Health Impact Assessment Screening Report: Tobacco Control Policy
VerifiedAdded on 2023/06/15
|9
|2291
|369
Report
AI Summary
This assignment presents a health impact assessment (HIA) screening report focused on the proposed tobacco control strategy in Queensland, Australia, based on the National Tobacco Strategy 2012-2018. The screening report addresses key questions related to the project's timing, potential health impacts (including environmental and social determinants), health inequities, and the significance of impacts, while also considering existing evidence and the decision-making process. The reflective report discusses the rationale for the HIA, initial assumptions, surprising data findings, stakeholder engagement, and barriers encountered during the screening and scoping process, such as dealing with multilingual populations and integrating research evidence. The report concludes that HIA is a valuable tool for informing policy decisions and improving public health outcomes, despite potential criticisms regarding evidence utilization, highlighting the importance of considering various factors influencing individual health and maximizing health gain opportunities.

Running head: HEALTH IMPACT ASSESSMENT SCREENING
Health Impact Assessment Screening
Name of the Student
Name of the University
Author note
Health Impact Assessment Screening
Name of the Student
Name of the University
Author note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1HEALTH IMPACT ASSESSMENT SCREENING
1. Screening Report
Screening Questions Response and Supporting Facts
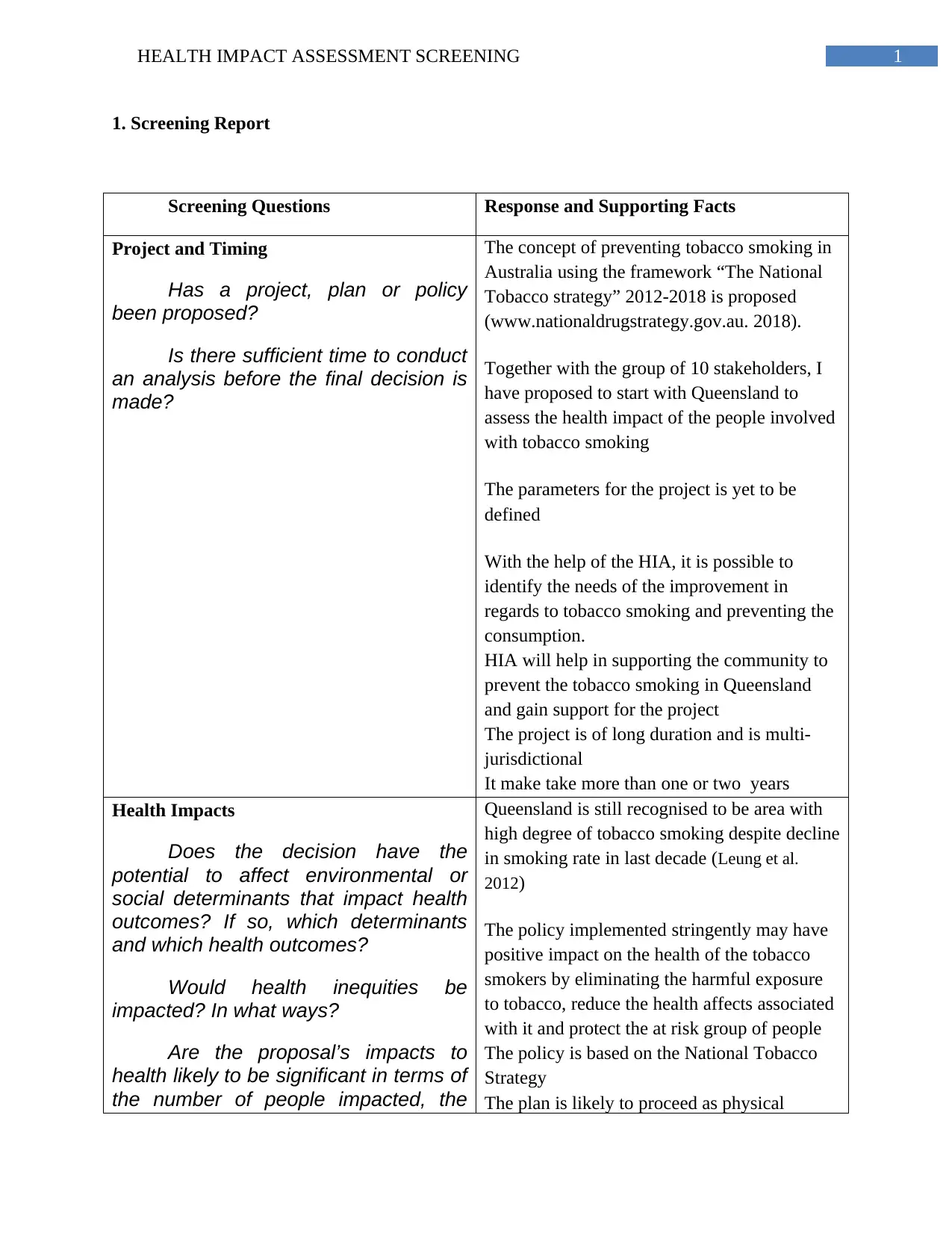
Project and Timing
Has a project, plan or policy
been proposed?
Is there sufficient time to conduct
an analysis before the final decision is
made?
The concept of preventing tobacco smoking in
Australia using the framework “The National
Tobacco strategy” 2012-2018 is proposed
(www.nationaldrugstrategy.gov.au. 2018).
Together with the group of 10 stakeholders, I
have proposed to start with Queensland to
assess the health impact of the people involved
with tobacco smoking
The parameters for the project is yet to be
defined
With the help of the HIA, it is possible to
identify the needs of the improvement in
regards to tobacco smoking and preventing the
consumption.
HIA will help in supporting the community to
prevent the tobacco smoking in Queensland
and gain support for the project
The project is of long duration and is multi-
jurisdictional
It make take more than one or two years
Health Impacts
Does the decision have the
potential to affect environmental or
social determinants that impact health
outcomes? If so, which determinants
and which health outcomes?
Would health inequities be
impacted? In what ways?
Are the proposal’s impacts to
health likely to be significant in terms of
the number of people impacted, the
Queensland is still recognised to be area with
high degree of tobacco smoking despite decline
in smoking rate in last decade (Leung et al.
2012)
The policy implemented stringently may have
positive impact on the health of the tobacco
smokers by eliminating the harmful exposure
to tobacco, reduce the health affects associated
with it and protect the at risk group of people
The policy is based on the National Tobacco
Strategy
The plan is likely to proceed as physical
1. Screening Report
Screening Questions Response and Supporting Facts
Project and Timing
Has a project, plan or policy
been proposed?
Is there sufficient time to conduct
an analysis before the final decision is
made?
The concept of preventing tobacco smoking in
Australia using the framework “The National
Tobacco strategy” 2012-2018 is proposed
(www.nationaldrugstrategy.gov.au. 2018).
Together with the group of 10 stakeholders, I
have proposed to start with Queensland to
assess the health impact of the people involved
with tobacco smoking
The parameters for the project is yet to be
defined
With the help of the HIA, it is possible to
identify the needs of the improvement in
regards to tobacco smoking and preventing the
consumption.
HIA will help in supporting the community to
prevent the tobacco smoking in Queensland
and gain support for the project
The project is of long duration and is multi-
jurisdictional
It make take more than one or two years
Health Impacts
Does the decision have the
potential to affect environmental or
social determinants that impact health
outcomes? If so, which determinants
and which health outcomes?
Would health inequities be
impacted? In what ways?
Are the proposal’s impacts to
health likely to be significant in terms of
the number of people impacted, the
Queensland is still recognised to be area with
high degree of tobacco smoking despite decline
in smoking rate in last decade (Leung et al.
2012)
The policy implemented stringently may have
positive impact on the health of the tobacco
smokers by eliminating the harmful exposure
to tobacco, reduce the health affects associated
with it and protect the at risk group of people
The policy is based on the National Tobacco
Strategy
The plan is likely to proceed as physical
2HEALTH IMPACT ASSESSMENT SCREENING
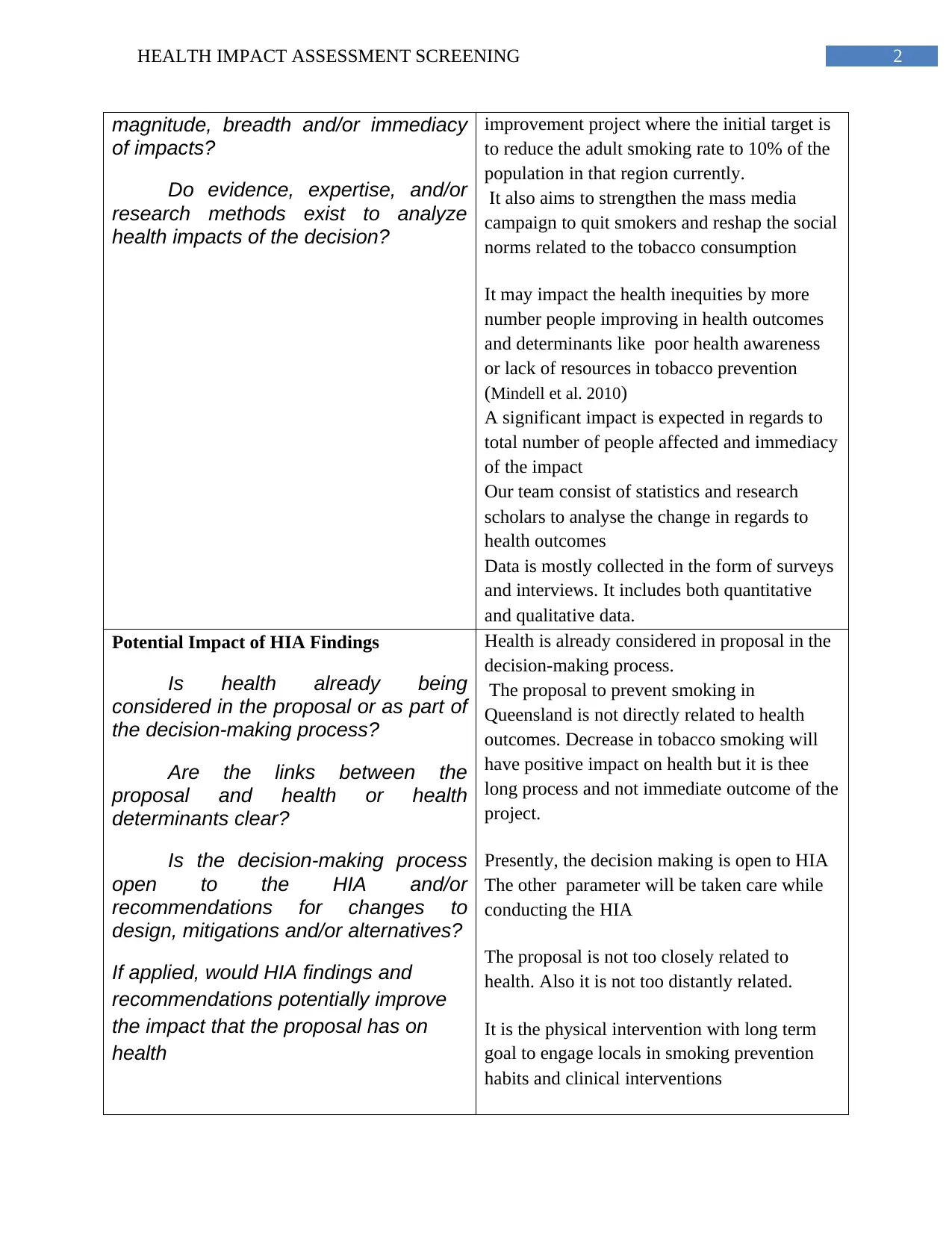
magnitude, breadth and/or immediacy
of impacts?
Do evidence, expertise, and/or
research methods exist to analyze
health impacts of the decision?
improvement project where the initial target is
to reduce the adult smoking rate to 10% of the
population in that region currently.
It also aims to strengthen the mass media
campaign to quit smokers and reshap the social
norms related to the tobacco consumption
It may impact the health inequities by more
number people improving in health outcomes
and determinants like poor health awareness
or lack of resources in tobacco prevention
(Mindell et al. 2010)
A significant impact is expected in regards to
total number of people affected and immediacy
of the impact
Our team consist of statistics and research
scholars to analyse the change in regards to
health outcomes
Data is mostly collected in the form of surveys
and interviews. It includes both quantitative
and qualitative data.
Potential Impact of HIA Findings
Is health already being
considered in the proposal or as part of
the decision-making process?
Are the links between the
proposal and health or health
determinants clear?
Is the decision-making process
open to the HIA and/or
recommendations for changes to
design, mitigations and/or alternatives?
If applied, would HIA findings and
recommendations potentially improve
the impact that the proposal has on
health
Health is already considered in proposal in the
decision-making process.
The proposal to prevent smoking in
Queensland is not directly related to health
outcomes. Decrease in tobacco smoking will
have positive impact on health but it is thee
long process and not immediate outcome of the
project.
Presently, the decision making is open to HIA
The other parameter will be taken care while
conducting the HIA
The proposal is not too closely related to
health. Also it is not too distantly related.
It is the physical intervention with long term
goal to engage locals in smoking prevention
habits and clinical interventions
magnitude, breadth and/or immediacy
of impacts?
Do evidence, expertise, and/or
research methods exist to analyze
health impacts of the decision?
improvement project where the initial target is
to reduce the adult smoking rate to 10% of the
population in that region currently.
It also aims to strengthen the mass media
campaign to quit smokers and reshap the social
norms related to the tobacco consumption
It may impact the health inequities by more
number people improving in health outcomes
and determinants like poor health awareness
or lack of resources in tobacco prevention
(Mindell et al. 2010)
A significant impact is expected in regards to
total number of people affected and immediacy
of the impact
Our team consist of statistics and research
scholars to analyse the change in regards to
health outcomes
Data is mostly collected in the form of surveys
and interviews. It includes both quantitative
and qualitative data.
Potential Impact of HIA Findings
Is health already being
considered in the proposal or as part of
the decision-making process?
Are the links between the
proposal and health or health
determinants clear?
Is the decision-making process
open to the HIA and/or
recommendations for changes to
design, mitigations and/or alternatives?
If applied, would HIA findings and
recommendations potentially improve
the impact that the proposal has on
health
Health is already considered in proposal in the
decision-making process.
The proposal to prevent smoking in
Queensland is not directly related to health
outcomes. Decrease in tobacco smoking will
have positive impact on health but it is thee
long process and not immediate outcome of the
project.
Presently, the decision making is open to HIA
The other parameter will be taken care while
conducting the HIA
The proposal is not too closely related to
health. Also it is not too distantly related.
It is the physical intervention with long term
goal to engage locals in smoking prevention
habits and clinical interventions
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3HEALTH IMPACT ASSESSMENT SCREENING
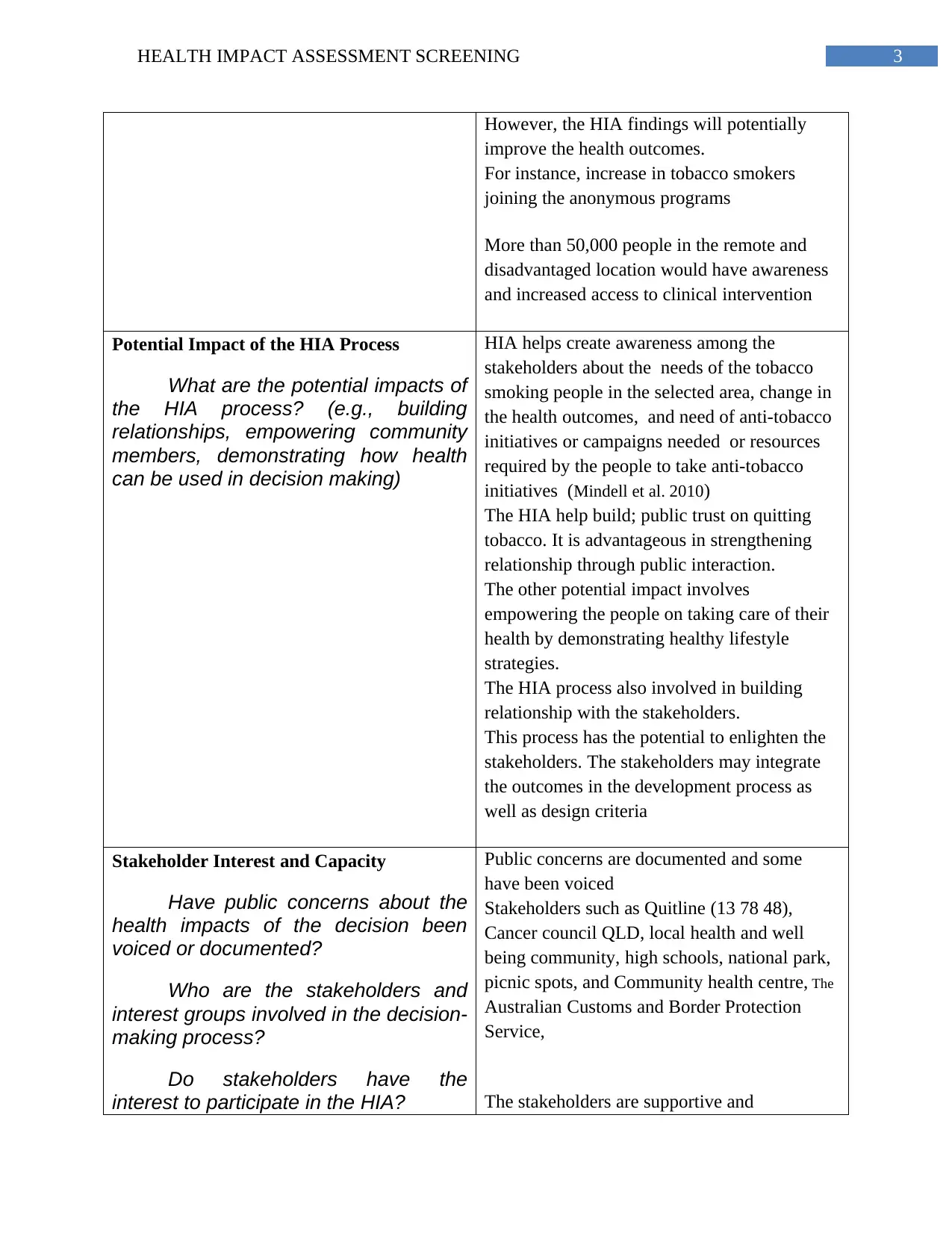
However, the HIA findings will potentially
improve the health outcomes.
For instance, increase in tobacco smokers
joining the anonymous programs
More than 50,000 people in the remote and
disadvantaged location would have awareness
and increased access to clinical intervention
Potential Impact of the HIA Process
What are the potential impacts of
the HIA process? (e.g., building
relationships, empowering community
members, demonstrating how health
can be used in decision making)
HIA helps create awareness among the
stakeholders about the needs of the tobacco
smoking people in the selected area, change in
the health outcomes, and need of anti-tobacco
initiatives or campaigns needed or resources
required by the people to take anti-tobacco
initiatives (Mindell et al. 2010)
The HIA help build; public trust on quitting
tobacco. It is advantageous in strengthening
relationship through public interaction.
The other potential impact involves
empowering the people on taking care of their
health by demonstrating healthy lifestyle
strategies.
The HIA process also involved in building
relationship with the stakeholders.
This process has the potential to enlighten the
stakeholders. The stakeholders may integrate
the outcomes in the development process as
well as design criteria
Stakeholder Interest and Capacity
Have public concerns about the
health impacts of the decision been
voiced or documented?
Who are the stakeholders and
interest groups involved in the decision-
making process?
Do stakeholders have the
interest to participate in the HIA?
Public concerns are documented and some
have been voiced
Stakeholders such as Quitline (13 78 48),
Cancer council QLD, local health and well
being community, high schools, national park,
picnic spots, and Community health centre, The
Australian Customs and Border Protection
Service,
The stakeholders are supportive and
However, the HIA findings will potentially
improve the health outcomes.
For instance, increase in tobacco smokers
joining the anonymous programs
More than 50,000 people in the remote and
disadvantaged location would have awareness
and increased access to clinical intervention
Potential Impact of the HIA Process
What are the potential impacts of
the HIA process? (e.g., building
relationships, empowering community
members, demonstrating how health
can be used in decision making)
HIA helps create awareness among the
stakeholders about the needs of the tobacco
smoking people in the selected area, change in
the health outcomes, and need of anti-tobacco
initiatives or campaigns needed or resources
required by the people to take anti-tobacco
initiatives (Mindell et al. 2010)
The HIA help build; public trust on quitting
tobacco. It is advantageous in strengthening
relationship through public interaction.
The other potential impact involves
empowering the people on taking care of their
health by demonstrating healthy lifestyle
strategies.
The HIA process also involved in building
relationship with the stakeholders.
This process has the potential to enlighten the
stakeholders. The stakeholders may integrate
the outcomes in the development process as
well as design criteria
Stakeholder Interest and Capacity
Have public concerns about the
health impacts of the decision been
voiced or documented?
Who are the stakeholders and
interest groups involved in the decision-
making process?
Do stakeholders have the
interest to participate in the HIA?
Public concerns are documented and some
have been voiced
Stakeholders such as Quitline (13 78 48),
Cancer council QLD, local health and well
being community, high schools, national park,
picnic spots, and Community health centre, The
Australian Customs and Border Protection
Service,
The stakeholders are supportive and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4HEALTH IMPACT ASSESSMENT SCREENING
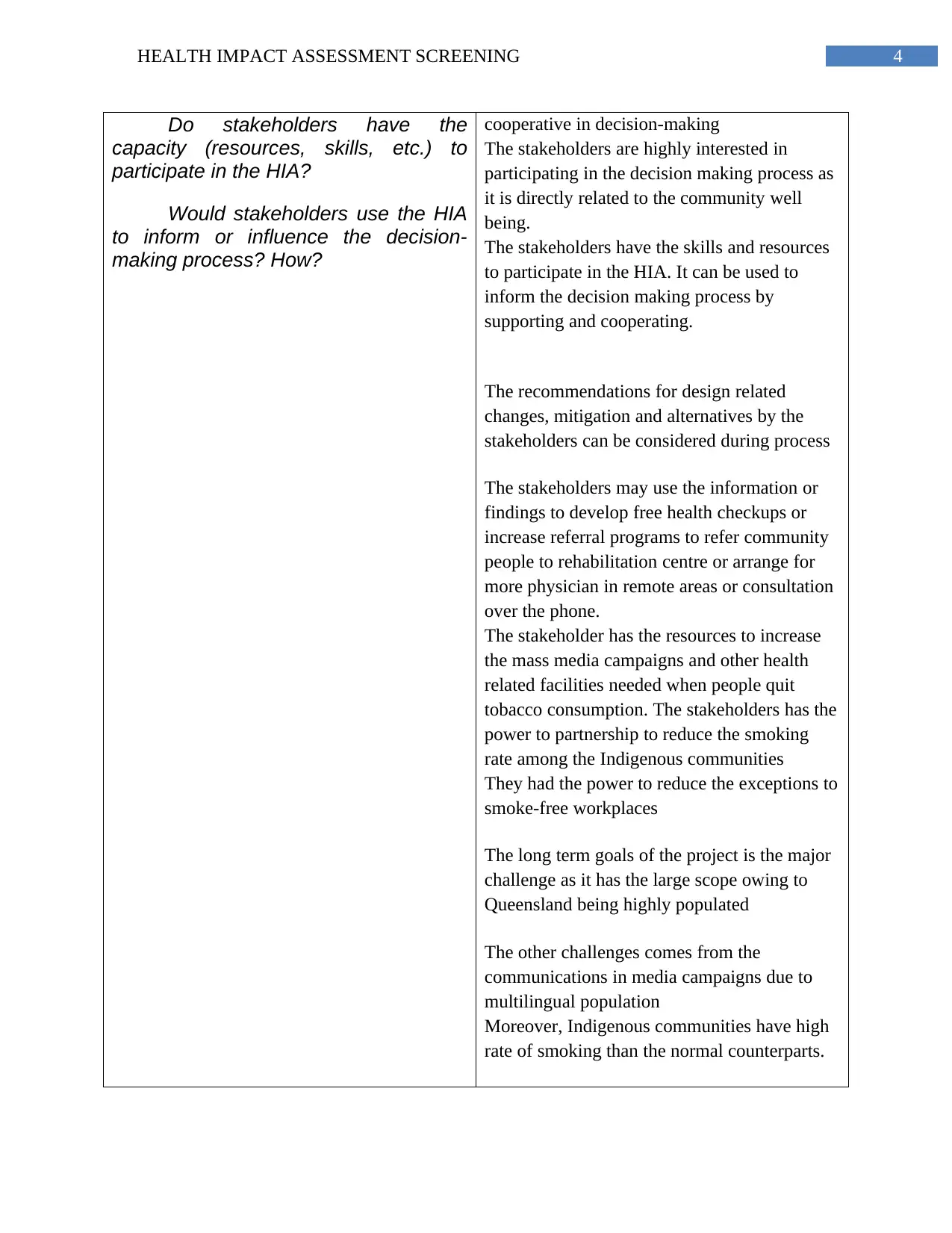
Do stakeholders have the
capacity (resources, skills, etc.) to
participate in the HIA?
Would stakeholders use the HIA
to inform or influence the decision-
making process? How?
cooperative in decision-making
The stakeholders are highly interested in
participating in the decision making process as
it is directly related to the community well
being.
The stakeholders have the skills and resources
to participate in the HIA. It can be used to
inform the decision making process by
supporting and cooperating.
The recommendations for design related
changes, mitigation and alternatives by the
stakeholders can be considered during process
The stakeholders may use the information or
findings to develop free health checkups or
increase referral programs to refer community
people to rehabilitation centre or arrange for
more physician in remote areas or consultation
over the phone.
The stakeholder has the resources to increase
the mass media campaigns and other health
related facilities needed when people quit
tobacco consumption. The stakeholders has the
power to partnership to reduce the smoking
rate among the Indigenous communities
They had the power to reduce the exceptions to
smoke-free workplaces
The long term goals of the project is the major
challenge as it has the large scope owing to
Queensland being highly populated
The other challenges comes from the
communications in media campaigns due to
multilingual population
Moreover, Indigenous communities have high
rate of smoking than the normal counterparts.
Do stakeholders have the
capacity (resources, skills, etc.) to
participate in the HIA?
Would stakeholders use the HIA
to inform or influence the decision-
making process? How?
cooperative in decision-making
The stakeholders are highly interested in
participating in the decision making process as
it is directly related to the community well
being.
The stakeholders have the skills and resources
to participate in the HIA. It can be used to
inform the decision making process by
supporting and cooperating.
The recommendations for design related
changes, mitigation and alternatives by the
stakeholders can be considered during process
The stakeholders may use the information or
findings to develop free health checkups or
increase referral programs to refer community
people to rehabilitation centre or arrange for
more physician in remote areas or consultation
over the phone.
The stakeholder has the resources to increase
the mass media campaigns and other health
related facilities needed when people quit
tobacco consumption. The stakeholders has the
power to partnership to reduce the smoking
rate among the Indigenous communities
They had the power to reduce the exceptions to
smoke-free workplaces
The long term goals of the project is the major
challenge as it has the large scope owing to
Queensland being highly populated
The other challenges comes from the
communications in media campaigns due to
multilingual population
Moreover, Indigenous communities have high
rate of smoking than the normal counterparts.
5HEALTH IMPACT ASSESSMENT SCREENING
2. Refelctive report
The rationale for the HIA was to recognise the needs of the people in the community in
the process of quitting the tobacco consumption and deliver appropriate strategies that can help
to prevent the tobacco smoking. Doing the HIA would have helped me understanding the public
needs in accessing the tobacco prevention facilities by both the remote and the urban areas in
Queensland. Considering the increasing death and disability rate in Australia due to smoking-
related illness, the aim of HIA is justified.
My initial assumptions were getting clear statistics on the public perception regarding the
process and obstacles in quitting tobacco. I assumed gaining plenty of information on the need of
the facilities required by the people, rehabilitation program and need of the other clinical
interventions to quit tobacco smoking. I assumed a low percentage of people to be aware of the
smoking consequences. I expected high need of attending counselling sessions or prevention
sessions.
The data obtained from screening was surprising. More number of people than I assumed
had the good awareness of the smoking consequences. However, the same was not the case of
people in the remote and disadvantaged areas. It was due to lack of education and poor access to
health facilities. More people in urban than in remote areas were ready for interventions and
discussed their barriers in accessing the public health service in this regard. HIA would have
impact on the number of people involved in smoking. It will eliminate the determinants like poor
access to tobacco smoking interventions. People were responsive than before. They were
proficient in explaining the health outcomes as a result of the smoking interventions accessed by
them. The stakeholder was more cooperative and enthusiastic than I had assumed. It was easy for
me to gain the public trust and bond with them. They were attentive to me when discussing about
2. Refelctive report
The rationale for the HIA was to recognise the needs of the people in the community in
the process of quitting the tobacco consumption and deliver appropriate strategies that can help
to prevent the tobacco smoking. Doing the HIA would have helped me understanding the public
needs in accessing the tobacco prevention facilities by both the remote and the urban areas in
Queensland. Considering the increasing death and disability rate in Australia due to smoking-
related illness, the aim of HIA is justified.
My initial assumptions were getting clear statistics on the public perception regarding the
process and obstacles in quitting tobacco. I assumed gaining plenty of information on the need of
the facilities required by the people, rehabilitation program and need of the other clinical
interventions to quit tobacco smoking. I assumed a low percentage of people to be aware of the
smoking consequences. I expected high need of attending counselling sessions or prevention
sessions.
The data obtained from screening was surprising. More number of people than I assumed
had the good awareness of the smoking consequences. However, the same was not the case of
people in the remote and disadvantaged areas. It was due to lack of education and poor access to
health facilities. More people in urban than in remote areas were ready for interventions and
discussed their barriers in accessing the public health service in this regard. HIA would have
impact on the number of people involved in smoking. It will eliminate the determinants like poor
access to tobacco smoking interventions. People were responsive than before. They were
proficient in explaining the health outcomes as a result of the smoking interventions accessed by
them. The stakeholder was more cooperative and enthusiastic than I had assumed. It was easy for
me to gain the public trust and bond with them. They were attentive to me when discussing about
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6HEALTH IMPACT ASSESSMENT SCREENING
the referral programs. Most of the people also gave the evidence of quitting tobacco smoking.
Parents were trying to protect the children from second hand smoke in their house. There were
some people who have completely quit smoking and were experiencing the health outcomes such
as improvement in asthma symptoms, and lung perforations.
The factors that influenced my screening and scoping are the cooperation and interest of
the stakeholder. They were open in communication and accepted my ideas and viewpoints.
Awareness and responsiveness of the public was the factor that made HIA a quick process. The
other parameter that was an added advantage is the use of existing tobacco control policy and
framework.
Screening and scooping was influenced by the support from the stakeholders and
knowledge of the people in Queensland. It was easy to communicate with the people in urban
areas, However, the same was difficult when dealing with people in remote areas. Lack of skills
in dealing with the multilingual population was a bigger challenge. Lack of awareness and
impact of the HIA on health outcomes was a barrier that delayed the process. Other barriers were
housing, transport, economic conditions and education. There is a need of better framework in
integrating the different types of research evidence in decision making (Hyland et al. 2016).
The tight timescales has made the review of the HIA evidence difficult. Further, different
stakeholders, need to make recommendations for them, lack of specific expertise in remote areas,
diversity of the health impacts and complex casual pathways, and at times difficulty conducting
high quality HIA were also barriers.
Given an opportunity to advice someone else who was about to undertake the screening
and scoping steps of a HIA, I would recommend them to public health centres and community
the referral programs. Most of the people also gave the evidence of quitting tobacco smoking.
Parents were trying to protect the children from second hand smoke in their house. There were
some people who have completely quit smoking and were experiencing the health outcomes such
as improvement in asthma symptoms, and lung perforations.
The factors that influenced my screening and scoping are the cooperation and interest of
the stakeholder. They were open in communication and accepted my ideas and viewpoints.
Awareness and responsiveness of the public was the factor that made HIA a quick process. The
other parameter that was an added advantage is the use of existing tobacco control policy and
framework.
Screening and scooping was influenced by the support from the stakeholders and
knowledge of the people in Queensland. It was easy to communicate with the people in urban
areas, However, the same was difficult when dealing with people in remote areas. Lack of skills
in dealing with the multilingual population was a bigger challenge. Lack of awareness and
impact of the HIA on health outcomes was a barrier that delayed the process. Other barriers were
housing, transport, economic conditions and education. There is a need of better framework in
integrating the different types of research evidence in decision making (Hyland et al. 2016).
The tight timescales has made the review of the HIA evidence difficult. Further, different
stakeholders, need to make recommendations for them, lack of specific expertise in remote areas,
diversity of the health impacts and complex casual pathways, and at times difficulty conducting
high quality HIA were also barriers.
Given an opportunity to advice someone else who was about to undertake the screening
and scoping steps of a HIA, I would recommend them to public health centres and community
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7HEALTH IMPACT ASSESSMENT SCREENING
care centres. I would suggest them to evidence based cessation services to support smokers to
quit.
It can be concluded that the HIA is an important tool to inform the decision making by
policy makers. Although it may be subjected to criticism for lacking the use of evidence in
decision-making, it is useful in influencing the health outcomes. Policy making is required as the
individual’s health is influenced by range of factors. HIA is important in gaining better
information on public health and develop appropriate strategies. I agree that policies have
significant impact on the public health. HIA helps improving the health care provision. I have
learned that HIA has the potential to change the health determinants. Screening and scoping are
practical approach to identify the positive and negative impact of health proposal. This flexible
approach is effective in maximising the health gain opportunities. Overall, my knowledge in this
subject has enhanced.
care centres. I would suggest them to evidence based cessation services to support smokers to
quit.
It can be concluded that the HIA is an important tool to inform the decision making by
policy makers. Although it may be subjected to criticism for lacking the use of evidence in
decision-making, it is useful in influencing the health outcomes. Policy making is required as the
individual’s health is influenced by range of factors. HIA is important in gaining better
information on public health and develop appropriate strategies. I agree that policies have
significant impact on the public health. HIA helps improving the health care provision. I have
learned that HIA has the potential to change the health determinants. Screening and scoping are
practical approach to identify the positive and negative impact of health proposal. This flexible
approach is effective in maximising the health gain opportunities. Overall, my knowledge in this
subject has enhanced.
8HEALTH IMPACT ASSESSMENT SCREENING
References
Hyland, A., Ambrose, B.K., Conway, K.P., Borek, N., Lambert, E., Carusi, C., Taylor, K.,
Crosse, S., Fong, G.T., Cummings, K.M. and Abrams, D., 2016. Design and methods of the
Population Assessment of Tobacco and Health (PATH) Study. Tobacco control,
pp.tobaccocontrol-2016.
Leung, J., Gartner, C., Hall, W., Lucke, J. and Dobson, A., 2012. A longitudinal study of the bi-
directional relationship between tobacco smoking and psychological distress in a community
sample of young Australian women. Psychological medicine, 42(6), pp.1273-1282.
Mindell, J., Biddulph, J., Taylor, L., Lock, K., Boaz, A., Joffe, M. and Curtis, S., 2010.
Improving the use of evidence in health impact assessment. Bulletin of the World Health
Organization, 88(7), pp.543-550.
www.nationaldrugstrategy.gov.au. 2018. National Tobacco Strategy 2012–2018. [online]
Available at: https://campaigns.health.gov.au/drughelp/resources/publications/report/national-
tobacco-strategy-2012 [Accessed 3 Feb. 2018].
References
Hyland, A., Ambrose, B.K., Conway, K.P., Borek, N., Lambert, E., Carusi, C., Taylor, K.,
Crosse, S., Fong, G.T., Cummings, K.M. and Abrams, D., 2016. Design and methods of the
Population Assessment of Tobacco and Health (PATH) Study. Tobacco control,
pp.tobaccocontrol-2016.
Leung, J., Gartner, C., Hall, W., Lucke, J. and Dobson, A., 2012. A longitudinal study of the bi-
directional relationship between tobacco smoking and psychological distress in a community
sample of young Australian women. Psychological medicine, 42(6), pp.1273-1282.
Mindell, J., Biddulph, J., Taylor, L., Lock, K., Boaz, A., Joffe, M. and Curtis, S., 2010.
Improving the use of evidence in health impact assessment. Bulletin of the World Health
Organization, 88(7), pp.543-550.
www.nationaldrugstrategy.gov.au. 2018. National Tobacco Strategy 2012–2018. [online]
Available at: https://campaigns.health.gov.au/drughelp/resources/publications/report/national-
tobacco-strategy-2012 [Accessed 3 Feb. 2018].
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.