Healthcare Report: Hypertension Significance, Risks, and Prevention
VerifiedAdded on 2020/05/16
|47
|7520
|38
Report
AI Summary
This healthcare report delves into the escalating public health concern of hypertension. It begins with an introduction to the condition, highlighting its increasing global burden and the associated challenges in diagnosis, treatment adherence, and public awareness. The report then explores the significance of studying hypertension, posing key research questions about its impact, risk factors, and prevention strategies. A comprehensive review of literature follows, examining studies on hypertension prevalence, economic impacts, and risk factors such as lifestyle, obesity, and age. The report also discusses the effects of hypertension on quality of life, including physical and mental health aspects. It emphasizes the importance of physical activity and lifestyle modifications in preventing hypertension. The report includes the research methodology, limitations, and recommendations for further research and public health interventions.

1Running head: HEALTHCARE
Healthcare
Name of student:
Name of university:
Author note:
Healthcare
Name of student:
Name of university:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
HEALTHCARE
Table of Contents
I.Introduction..............................................................................................................................3
II.Significance of the Study........................................................................................................4
III.Review of Literature.............................................................................................................5
IV.Research Methodology.......................................................................................................11
V.Limitation/Delimitation........................................................................................................27
VI.Summary.............................................................................................................................28
VII.Recommendations.............................................................................................................28
VIII.Appendix..........................................................................................................................29
IX.References...........................................................................................................................32
HEALTHCARE
Table of Contents
I.Introduction..............................................................................................................................3
II.Significance of the Study........................................................................................................4
III.Review of Literature.............................................................................................................5
IV.Research Methodology.......................................................................................................11
V.Limitation/Delimitation........................................................................................................27
VI.Summary.............................................................................................................................28
VII.Recommendations.............................................................................................................28
VIII.Appendix..........................................................................................................................29
IX.References...........................................................................................................................32
3
HEALTHCARE
I. Introduction
The past one decade has witnessed a rapid increase in the burden of public health
concerns that have drawn the attention of public health departments across the globe.
Research is being conducted extensively to understand the effective strategies that when
applied can ensure prevention of the disease occurrence among the populations. Among the
most notable diseases and health conditions that have emerged as crucial public health
concerns in the recent past is hypertension, as pointed out by (Bakris & Sorrentino, 2017).
Primary hypertension is one of the world’s major risk factors for disease burden and is
expected to be the cause of millions of deaths annually due to cardiovascular diseases when
speaking on a global scale. Hypertension has been strongly correlated with some of the
adverse outcomes individuals can suffer such as heart failure, ischemic heart disease, stroke
and end-stage renal disease. The challenges and concerns regarding management of
hypertension and prevention of the same are unlikely to concede. As per statistical data, the
global burden of hypertension is supposed to increase by almost 60% by 2025. This would
imply that about 1.6 billion adults would be affected by this condition. Considerable
challenges remain in the attempt to decrease the burden of this condition. Firstly, the frequent
un-diagnosis of hypertension is a major issue, and early detection leads to end-organ damage.
Further, a major section of the patient population fails to adhere to the disease management
guidelines. In addition, there is some uncertainty as to the appropriate treatment target for
high-risk patients. Lastly, there is a low level of awareness among the public regarding the
risk factors for hypertension and the course of appropriate care (Iadecola et al., 2016).
A large pool of literature has concentrated on hypertension, encompassing both the
risk factors and preventive measures, but there also lies some limitations of these studies.
Noteworthy progress has not been achieved in understanding the awareness level, treatment
HEALTHCARE
I. Introduction
The past one decade has witnessed a rapid increase in the burden of public health
concerns that have drawn the attention of public health departments across the globe.
Research is being conducted extensively to understand the effective strategies that when
applied can ensure prevention of the disease occurrence among the populations. Among the
most notable diseases and health conditions that have emerged as crucial public health
concerns in the recent past is hypertension, as pointed out by (Bakris & Sorrentino, 2017).
Primary hypertension is one of the world’s major risk factors for disease burden and is
expected to be the cause of millions of deaths annually due to cardiovascular diseases when
speaking on a global scale. Hypertension has been strongly correlated with some of the
adverse outcomes individuals can suffer such as heart failure, ischemic heart disease, stroke
and end-stage renal disease. The challenges and concerns regarding management of
hypertension and prevention of the same are unlikely to concede. As per statistical data, the
global burden of hypertension is supposed to increase by almost 60% by 2025. This would
imply that about 1.6 billion adults would be affected by this condition. Considerable
challenges remain in the attempt to decrease the burden of this condition. Firstly, the frequent
un-diagnosis of hypertension is a major issue, and early detection leads to end-organ damage.
Further, a major section of the patient population fails to adhere to the disease management
guidelines. In addition, there is some uncertainty as to the appropriate treatment target for
high-risk patients. Lastly, there is a low level of awareness among the public regarding the
risk factors for hypertension and the course of appropriate care (Iadecola et al., 2016).
A large pool of literature has concentrated on hypertension, encompassing both the
risk factors and preventive measures, but there also lies some limitations of these studies.
Noteworthy progress has not been achieved in understanding the awareness level, treatment
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
HEALTHCARE
and detection process and control measures that are perceived as important by individuals
across the community. There is a need for further research that can highlight the views and
perceptions of individuals so that the concerns faced by these people can be addressed at the
grass root level (Dominiczak & Kuo, 2018).
II. Significance of the Study
a) Research Questions
Research indicates that there lies a gap in existing literature that highlights the impact of
hypertension on daily lives of individuals across communities. Further, research is also
required to understand the significant risk factors for hypertension in the social and economic
context of communities. In addition, extensive research is required to highlight the suitable
prevention strategies that when applied to the community can arrest the increasing prevalence
of hypertension among individuals. The present research aimed at addressing the following
research questions to gain valuable insights into the important health topic of hypertension-
What is hypertension? What are the main signs and symptoms of hypertension?
What are the important risk factors for developing hypertension?
How does hypertension affect people in their daily lives?
How can hypertension be prevented and the risk of developing the disease be
reduced?
b) Definitions
Hypertension, also termed as high blood pressure, is the long term medical condition
in which the individiauls have persistently elevated blood pressure of the arteries. High blood
pressure does not lead to symptoms when speaking in general terms. High blood pressure is
classified as primary or secondary high blood pressure.
HEALTHCARE
and detection process and control measures that are perceived as important by individuals
across the community. There is a need for further research that can highlight the views and
perceptions of individuals so that the concerns faced by these people can be addressed at the
grass root level (Dominiczak & Kuo, 2018).
II. Significance of the Study
a) Research Questions
Research indicates that there lies a gap in existing literature that highlights the impact of
hypertension on daily lives of individuals across communities. Further, research is also
required to understand the significant risk factors for hypertension in the social and economic
context of communities. In addition, extensive research is required to highlight the suitable
prevention strategies that when applied to the community can arrest the increasing prevalence
of hypertension among individuals. The present research aimed at addressing the following
research questions to gain valuable insights into the important health topic of hypertension-
What is hypertension? What are the main signs and symptoms of hypertension?
What are the important risk factors for developing hypertension?
How does hypertension affect people in their daily lives?
How can hypertension be prevented and the risk of developing the disease be
reduced?
b) Definitions
Hypertension, also termed as high blood pressure, is the long term medical condition
in which the individiauls have persistently elevated blood pressure of the arteries. High blood
pressure does not lead to symptoms when speaking in general terms. High blood pressure is
classified as primary or secondary high blood pressure.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
HEALTHCARE
Blood pressure in humans is measured by the systolic and diastolic pressures,that
denote that manimum and minimum pressures respectively. For healthy adults, the normal
reference range of blood pressure is between 100–130 millimeters mercury (mmHg) systolic
and 60–80 mmHg diastolic pressure. High blood pressure is denoted when the blood pressure
is persistently at or above 30/90 or 140/90 mmHg. For children, the rnage varies between
individuals (Galie et al., 2015).
III. Review of Literature
Hypertension is certainly a leading factor behind premature mortality and what is
striking is that hypertension is preventbale. Mill et al., (2016) carried out a study to examine
the global disparities of prevalenc, control and treatment of hypertension in 2010. A rigorous
literature search was done for concluding the results. In 2010, the proportion of the global
population with hypertension was 31.1%. high income countries contributed to 28.5% of this
number whie low and middle income countries contributed to 31.5%. the age-standardized
prevalence of hypertension witnessed a decrease by 2.6% from the year 2000 to 2010 in high
income countries. In constrast, the number increased by 7.7% in middle and low income
countries. The ultimate conclusion was that global hypertension is on the rise and
collaborative initiatives are required at the earliest for combating the increasing the burden of
hypertension. Hypertension leads to increased healthcare costs as opined by Isllam et al.,
(2015). Major economic burden have been felt on households, individuals, healthcare systems
and the entire nation due to the increasing prevalence of hypertension. Investments to prevent
hypertension would lead to cost-saving, as indicated by previous studies. In a number of
developing countries, and some developed countries, hypertension is often undiagnosed.
Though effective lifestyle interventions and therapies have been articulated across literature,
full control of the growing burden of the disease still remains difficult to achieve.
HEALTHCARE
Blood pressure in humans is measured by the systolic and diastolic pressures,that
denote that manimum and minimum pressures respectively. For healthy adults, the normal
reference range of blood pressure is between 100–130 millimeters mercury (mmHg) systolic
and 60–80 mmHg diastolic pressure. High blood pressure is denoted when the blood pressure
is persistently at or above 30/90 or 140/90 mmHg. For children, the rnage varies between
individuals (Galie et al., 2015).
III. Review of Literature
Hypertension is certainly a leading factor behind premature mortality and what is
striking is that hypertension is preventbale. Mill et al., (2016) carried out a study to examine
the global disparities of prevalenc, control and treatment of hypertension in 2010. A rigorous
literature search was done for concluding the results. In 2010, the proportion of the global
population with hypertension was 31.1%. high income countries contributed to 28.5% of this
number whie low and middle income countries contributed to 31.5%. the age-standardized
prevalence of hypertension witnessed a decrease by 2.6% from the year 2000 to 2010 in high
income countries. In constrast, the number increased by 7.7% in middle and low income
countries. The ultimate conclusion was that global hypertension is on the rise and
collaborative initiatives are required at the earliest for combating the increasing the burden of
hypertension. Hypertension leads to increased healthcare costs as opined by Isllam et al.,
(2015). Major economic burden have been felt on households, individuals, healthcare systems
and the entire nation due to the increasing prevalence of hypertension. Investments to prevent
hypertension would lead to cost-saving, as indicated by previous studies. In a number of
developing countries, and some developed countries, hypertension is often undiagnosed.
Though effective lifestyle interventions and therapies have been articulated across literature,
full control of the growing burden of the disease still remains difficult to achieve.
6
HEALTHCARE
Hypertension in children and adolescents is strikingly detectable. In children, just as
adults, hypertension has been linked with lifestyle factors, obesity and family history of
hypertension. Due to well established epidemic of obesity, high blood pressure prevalence is
also increasing. Though cardiovascular disability and death are not common in children
suffering from hypertension, target organ damage is common such as left ventricular
hypertrophy, retinal vascular changes, thickening of the carotid vessel wall, and even subtle
cognitive change (Falkner, 2010). Lurbe and Ingelfinger (2016) in this regard mentioned that
data present on childhood blood pressure has seen a substantial increase over the past three
decades. The progress marked in data is to be used as research advances that would precisely
translate into clinical practice.
Hu et al., (2017) studied the risk factors for hypertension with the justification that
hypertension is a helaht challenge faced by all countries worldwide. At present, 1.5 billion
people are estimated to suffer from this disease. Blood pressure (BP) values of 120–139/80–
89 mm Hg have a distinct link with increased risk of mortality and cardiovascular morbidity.
Themain reasons for hypertension is fast economic development, urbinsation, population
aging and dietary habits. The researchers undertook a study with multivariate logistic
regression analysis and SPSS for assessing determinants of hypertension. The risk of
hypertension increased with a sharp increase in BMI. There was also a significant correlation
between increasing age and hypertension. Abdominal, smoking and menopause in women
were other risk factors. Another notebale revealation was that the overnall prevelance of
hypertension was higher in males when compared to females. However, the prevalence in
females aged above 65 years was more than that in males belonging to the same age group.
The prevalence of hypertension had the tendency to increase with age, more for people with
age 45 years and above. Further,
HEALTHCARE
Hypertension in children and adolescents is strikingly detectable. In children, just as
adults, hypertension has been linked with lifestyle factors, obesity and family history of
hypertension. Due to well established epidemic of obesity, high blood pressure prevalence is
also increasing. Though cardiovascular disability and death are not common in children
suffering from hypertension, target organ damage is common such as left ventricular
hypertrophy, retinal vascular changes, thickening of the carotid vessel wall, and even subtle
cognitive change (Falkner, 2010). Lurbe and Ingelfinger (2016) in this regard mentioned that
data present on childhood blood pressure has seen a substantial increase over the past three
decades. The progress marked in data is to be used as research advances that would precisely
translate into clinical practice.
Hu et al., (2017) studied the risk factors for hypertension with the justification that
hypertension is a helaht challenge faced by all countries worldwide. At present, 1.5 billion
people are estimated to suffer from this disease. Blood pressure (BP) values of 120–139/80–
89 mm Hg have a distinct link with increased risk of mortality and cardiovascular morbidity.
Themain reasons for hypertension is fast economic development, urbinsation, population
aging and dietary habits. The researchers undertook a study with multivariate logistic
regression analysis and SPSS for assessing determinants of hypertension. The risk of
hypertension increased with a sharp increase in BMI. There was also a significant correlation
between increasing age and hypertension. Abdominal, smoking and menopause in women
were other risk factors. Another notebale revealation was that the overnall prevelance of
hypertension was higher in males when compared to females. However, the prevalence in
females aged above 65 years was more than that in males belonging to the same age group.
The prevalence of hypertension had the tendency to increase with age, more for people with
age 45 years and above. Further,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
HEALTHCARE
According to Mollaoglu et al., (2015) hypertension is a chronic disease that leads to
different organ injury and thus the target for life-long therapy revolves around keeping
hypertension under control. Research indicates that in more than half of the patient
population suffering from hypertension, bood pressure is not controlled optimally.
Hypertension has been denoted to impair significantly the quality of life and shorten the life
span of the individual. This is more prominent in the advanced stages of the disease though
the course is not evident in the initial stages. Hypertensive patients coomonly feel the
psychology of suffering from a chronic disease. They also face challenges and difficulties in
changing their lifestyle so as to control high blood pressure. As a result there is a negative
impact on the quality of life. previous studies had indicated that factors such as exercise and
diet have a negative impact on quality of life in hypertensive patients. the study conducted by
the researchers found that females are more likely to suffer from hypertension than males. It
further highlighted that the majority of patients do not undergo checkups on a regular basis
for hypertensive therapy.
Khaw et al., (2011) carried out a survey to highlighted the health-related quality of
life (HRQOL) among patients suffering from hypertension and compared the same with
general population. the study used the 36-item short form for measuring different aspects of
quality of life of 388 hypertensive patients. the study result indicated that hypertension was
responsible for reducing HRQOL to a considerable degree. Further, cardiovascular
comorbidities exacerbated the reductions. The researchers suggested that future research is
required to understand the effective interventions that can ensure suitbaale HRQOL. Oza et
al., (2014) highlighted that female gender, age, number of symptoms, duration, systolic blood
pressure and number of medications are crucial predictors of QOL in hypertensive patients.
this finding was supported by the research of Pangtey and Singh (2016) who concluded from
their descriptive cross sectional study that most hypertensive patients suffer poor quality of
HEALTHCARE
According to Mollaoglu et al., (2015) hypertension is a chronic disease that leads to
different organ injury and thus the target for life-long therapy revolves around keeping
hypertension under control. Research indicates that in more than half of the patient
population suffering from hypertension, bood pressure is not controlled optimally.
Hypertension has been denoted to impair significantly the quality of life and shorten the life
span of the individual. This is more prominent in the advanced stages of the disease though
the course is not evident in the initial stages. Hypertensive patients coomonly feel the
psychology of suffering from a chronic disease. They also face challenges and difficulties in
changing their lifestyle so as to control high blood pressure. As a result there is a negative
impact on the quality of life. previous studies had indicated that factors such as exercise and
diet have a negative impact on quality of life in hypertensive patients. the study conducted by
the researchers found that females are more likely to suffer from hypertension than males. It
further highlighted that the majority of patients do not undergo checkups on a regular basis
for hypertensive therapy.
Khaw et al., (2011) carried out a survey to highlighted the health-related quality of
life (HRQOL) among patients suffering from hypertension and compared the same with
general population. the study used the 36-item short form for measuring different aspects of
quality of life of 388 hypertensive patients. the study result indicated that hypertension was
responsible for reducing HRQOL to a considerable degree. Further, cardiovascular
comorbidities exacerbated the reductions. The researchers suggested that future research is
required to understand the effective interventions that can ensure suitbaale HRQOL. Oza et
al., (2014) highlighted that female gender, age, number of symptoms, duration, systolic blood
pressure and number of medications are crucial predictors of QOL in hypertensive patients.
this finding was supported by the research of Pangtey and Singh (2016) who concluded from
their descriptive cross sectional study that most hypertensive patients suffer poor quality of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
HEALTHCARE
life. As per the researchers quality of life is a vital outcome for hypertensive patients which
is affected in an adverse manner by both hypertension itself and the side effects of the drugs.
The results of the study further indicated that women had poorer QOL when compared to
men. Other studies such as that of De Carvalho et al., (2013) also point out the same results
that systematic hypertension impairs QOL. Health professionals are to give more attention to
QOL of patients and seek changes in the therapeutic approaches. Social and medical
alternatives having a suitable influence on QOL can be a good approach. A better patient-
docor relationship would also be beneficial for enabling blood pressure control.
Oza et al., (2014) however commented that reports of QOL among patients with
hypertension has been fundamentally conflicting. While some studies point out that QOL
among hypertensives is poor as compared to the general population, other studies point out
that hypertension has no influence on the QOL. Soni et al. (2011) contradicts that HRQOL is
impaired due to comorbidities and complications. The review article of the researchers
pointed out that QOL is poorer when the patient is suffering from co-existent diseases such as
diabetes and chronic kidney disease. Themost prominent impact of hypertension was on the
physcial function domains of QOL. Evidences highlighted that ACE-inhibitors were useful
for improving cardiovascular outcomes and renal outcomes in hypertensive patients.
however, the role in amelioration of QOL outcomes were not established. Wang et al., (2009)
highlighted that hypertension jas been associated with symptoms such as dizziness, anxiety,
tiredness and headache, that lead to increased stress. As a result, patients suffer poor mental
health since their is impaired social functioning, mood and psychological functioning.
Sociodemographic factors such as region of residence, gender, age, marital status, frequency
of activities, educational level, family monthly income and occupation influences dimension
of QOL.
HEALTHCARE
life. As per the researchers quality of life is a vital outcome for hypertensive patients which
is affected in an adverse manner by both hypertension itself and the side effects of the drugs.
The results of the study further indicated that women had poorer QOL when compared to
men. Other studies such as that of De Carvalho et al., (2013) also point out the same results
that systematic hypertension impairs QOL. Health professionals are to give more attention to
QOL of patients and seek changes in the therapeutic approaches. Social and medical
alternatives having a suitable influence on QOL can be a good approach. A better patient-
docor relationship would also be beneficial for enabling blood pressure control.
Oza et al., (2014) however commented that reports of QOL among patients with
hypertension has been fundamentally conflicting. While some studies point out that QOL
among hypertensives is poor as compared to the general population, other studies point out
that hypertension has no influence on the QOL. Soni et al. (2011) contradicts that HRQOL is
impaired due to comorbidities and complications. The review article of the researchers
pointed out that QOL is poorer when the patient is suffering from co-existent diseases such as
diabetes and chronic kidney disease. Themost prominent impact of hypertension was on the
physcial function domains of QOL. Evidences highlighted that ACE-inhibitors were useful
for improving cardiovascular outcomes and renal outcomes in hypertensive patients.
however, the role in amelioration of QOL outcomes were not established. Wang et al., (2009)
highlighted that hypertension jas been associated with symptoms such as dizziness, anxiety,
tiredness and headache, that lead to increased stress. As a result, patients suffer poor mental
health since their is impaired social functioning, mood and psychological functioning.
Sociodemographic factors such as region of residence, gender, age, marital status, frequency
of activities, educational level, family monthly income and occupation influences dimension
of QOL.
9
HEALTHCARE
The worldwide prevalence of hypertension is increasing at an alarming rate and thus
the primary prevention of hypetension is a global health initiative at present. Physical activity
is the most commonly recommended lifestyle modification that aids in prevention of
hypertension. Epidemiological evidence point out that a temporal, consistent, and dose-
dependent relationship exists between physcial activity and hypertension development (Diaz
& Shimbo, 2014). Evidence gathered from interventional studies confirm the association
between hypertension and physical activity in the recent years. However, some questions still
remain unanswered regarding the benefits of physical activity in preventing hypertension,
factors moderating the link between the two and the best prescription for prevention of th
disease.
Fuchs et al., (2010) discussed the prevention of hypertension in patient with
prehypertension. Blood pressure with levels of pre-hypertension confers more cardiovascular
risk and thus has been noted as the intermediate stage for full hypertension. Non-drug
interventions for preventing hypertension have had poor effectiveness. For patients who have
had previous history of diabetes or cardiovasucular disease, the administration of blood
pressure reducing agents is effective in reducing the risk of major cardiovasucalr events. The
early use of drugs that act to lower blood pressure might prevent incidence of hypertension.
The concept that blood pressure lowring agents have marked impacts on patients is rooted in
the minds of the physicians. Some of the clinical trials highlighted that hypertension can be
prevented with the help of drug treatment.
Nutritional factors in management of hypertension has been discussed by a number of
researchers out which the study by Ngueyn et al., (2013) had been important. Hypertension is
a significant cause of mortality and morbidity that take a toll on the lives of patients,
negatively influencing chances of survival. Optimisation of bood pressure has been linked
with improvement in overall health conditions, apart from pharmacological therapies, diertary
HEALTHCARE
The worldwide prevalence of hypertension is increasing at an alarming rate and thus
the primary prevention of hypetension is a global health initiative at present. Physical activity
is the most commonly recommended lifestyle modification that aids in prevention of
hypertension. Epidemiological evidence point out that a temporal, consistent, and dose-
dependent relationship exists between physcial activity and hypertension development (Diaz
& Shimbo, 2014). Evidence gathered from interventional studies confirm the association
between hypertension and physical activity in the recent years. However, some questions still
remain unanswered regarding the benefits of physical activity in preventing hypertension,
factors moderating the link between the two and the best prescription for prevention of th
disease.
Fuchs et al., (2010) discussed the prevention of hypertension in patient with
prehypertension. Blood pressure with levels of pre-hypertension confers more cardiovascular
risk and thus has been noted as the intermediate stage for full hypertension. Non-drug
interventions for preventing hypertension have had poor effectiveness. For patients who have
had previous history of diabetes or cardiovasucular disease, the administration of blood
pressure reducing agents is effective in reducing the risk of major cardiovasucalr events. The
early use of drugs that act to lower blood pressure might prevent incidence of hypertension.
The concept that blood pressure lowring agents have marked impacts on patients is rooted in
the minds of the physicians. Some of the clinical trials highlighted that hypertension can be
prevented with the help of drug treatment.
Nutritional factors in management of hypertension has been discussed by a number of
researchers out which the study by Ngueyn et al., (2013) had been important. Hypertension is
a significant cause of mortality and morbidity that take a toll on the lives of patients,
negatively influencing chances of survival. Optimisation of bood pressure has been linked
with improvement in overall health conditions, apart from pharmacological therapies, diertary
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
HEALTHCARE
modification as a nonpharmacological approach plays a crucial role in the control of blood
pressure. The main dietary components have been pointed out to be calcium, sodium,
potassium, fibre and magnesium. These nutritional factors have been repeatedly used as a
robust strategy for controlling blood pressre, mainly in the early stages of hypertension (SBP
140–159 mmHg and/or DBP 90–99 mmHg). Strong evidences are present that recommend
the consumption of a diet that has rich potassium, high fibre and low alcohol intake. A
patterned diet with high content of fruits, low-fat diary products, vegetables, fish, nuts and
whole grains, and low content of fat, red meat and sugar-sweetended food have been
recommended. Pharmacological supplements for achieving these goals pertaining to diet has
not been advised. The recommendation outlined above is not very clear and lacks consistency
across research. Nevertheless, recommendations for nutritional therapy have been effective in
reduction of blood pressure and reducing overall mortality due to hypertension related
complications.
Ferdinand et al., (2012) put forward a valuable literature on the community based
approaches for prevention and management of cardiovascular disease and hypertension.
Community hypertension has reached to a level where improvement of public health has been
thought important. Hypertension is certainly the leading cause of cardiovascular disease,
accounting for almost 66% of the deaths in the US. The other risk factors include obesity,
high cholesterol and obesity. A public health approach to hypertension reduces the rate of
mortality and morbidity related to hypertension. Further, it curtails the high costs of
healthcare. Thus, public health interventions for hypertension promises to diminish the risk of
cardiovascular diseases too. It is to be mentioned that educating people about lifestyle
modifications, healthy eating and regular exercise can be effective in this regard.
HEALTHCARE
modification as a nonpharmacological approach plays a crucial role in the control of blood
pressure. The main dietary components have been pointed out to be calcium, sodium,
potassium, fibre and magnesium. These nutritional factors have been repeatedly used as a
robust strategy for controlling blood pressre, mainly in the early stages of hypertension (SBP
140–159 mmHg and/or DBP 90–99 mmHg). Strong evidences are present that recommend
the consumption of a diet that has rich potassium, high fibre and low alcohol intake. A
patterned diet with high content of fruits, low-fat diary products, vegetables, fish, nuts and
whole grains, and low content of fat, red meat and sugar-sweetended food have been
recommended. Pharmacological supplements for achieving these goals pertaining to diet has
not been advised. The recommendation outlined above is not very clear and lacks consistency
across research. Nevertheless, recommendations for nutritional therapy have been effective in
reduction of blood pressure and reducing overall mortality due to hypertension related
complications.
Ferdinand et al., (2012) put forward a valuable literature on the community based
approaches for prevention and management of cardiovascular disease and hypertension.
Community hypertension has reached to a level where improvement of public health has been
thought important. Hypertension is certainly the leading cause of cardiovascular disease,
accounting for almost 66% of the deaths in the US. The other risk factors include obesity,
high cholesterol and obesity. A public health approach to hypertension reduces the rate of
mortality and morbidity related to hypertension. Further, it curtails the high costs of
healthcare. Thus, public health interventions for hypertension promises to diminish the risk of
cardiovascular diseases too. It is to be mentioned that educating people about lifestyle
modifications, healthy eating and regular exercise can be effective in this regard.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
HEALTHCARE
IV. Research Methodology
A) Subjects
A online survey was carried out for addressing the research questions on
hypertension. 100 participants were selected for this purpose. The population information
was collected from a city retail store after getting their approval. The persons were contacted
individually over telephone and the purpose of the research was explained to them. They
were motivated to take part in the research as it was directed towards understanding health
behaviours of individuals.
B) Data Collection Methods
A questionnaire with 25 questions was prepared keeping in mind the research
objectives that acted as the data collection tool. There are some distinct advantages of using
questionnaires as the data collection tool in a research, the most important one being the fact
that it is the most practical way of collecting data. Large volume of information can be
collected from a group of people within a short span of time. It is also a cost effective
process. The results of the questionnaires can be quantified in a easy manner and analysis is
objectively done. The questionnaire has been attached in the appendix.
C) Role of the Researcher
The main role of the researcher was to motivate the respondents to take part in the
study and provide adequate responses. Gaining informed constent from the respondents prior
to research was of prime importance as an ethical principle.
D) Data analysis
This section analyses the data collecton from online survey as the form of primary
data. The data is represented in graphical form that would help to analyse the information for
drawing in inferences from the study.
HEALTHCARE
IV. Research Methodology
A) Subjects
A online survey was carried out for addressing the research questions on
hypertension. 100 participants were selected for this purpose. The population information
was collected from a city retail store after getting their approval. The persons were contacted
individually over telephone and the purpose of the research was explained to them. They
were motivated to take part in the research as it was directed towards understanding health
behaviours of individuals.
B) Data Collection Methods
A questionnaire with 25 questions was prepared keeping in mind the research
objectives that acted as the data collection tool. There are some distinct advantages of using
questionnaires as the data collection tool in a research, the most important one being the fact
that it is the most practical way of collecting data. Large volume of information can be
collected from a group of people within a short span of time. It is also a cost effective
process. The results of the questionnaires can be quantified in a easy manner and analysis is
objectively done. The questionnaire has been attached in the appendix.
C) Role of the Researcher
The main role of the researcher was to motivate the respondents to take part in the
study and provide adequate responses. Gaining informed constent from the respondents prior
to research was of prime importance as an ethical principle.
D) Data analysis
This section analyses the data collecton from online survey as the form of primary
data. The data is represented in graphical form that would help to analyse the information for
drawing in inferences from the study.
12
HEALTHCARE
The following are the results of the survey done with the questionnaire-
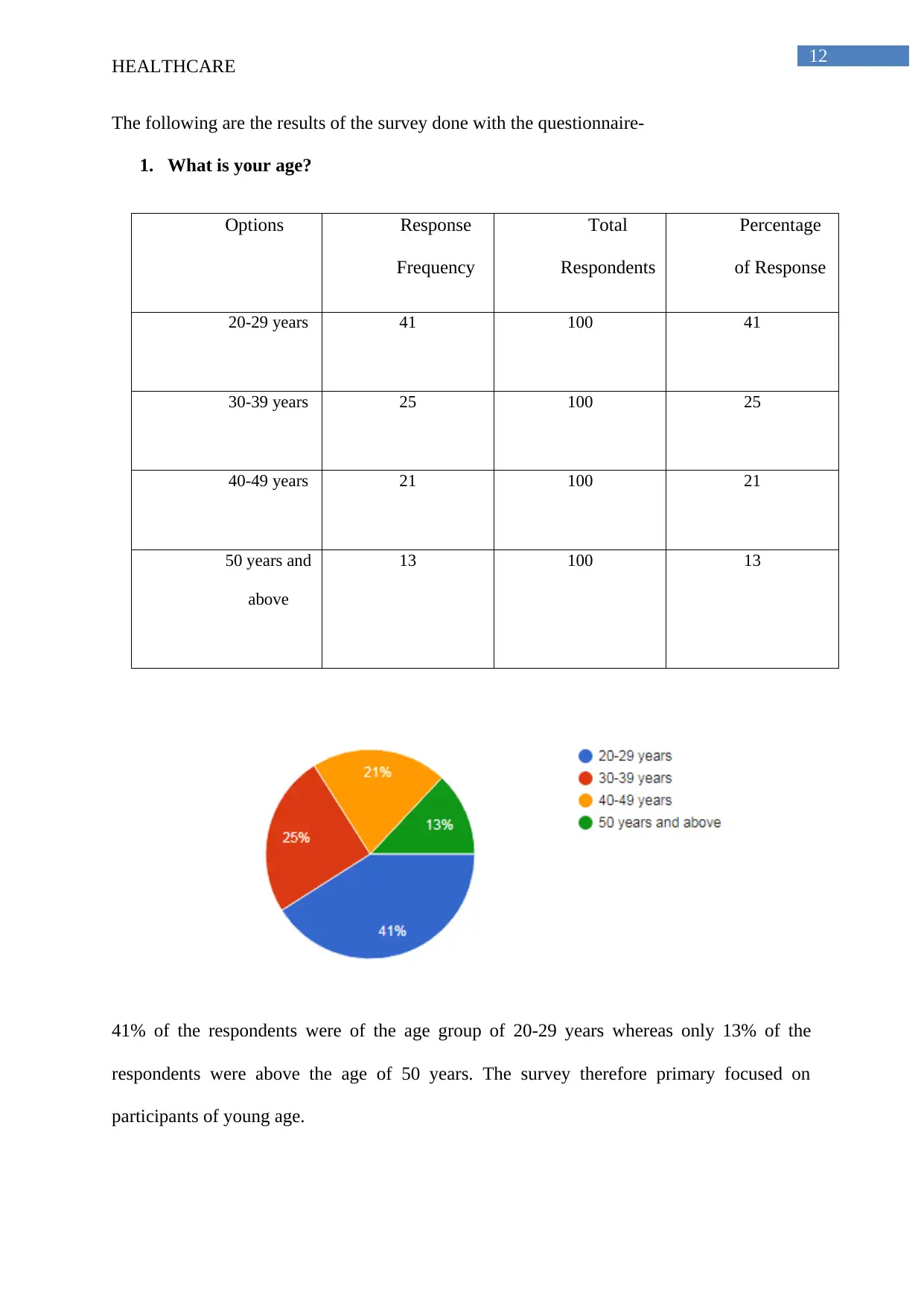
1. What is your age?
Options Response
Frequency
Total
Respondents
Percentage
of Response
20-29 years 41 100 41
30-39 years 25 100 25
40-49 years 21 100 21
50 years and
above
13 100 13
41% of the respondents were of the age group of 20-29 years whereas only 13% of the
respondents were above the age of 50 years. The survey therefore primary focused on
participants of young age.
HEALTHCARE
The following are the results of the survey done with the questionnaire-
1. What is your age?
Options Response
Frequency
Total
Respondents
Percentage
of Response
20-29 years 41 100 41
30-39 years 25 100 25
40-49 years 21 100 21
50 years and
above
13 100 13
41% of the respondents were of the age group of 20-29 years whereas only 13% of the
respondents were above the age of 50 years. The survey therefore primary focused on
participants of young age.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 47
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.