IT Healthcare Systems: EHR, Regulations, and Incentives
VerifiedAdded on 2022/10/04
|11
|2260
|155
Report
AI Summary
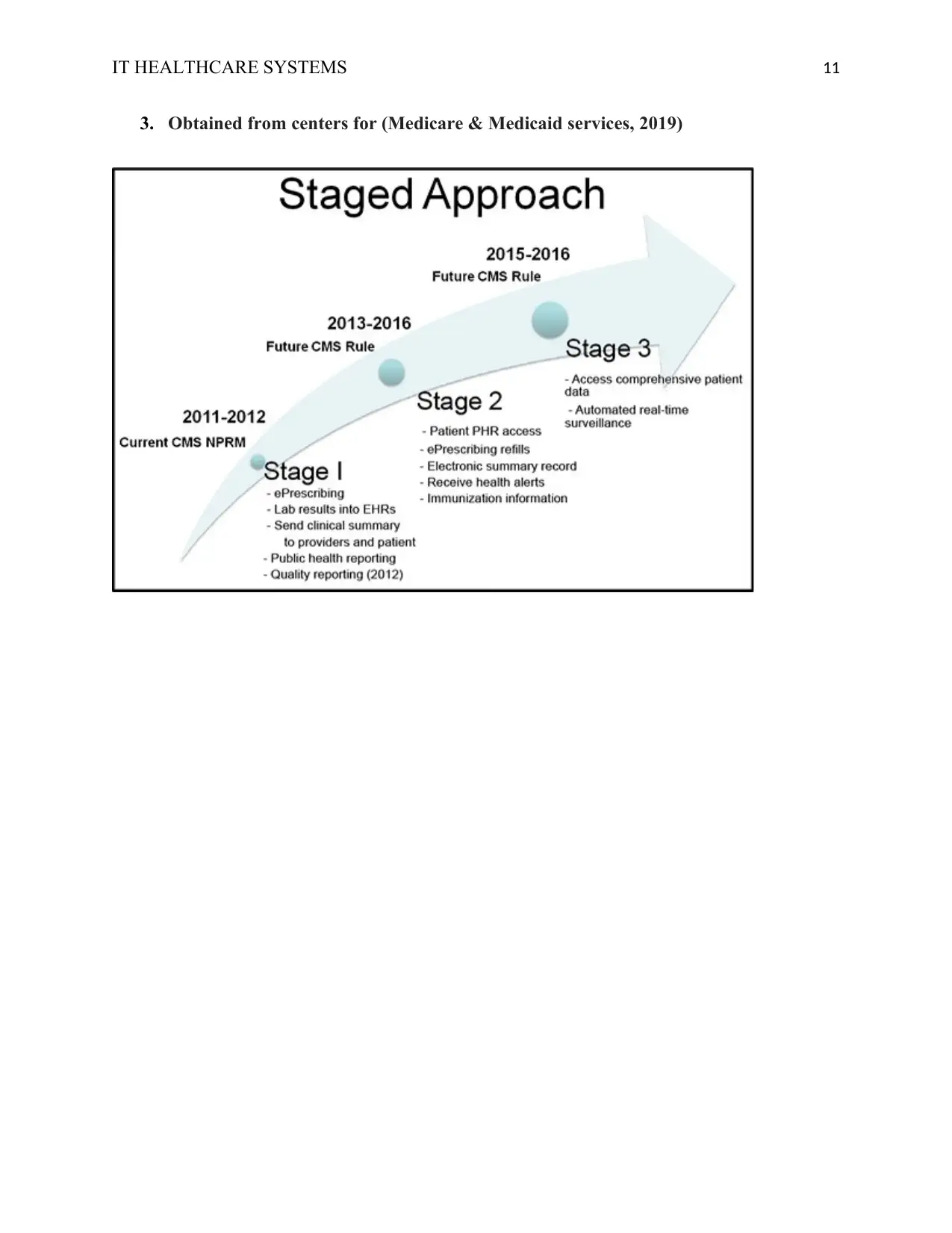
This report provides a comprehensive overview of the integration of Information Technology (IT) within healthcare systems. It explores the significant impact of IT on healthcare delivery, emphasizing the role of Electronic Health Records (EHRs) in enhancing patient care and achieving health equity. The report delves into the implications and uses of IT, highlighting its capacity to improve the safety, quality, and efficiency of healthcare services. It examines the applicable statutes and regulations governing EHRs in the United States, including the HITECH Act and the Meaningful Use program, which provide financial incentives for the adoption of certified EHR technology. The report discusses the benefits of EHRs, such as improved access to patient information, reduced medical errors, and enhanced patient-provider interaction. It also references real-world examples like Kaiser Permanente's EHR system and the Department of Veterans Affairs' system. Furthermore, it acknowledges the challenges and costs associated with EHR implementation, while underscoring IT's vital role in transforming healthcare and improving patient outcomes.


1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.