Hematological Complains Analysis: Types, Diagnosis, and Treatments
VerifiedAdded on 2022/09/21
|5
|765
|16
Homework Assignment
AI Summary
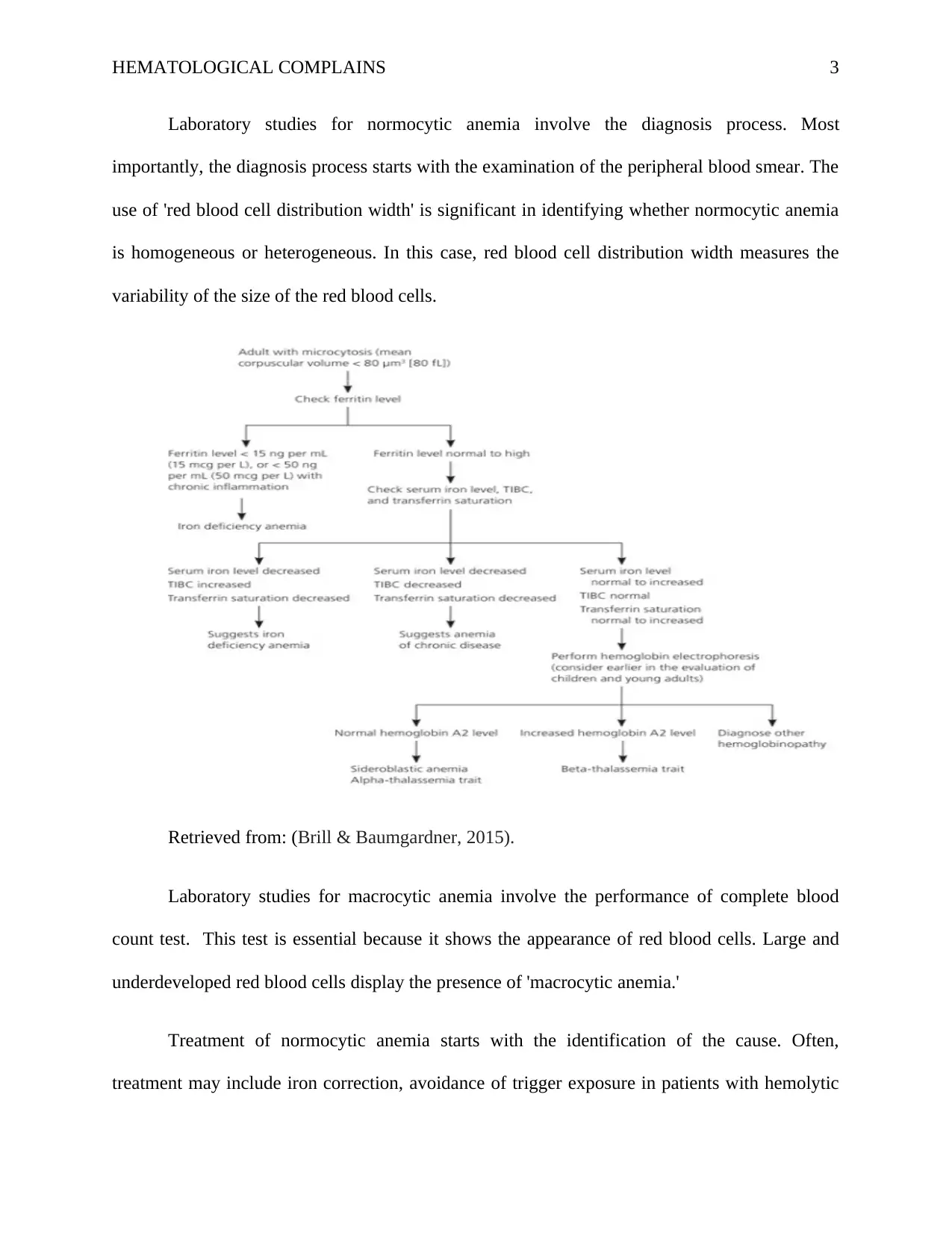
This assignment provides a detailed overview of hematological complains, specifically focusing on anemia. It begins by defining anemia and then outlines the three main types: microcytic, normocytic, and macrocytic anemia. The assignment explains the causes and characteristics of each type, including the role of red blood cell size and number. It then delves into laboratory studies used for diagnosis, such as ferritin levels, serum iron tests, and complete blood counts. The assignment also covers treatment approaches for each type of anemia, including iron correction, avoidance of triggers, vitamin B12 supplementation, and blood transfusions. The document references several sources to support its findings.


1 out of 5
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.