Examining Hierarchy & Power Dynamics in Australian Healthcare System
VerifiedAdded on 2023/06/04
|14
|3031
|166
Essay
AI Summary
This essay provides a comprehensive overview of the Australian healthcare system, highlighting its hierarchical structure and the power dynamics inherent within it. It discusses the roles of various medical professionals, from senior medical officers to resident medical officers, and examines how power imbalances can affect the quality of care. The essay also explores sociological theories relevant to public health, such as the unintended consequences of social interventions and the social construction of reality, and analyzes their impact on the Australian healthcare system. Furthermore, it addresses the challenges of maintaining autonomy and power within the system, the need for interprofessional collaboration, and the importance of considering social factors in healthcare delivery. The essay concludes by emphasizing the need for inclusivity and quality care for all patients within the Australian healthcare framework.

Healthcare system in Australia
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Contents
Introduction.................................................................................................................................................2
Overview of healthcare system of Australia................................................................................................3
Hierarchy of the Australian healthcare system............................................................................................4
Senior Medical officers............................................................................................................................5
Visiting medical officers.........................................................................................................................6
Registrars.................................................................................................................................................6
Principal house officer.............................................................................................................................6
Resident medical officers........................................................................................................................6
Power in the healthcare system of Australia................................................................................................7
Sociological theories of public health..........................................................................................................8
Impact of these developments...................................................................................................................10
Conclusion.................................................................................................................................................11
References.................................................................................................................................................12
Introduction.................................................................................................................................................2
Overview of healthcare system of Australia................................................................................................3
Hierarchy of the Australian healthcare system............................................................................................4
Senior Medical officers............................................................................................................................5
Visiting medical officers.........................................................................................................................6
Registrars.................................................................................................................................................6
Principal house officer.............................................................................................................................6
Resident medical officers........................................................................................................................6
Power in the healthcare system of Australia................................................................................................7
Sociological theories of public health..........................................................................................................8
Impact of these developments...................................................................................................................10
Conclusion.................................................................................................................................................11
References.................................................................................................................................................12
Introduction
The healthcare system of Australia has passed through different stages after the colonial era.
Currently, the Australian healthcare system is divided into different tiers. There are not only
medical practitioners but also administrative officers. These officers take decisions according to
the need. This system has till now worked well and the healthcare system in Australia is
considered as one of the best healthcare systems of the world. Australia exports the medical
services to many countries of the world. There are some key findings like Australia spend 9.5%
of its GDP on public health. This is lower than many OECD countries especially the USA but a
considerable amount is spent on health (Brien, 2017).
Despite this, there is a section of the population in Australia which remains deprived of
healthcare facilities because of excessive cost. The government interventions like Medicare has
benefited the population but the healthcare services have not reached every stratum of the
population. There are aborigines who cannot access health services because of economic reasons.
Nurses are present in remote areas but doctors and specialists are practice only in cities. This
essay addresses various salient features of the healthcare system of Australia. This aims to
critically evaluate the statement that hierarchy and power are intrinsic to the health care system
of Australia. The essay also considers sociological theories in the context of the healthcare
system. The health care services are provided in Australia by the public as well as private sector.
Overview of healthcare system of Australia
The healthcare system of Australia is an established and successful system though some lacunae
are there like lack of doctors for countryside population. In addition to this, the public hospitals
The healthcare system of Australia has passed through different stages after the colonial era.
Currently, the Australian healthcare system is divided into different tiers. There are not only
medical practitioners but also administrative officers. These officers take decisions according to
the need. This system has till now worked well and the healthcare system in Australia is
considered as one of the best healthcare systems of the world. Australia exports the medical
services to many countries of the world. There are some key findings like Australia spend 9.5%
of its GDP on public health. This is lower than many OECD countries especially the USA but a
considerable amount is spent on health (Brien, 2017).
Despite this, there is a section of the population in Australia which remains deprived of
healthcare facilities because of excessive cost. The government interventions like Medicare has
benefited the population but the healthcare services have not reached every stratum of the
population. There are aborigines who cannot access health services because of economic reasons.
Nurses are present in remote areas but doctors and specialists are practice only in cities. This
essay addresses various salient features of the healthcare system of Australia. This aims to
critically evaluate the statement that hierarchy and power are intrinsic to the health care system
of Australia. The essay also considers sociological theories in the context of the healthcare
system. The health care services are provided in Australia by the public as well as private sector.
Overview of healthcare system of Australia
The healthcare system of Australia is an established and successful system though some lacunae
are there like lack of doctors for countryside population. In addition to this, the public hospitals
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
are flooded with patients so the person has to wait for long in the queue to get treatment from
public hospital doctors. The healthcare system of Australia provides many kind of services, it
provides population helath as well as prevention measures. In addition to this, this system
provides emergency treatment and hospital acre. Rehabilitation and palliative care is part of
Australian health system (Wardle et al., 2017).
The first point of call for most people is the primary health care (Robards, 2018). It is delivered
at home, general practices centers and community health system. Australia has allied health
professionals also; they are not doctors, dentist or nurses but they are trained as medical
practitioners. Primary health care can be provided by doctors, dentists, nurses and even allied
health professionals. In addition to this, Australia has after-hour general practitioners which
provide the special services to the patients. They can visit the home of the patient and in some
cases, this service is covered by the government’s ambitious program Medicare ( Malik et al.
2018). The urgent or emergency cases are treated by the emergency department; rest services can
be provided by general practitioners. Emergency departments are mostly located at public
hospital of Australia. Then, there are specialists who can work in private as well as public
hospitals and they are specialized in the particular field.
Hierarchy of the Australian healthcare system
Australia has a strict hierarchical structure to give the best services to patients. Because of this
structure, Australia is considered one of the best places in terms of healthcare assistance. The
hospitals are governed by the commonwealth as well as state or territory governments (wiskar,
2013). The particular hospital has to abide by all the relevant rules and regulations formed by the
public hospital doctors. The healthcare system of Australia provides many kind of services, it
provides population helath as well as prevention measures. In addition to this, this system
provides emergency treatment and hospital acre. Rehabilitation and palliative care is part of
Australian health system (Wardle et al., 2017).
The first point of call for most people is the primary health care (Robards, 2018). It is delivered
at home, general practices centers and community health system. Australia has allied health
professionals also; they are not doctors, dentist or nurses but they are trained as medical
practitioners. Primary health care can be provided by doctors, dentists, nurses and even allied
health professionals. In addition to this, Australia has after-hour general practitioners which
provide the special services to the patients. They can visit the home of the patient and in some
cases, this service is covered by the government’s ambitious program Medicare ( Malik et al.
2018). The urgent or emergency cases are treated by the emergency department; rest services can
be provided by general practitioners. Emergency departments are mostly located at public
hospital of Australia. Then, there are specialists who can work in private as well as public
hospitals and they are specialized in the particular field.
Hierarchy of the Australian healthcare system
Australia has a strict hierarchical structure to give the best services to patients. Because of this
structure, Australia is considered one of the best places in terms of healthcare assistance. The
hospitals are governed by the commonwealth as well as state or territory governments (wiskar,
2013). The particular hospital has to abide by all the relevant rules and regulations formed by the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
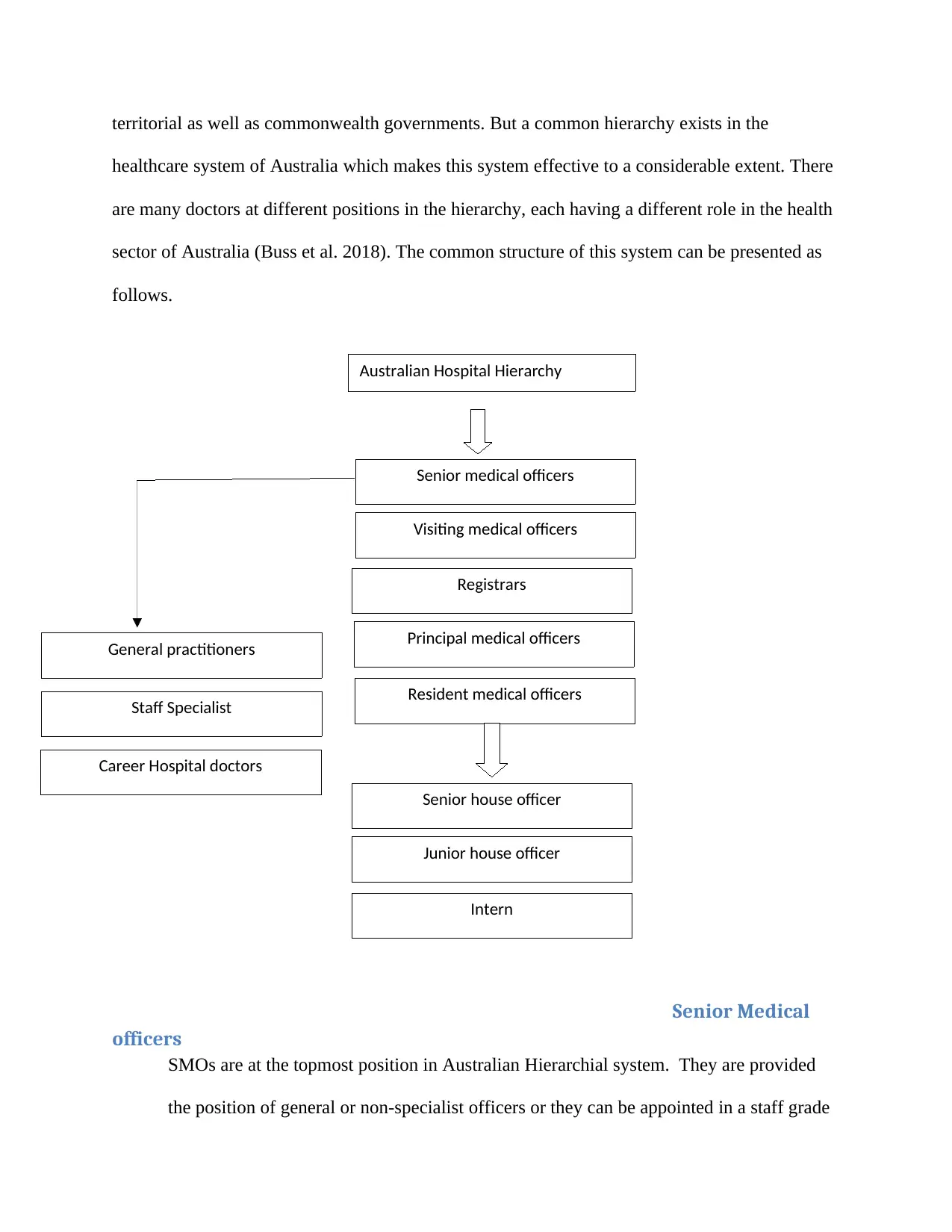
territorial as well as commonwealth governments. But a common hierarchy exists in the
healthcare system of Australia which makes this system effective to a considerable extent. There
are many doctors at different positions in the hierarchy, each having a different role in the health
sector of Australia (Buss et al. 2018). The common structure of this system can be presented as
follows.
Senior Medical
officers
SMOs are at the topmost position in Australian Hierarchial system. They are provided
the position of general or non-specialist officers or they can be appointed in a staff grade
Australian Hospital Hierarchy
Principal medical officers
Resident medical officers
Registrars
Visiting medical officers
Senior medical officers
Junior house officer
Intern
Career Hospital doctors
Staff Specialist
General practitioners
Senior house officer
healthcare system of Australia which makes this system effective to a considerable extent. There
are many doctors at different positions in the hierarchy, each having a different role in the health
sector of Australia (Buss et al. 2018). The common structure of this system can be presented as
follows.
Senior Medical
officers
SMOs are at the topmost position in Australian Hierarchial system. They are provided
the position of general or non-specialist officers or they can be appointed in a staff grade
Australian Hospital Hierarchy
Principal medical officers
Resident medical officers
Registrars
Visiting medical officers
Senior medical officers
Junior house officer
Intern
Career Hospital doctors
Staff Specialist
General practitioners
Senior house officer
positions. Non-specialist officers need not be qualified; they work under the senior
specialist. Whereas the SMOs who work at the position of staff grade are qualified
(Delaney, 2018). It has 3 subdivisions namely, visiting medical officers, staff specialists,
and career hospital doctors.
Visiting medical officers
These are known as general practitioners. They have their own private set up and work at
public or private hospitals on a part-time basis.
Registrars
These doctors are accepted at an accredited specialist training program at the nominated
college.
Principal house officer
This is the next level in the Australian healthcare system. PHOs are basically students
who are in the 4th year of their post-graduation course but given some responsibility to
treat patients (LiLi, 2017). They are equal to registrars as far as their position is
concerned.
Resident medical officers
It further has three subdivisions:
specialist. Whereas the SMOs who work at the position of staff grade are qualified
(Delaney, 2018). It has 3 subdivisions namely, visiting medical officers, staff specialists,
and career hospital doctors.
Visiting medical officers
These are known as general practitioners. They have their own private set up and work at
public or private hospitals on a part-time basis.
Registrars
These doctors are accepted at an accredited specialist training program at the nominated
college.
Principal house officer
This is the next level in the Australian healthcare system. PHOs are basically students
who are in the 4th year of their post-graduation course but given some responsibility to
treat patients (LiLi, 2017). They are equal to registrars as far as their position is
concerned.
Resident medical officers
It further has three subdivisions:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
a)Senior house officer
SHO is inferior in the hierarchy. Those who are not appointed as registrars or PHOs are
included in this category. They are generally 3rd-year students.
b) Junior house officer
These are 2nd-year students who are quite away from becoming registrar or PHOs.
c) Intern
The first year students of post-graduation are considered as interns. They are not given
any responsibility to treat the patients. They are mere observers; they observe the
treatment of patients, learn it and make reports.
Power in the healthcare system of Australia
Based upon the findings of a case study, three themes are there with respect to power
dynamics: (a) tendency to protect autonomy by the use of power (b) power dynamics
between public and private health services provider (c) reduced consultation to maintain
hegemony or influence of power. It is observed that the CDM program was started by the
government to increase inclusion in the decision-making process. But the results are
disappointing. Still, in Australian hospitals, the doctors of particular position tend to
maintain their autonomy and do not seek consultation from colleagues to maintain their
power (Seah et al., 2012). General practitioners seldom try to engage with allied health
professionals. The interaction between inter-organizational, interprofessional and intra-
professional relationships is revealed by a case study of similar kind which was done on
SHO is inferior in the hierarchy. Those who are not appointed as registrars or PHOs are
included in this category. They are generally 3rd-year students.
b) Junior house officer
These are 2nd-year students who are quite away from becoming registrar or PHOs.
c) Intern
The first year students of post-graduation are considered as interns. They are not given
any responsibility to treat the patients. They are mere observers; they observe the
treatment of patients, learn it and make reports.
Power in the healthcare system of Australia
Based upon the findings of a case study, three themes are there with respect to power
dynamics: (a) tendency to protect autonomy by the use of power (b) power dynamics
between public and private health services provider (c) reduced consultation to maintain
hegemony or influence of power. It is observed that the CDM program was started by the
government to increase inclusion in the decision-making process. But the results are
disappointing. Still, in Australian hospitals, the doctors of particular position tend to
maintain their autonomy and do not seek consultation from colleagues to maintain their
power (Seah et al., 2012). General practitioners seldom try to engage with allied health
professionals. The interaction between inter-organizational, interprofessional and intra-
professional relationships is revealed by a case study of similar kind which was done on
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
health care networks. These are attributed to balance of power shifts like shift in
professional heirachies and power relations followed by tradition which is also known as
dark side of interprofessional relationship.
These developments have a negative effect on the healthcare system as a whole. Till now,
the attention has been concentrated on the private sector, there is need to go beyond that
and reform the public healthcare system as well. Power dynamics affect day to day
functions of the hospital. The power dynamics affect the choice of professional whether
to seek consultation or collaborate, to whom and when. Two theories must be considered
here: one is the resource dependency and another one on transactional cost analysis.
These theories point towards the integrated approach instead of treating the patient in
isolation or alone (Charlesworth et al., 2015) or these theories point at an integrated
approach to provide quality health services. Interprofessional collaboration is must to
provide quality care to the patients. Australia lacks in this aspect. It has very less
collaboration among professional doctors. General practitioners resist shared decision
making with allied professionals and other relevant authorities that result in the resistance
of the incursion of GPs in their areas. This all is done to maintain the power structure.
Sociological theories of public health
There has been a lack of searches related to global health which contains the health-
related education. But 4 sociological theories have a direct relationship with the health of
the community (Robinson et al., 2013) The first theory was given by Robert Merton. This
theory emphasizes that all social interventions have more or less unintended
consequences. Some of these consequences can be predicted and prevented but some
professional heirachies and power relations followed by tradition which is also known as
dark side of interprofessional relationship.
These developments have a negative effect on the healthcare system as a whole. Till now,
the attention has been concentrated on the private sector, there is need to go beyond that
and reform the public healthcare system as well. Power dynamics affect day to day
functions of the hospital. The power dynamics affect the choice of professional whether
to seek consultation or collaborate, to whom and when. Two theories must be considered
here: one is the resource dependency and another one on transactional cost analysis.
These theories point towards the integrated approach instead of treating the patient in
isolation or alone (Charlesworth et al., 2015) or these theories point at an integrated
approach to provide quality health services. Interprofessional collaboration is must to
provide quality care to the patients. Australia lacks in this aspect. It has very less
collaboration among professional doctors. General practitioners resist shared decision
making with allied professionals and other relevant authorities that result in the resistance
of the incursion of GPs in their areas. This all is done to maintain the power structure.
Sociological theories of public health
There has been a lack of searches related to global health which contains the health-
related education. But 4 sociological theories have a direct relationship with the health of
the community (Robinson et al., 2013) The first theory was given by Robert Merton. This
theory emphasizes that all social interventions have more or less unintended
consequences. Some of these consequences can be predicted and prevented but some
may take dangerous forms as they cannot be predicted easily. Therefore, this theory
suggests assessing the consequences of each social programme beforehand; in severe
cases, the end result can be the termination of the program itself. To prevent such
situation, predict the consequences well in advance and prevent that from taking monster
form. There have been many examples of turning a program into unintended
consequences, such as after application of coercive action in India to treat small pox, the
Indian population turned hostile to every kind of vaccination campaigns. Another
example is one child policy of China which led to an unintended consequence of the
sexual revolution (MacIntyre, 2011).
The second theory, known as the social construction of reality was given by Peter Burger
and Thomas Luckmann in the 1960s. According to this theory the real world is
influenced by social and cultural ideas and other things without any relevance to material
base. The examples of this aspect can be provided by the spread of H1N1 influenza,
stigmatization of mental disease in The Republic of China. Another example is the social
rejection of abortion in the USA while abortions are considered safe in Japan. So the
health programs can be against the cultural norms of the particular locality like village,
neighborhood, hospital etc. This theory emphasizes that these cultural values have the
effect on each kind of medical development like smoking cessation and AIDS prevention.
The third theory has four implications for the healthcare system. First, that political and
economic forces in society can lead to disease, for example in case of abject poverty,
Tuberculosis flourishes rapidly and resistant variants of pathogen related to tuberculosis,
develops (Armstrong et al., 2007). The Second implication is that sociopolitical
institutions like health care bureaucracies can give unintended out comes and lead to
suggests assessing the consequences of each social programme beforehand; in severe
cases, the end result can be the termination of the program itself. To prevent such
situation, predict the consequences well in advance and prevent that from taking monster
form. There have been many examples of turning a program into unintended
consequences, such as after application of coercive action in India to treat small pox, the
Indian population turned hostile to every kind of vaccination campaigns. Another
example is one child policy of China which led to an unintended consequence of the
sexual revolution (MacIntyre, 2011).
The second theory, known as the social construction of reality was given by Peter Burger
and Thomas Luckmann in the 1960s. According to this theory the real world is
influenced by social and cultural ideas and other things without any relevance to material
base. The examples of this aspect can be provided by the spread of H1N1 influenza,
stigmatization of mental disease in The Republic of China. Another example is the social
rejection of abortion in the USA while abortions are considered safe in Japan. So the
health programs can be against the cultural norms of the particular locality like village,
neighborhood, hospital etc. This theory emphasizes that these cultural values have the
effect on each kind of medical development like smoking cessation and AIDS prevention.
The third theory has four implications for the healthcare system. First, that political and
economic forces in society can lead to disease, for example in case of abject poverty,
Tuberculosis flourishes rapidly and resistant variants of pathogen related to tuberculosis,
develops (Armstrong et al., 2007). The Second implication is that sociopolitical
institutions like health care bureaucracies can give unintended out comes and lead to
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
further suffering to patient, rather than treatment. For example, US veterans
administration clinics failed to diagnose and treat the clinical problem (psychiatric
trauma) among the US soldiers who run a long battle in Iraq and Afghanistan.
The third implication is that social suffering is not limited to an individual or patient, but
it has wider repercussions; other associated persons also experience discomfort due to a
particular disease of the patient (Nicholson, 2012). For example, in severe cases of
Alzheimer’s disease, the patient is not able to feel pain but adult children may suffer from
pain and other related problems to disease. Then, there is the theory of social suffering
which implies the removal of distinction between health problem and social problem.
These problems require health as well as social solutions like in the cases of poverty and
violence, the patient are provided social care along with the treatment of physical injury
e.g. depression, post traumatic stress disorder etc.
Fourth social theory draws attention to the concept of biopower. This term ‘biopower’
was coined by Michel Foucault (Makridis, 2011). This theory emphasizes the effect of
political governance on social institutions including health. The big example of China
substantiates this claim; in 1960s and1970s, under the influence of Maoist government, it
was made compulsory for every woman to place the date of her menstrual cycle on the
doors of their home for the purpose of surveillance and birth control. These four theories
show light on the global health system. Australian healthcare system is not indifferent to
these sociological theories; it also gets affected and influenced according to exigencies of
time (Hall, 2015).
administration clinics failed to diagnose and treat the clinical problem (psychiatric
trauma) among the US soldiers who run a long battle in Iraq and Afghanistan.
The third implication is that social suffering is not limited to an individual or patient, but
it has wider repercussions; other associated persons also experience discomfort due to a
particular disease of the patient (Nicholson, 2012). For example, in severe cases of
Alzheimer’s disease, the patient is not able to feel pain but adult children may suffer from
pain and other related problems to disease. Then, there is the theory of social suffering
which implies the removal of distinction between health problem and social problem.
These problems require health as well as social solutions like in the cases of poverty and
violence, the patient are provided social care along with the treatment of physical injury
e.g. depression, post traumatic stress disorder etc.
Fourth social theory draws attention to the concept of biopower. This term ‘biopower’
was coined by Michel Foucault (Makridis, 2011). This theory emphasizes the effect of
political governance on social institutions including health. The big example of China
substantiates this claim; in 1960s and1970s, under the influence of Maoist government, it
was made compulsory for every woman to place the date of her menstrual cycle on the
doors of their home for the purpose of surveillance and birth control. These four theories
show light on the global health system. Australian healthcare system is not indifferent to
these sociological theories; it also gets affected and influenced according to exigencies of
time (Hall, 2015).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Impact of these developments
As a health practitioner, these attributes affect me also. To maintain autonomy and
power, professional does not consult anyone. This leads to the narrow decision-making
process (J, 2015). There is no inclusivity and quality care of the patient. Interprofessional
consultation has many other benefits. It has been proven by a study that hospitals or
clinics in which interprofessional consultation is widely used, tend to attract more
patients. The examples of the relation of global health with the sociological theories have
already been provided. as an individual of society, I also get affected by these
percussions.
Conclusion
From the above-provided information, it can be concluded that power and hierarchy are
intrinsic to the current healthcare system of Australia (Dixit and Sambasivan, 2018).
Power dynamics prevent interprofessional consultation and adequate research into the
depth of disease. In addition to this, the sociological theories are discussed in the context
of global health. There is a need to remove these lacunae from the healthcare system and
try to make doctors' assistance accessible for aborigines also.
As a health practitioner, these attributes affect me also. To maintain autonomy and
power, professional does not consult anyone. This leads to the narrow decision-making
process (J, 2015). There is no inclusivity and quality care of the patient. Interprofessional
consultation has many other benefits. It has been proven by a study that hospitals or
clinics in which interprofessional consultation is widely used, tend to attract more
patients. The examples of the relation of global health with the sociological theories have
already been provided. as an individual of society, I also get affected by these
percussions.
Conclusion
From the above-provided information, it can be concluded that power and hierarchy are
intrinsic to the current healthcare system of Australia (Dixit and Sambasivan, 2018).
Power dynamics prevent interprofessional consultation and adequate research into the
depth of disease. In addition to this, the sociological theories are discussed in the context
of global health. There is a need to remove these lacunae from the healthcare system and
try to make doctors' assistance accessible for aborigines also.
References
Arunima Malik, Prof Manfrod Lenzen, Scott McAlister & Forbes McGain (2018). The carbon footprint of
Australian health care. The Lancet, 112-124. Retrieved from
https://www.thelancet.com/journals/lanplh/article/PIIS2542-5196(17)30180-8/fulltext
Bruce K Armstrong, James A Gillespie, Stephen R Leeder, george L rubin & Lesley M Rusell. (2007).
Challenges in health and health care for Australia. Medical Journal of Australia, 23-34. Retrieved
from https://www.mja.com.au/journal/2007/187/9/challenges-health-and-health-care-australia
Caroline Nicholson, Jackson C L, Marley J &Wells R. (2012). The Australian Experiment: How Primary
Health Care Organizations Supported the Evolution of a Primary Health Care System. Journal of
the American Board of Family Income, 32-35. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/22403246
Davinia S. E. Seah, T. Z. Cheong, Matthew & H. R. Anstey (2012). The hidden cost of private health
insurance in Australia. Austalian Health Review, 35-39.
Delaney, L. J. (2018). Patient-centred care as an approach to improving health care in Australia.
Austalian Journal of Nursing Practice, scholarship and Research, 119-123.
Fiona Robards, Melissa Kang, Time Usherwood, lena Sanci, catherine Hawke, Stephen Jan, Marlene Kong
& Katharine S. (2018). How Do Marginalized Young People Navigate the Australian Healthcare
System? Journal od Adolescent Health, 112-113.
Hall & Jane. (2015). Australian Health Care — The Challenge of Reform in a Fragmented System. The
New England Journal of Medicine, 45-56.
J. Macri. (2015). Australia's Health System: Some Issues and Challenges. Journal of Health and Medical
Economics, 56-67.
J. Wardle, A. Steel, R.Lauche, J. Adams. (2017). Collaborating with medicine? Perceptions of Australian
naturopaths on integrating within the conventional medical system. Journal of Interprofessional
Care, 734-743.
Jie-LiLi. (2017). Cultural barriers lead to inequitable healthcare access for aboriginal Australians and
Torres Strait Islanders. ScienceDirect, 76-78. Retrieved from
https://www.sciencedirect.com/science/article/pii/S2095771817301044
Kate Charlesworth, Maggie Jameison, Colin D. Butler & rachel Davey. (2015). The future healthcare?
Australian Health Review, 53-59.
MacIntyre & C. R. (2011). Public health and health reform in Australia. The Medical Journal of Australia.
Arunima Malik, Prof Manfrod Lenzen, Scott McAlister & Forbes McGain (2018). The carbon footprint of
Australian health care. The Lancet, 112-124. Retrieved from
https://www.thelancet.com/journals/lanplh/article/PIIS2542-5196(17)30180-8/fulltext
Bruce K Armstrong, James A Gillespie, Stephen R Leeder, george L rubin & Lesley M Rusell. (2007).
Challenges in health and health care for Australia. Medical Journal of Australia, 23-34. Retrieved
from https://www.mja.com.au/journal/2007/187/9/challenges-health-and-health-care-australia
Caroline Nicholson, Jackson C L, Marley J &Wells R. (2012). The Australian Experiment: How Primary
Health Care Organizations Supported the Evolution of a Primary Health Care System. Journal of
the American Board of Family Income, 32-35. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/22403246
Davinia S. E. Seah, T. Z. Cheong, Matthew & H. R. Anstey (2012). The hidden cost of private health
insurance in Australia. Austalian Health Review, 35-39.
Delaney, L. J. (2018). Patient-centred care as an approach to improving health care in Australia.
Austalian Journal of Nursing Practice, scholarship and Research, 119-123.
Fiona Robards, Melissa Kang, Time Usherwood, lena Sanci, catherine Hawke, Stephen Jan, Marlene Kong
& Katharine S. (2018). How Do Marginalized Young People Navigate the Australian Healthcare
System? Journal od Adolescent Health, 112-113.
Hall & Jane. (2015). Australian Health Care — The Challenge of Reform in a Fragmented System. The
New England Journal of Medicine, 45-56.
J. Macri. (2015). Australia's Health System: Some Issues and Challenges. Journal of Health and Medical
Economics, 56-67.
J. Wardle, A. Steel, R.Lauche, J. Adams. (2017). Collaborating with medicine? Perceptions of Australian
naturopaths on integrating within the conventional medical system. Journal of Interprofessional
Care, 734-743.
Jie-LiLi. (2017). Cultural barriers lead to inequitable healthcare access for aboriginal Australians and
Torres Strait Islanders. ScienceDirect, 76-78. Retrieved from
https://www.sciencedirect.com/science/article/pii/S2095771817301044
Kate Charlesworth, Maggie Jameison, Colin D. Butler & rachel Davey. (2015). The future healthcare?
Australian Health Review, 53-59.
MacIntyre & C. R. (2011). Public health and health reform in Australia. The Medical Journal of Australia.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.