Analysis of Healthcare Operations Using Queuing Theory and Models
VerifiedAdded on 2021/02/20
|7
|1282
|54
Report
AI Summary
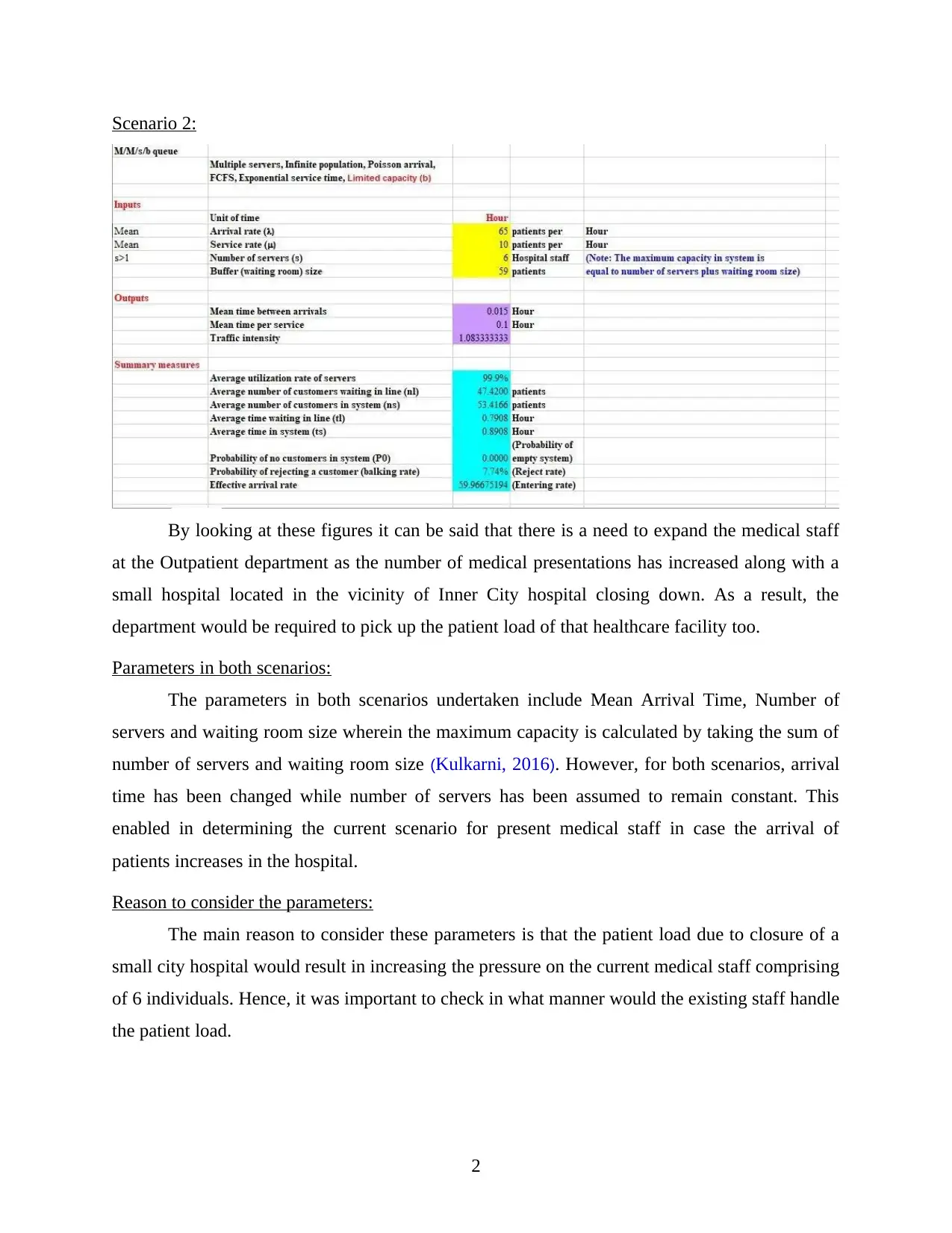
This report analyzes healthcare operations using queuing theory, specifically focusing on an M/M/s/b model to evaluate the outpatient unit's performance under different scenarios. Scenario 1 examines the current patient load, while Scenario 2 considers an increased arrival rate due to the closure of a nearby hospital. The parameters considered include mean arrival time, number of servers, and waiting room size. The report highlights the impact of increased patient load on server utilization, waiting times, and rejection rates, concluding that expansion of medical staff is necessary. The analysis uses formulas to calculate average utilization rate, number of customers waiting in line, and probability of customer rejection. The report emphasizes the role of queuing theory in making informed decisions about resource allocation and service delivery in healthcare settings, providing valuable insights for healthcare managers to optimize patient flow and ensure sustainable service.



1 out of 7

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.