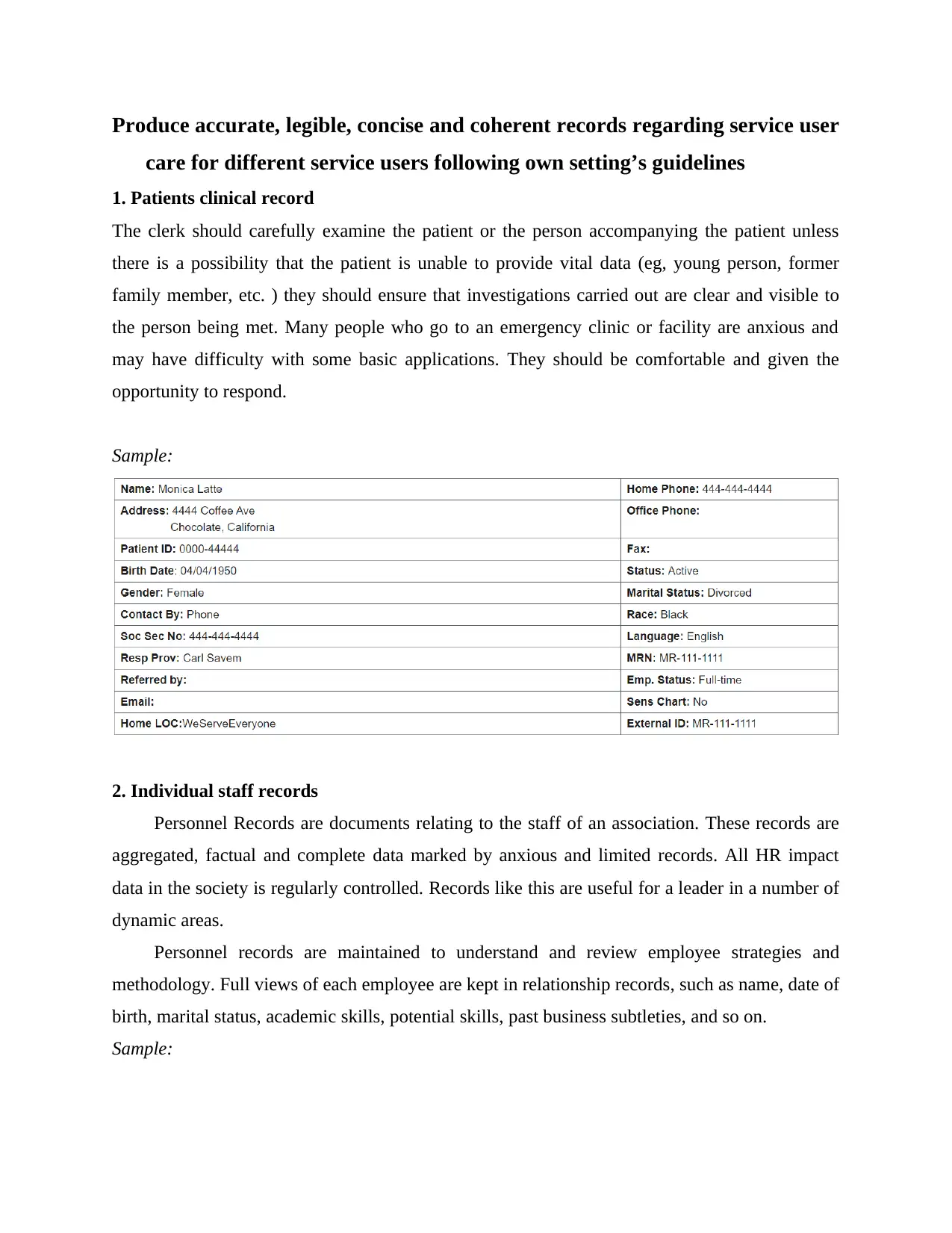
Produce accurate, legible, concise and coherent records regarding service user
care for different service users following own setting’s guidelines
1. Patients clinical record
The clerk should carefully examine the patient or the person accompanying the patient unless
there is a possibility that the patient is unable to provide vital data (eg, young person, former
family member, etc. ) they should ensure that investigations carried out are clear and visible to
the person being met. Many people who go to an emergency clinic or facility are anxious and
may have difficulty with some basic applications. They should be comfortable and given the
opportunity to respond.
Sample:
2. Individual staff records
Personnel Records are documents relating to the staff of an association. These records are
aggregated, factual and complete data marked by anxious and limited records. All HR impact
data in the society is regularly controlled. Records like this are useful for a leader in a number of
dynamic areas.
Personnel records are maintained to understand and review employee strategies and
methodology. Full views of each employee are kept in relationship records, such as name, date of
birth, marital status, academic skills, potential skills, past business subtleties, and so on.
Sample:
care for different service users following own setting’s guidelines
1. Patients clinical record
The clerk should carefully examine the patient or the person accompanying the patient unless
there is a possibility that the patient is unable to provide vital data (eg, young person, former
family member, etc. ) they should ensure that investigations carried out are clear and visible to
the person being met. Many people who go to an emergency clinic or facility are anxious and
may have difficulty with some basic applications. They should be comfortable and given the
opportunity to respond.
Sample:
2. Individual staff records
Personnel Records are documents relating to the staff of an association. These records are
aggregated, factual and complete data marked by anxious and limited records. All HR impact
data in the society is regularly controlled. Records like this are useful for a leader in a number of
dynamic areas.
Personnel records are maintained to understand and review employee strategies and
methodology. Full views of each employee are kept in relationship records, such as name, date of
birth, marital status, academic skills, potential skills, past business subtleties, and so on.
Sample:
3. Ward Records
A separate set of record is required for each employee, providing misconceptions about the
disturbance and their absence, their transportation and promotional exercises and a report note
DEPARTMENT RECORD. These are the records associated with a particular ward.
Standards issued by the Keeper of Public Records under section 12 of the Public Records
Act establishing the agreed maintenance schedules and subsequent transfer actions for the classes
of records held exhibit in these rituals. RDAs proceed with permission to remove these record
classes. RDA can be transparent for one organization or appropriate for more than one office.
A separate set of record is required for each employee, providing misconceptions about the
disturbance and their absence, their transportation and promotional exercises and a report note
DEPARTMENT RECORD. These are the records associated with a particular ward.
Standards issued by the Keeper of Public Records under section 12 of the Public Records
Act establishing the agreed maintenance schedules and subsequent transfer actions for the classes
of records held exhibit in these rituals. RDAs proceed with permission to remove these record
classes. RDA can be transparent for one organization or appropriate for more than one office.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 18
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.