Comprehensive Analysis of HIV: Stages, Myths, Education, and Stigma
VerifiedAdded on 2022/08/23
|8
|1829
|27
Homework Assignment
AI Summary
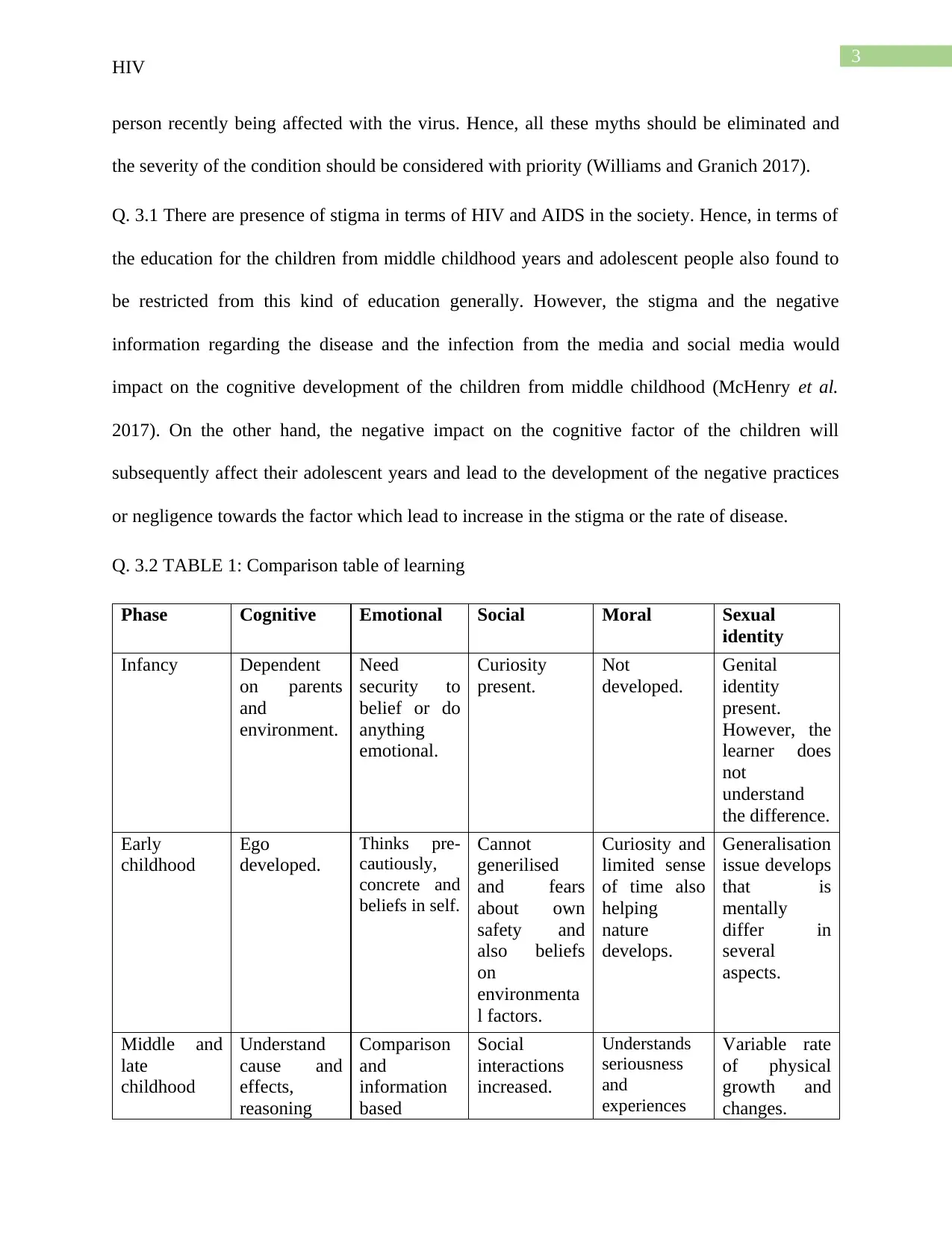
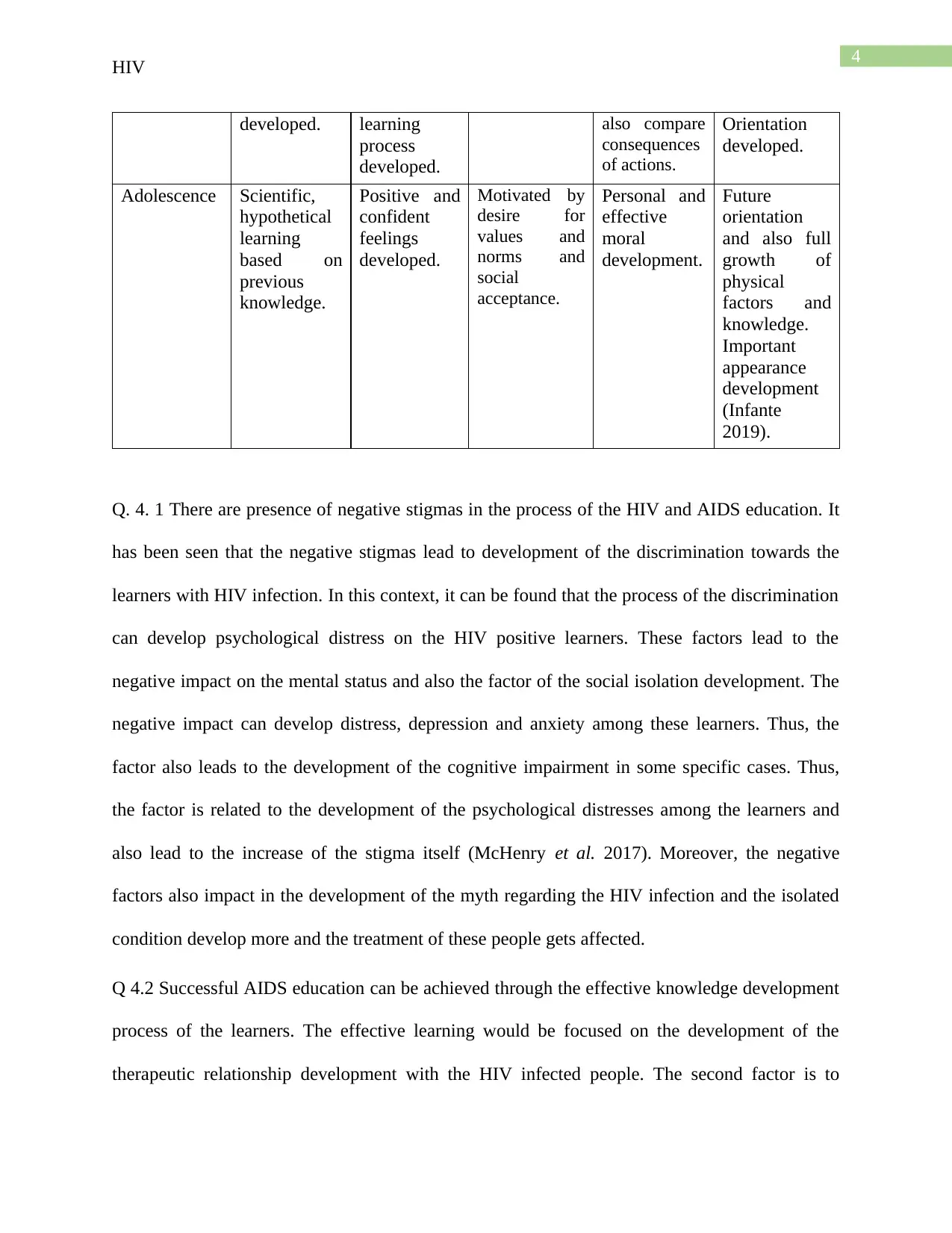
This assignment provides a detailed exploration of HIV, starting with an introduction to the virus and its impact on the human immune system, specifically targeting CD4 cells. It outlines the stages of HIV infection, from the asymptomatic stage to AIDS and death, including the symptoms associated with each stage. The assignment addresses common myths and misconceptions about HIV transmission, emphasizing the importance of safe sex practices. It also examines the societal stigma surrounding HIV and its impact on education, particularly for children and adolescents, and includes a comparison table of learning phases. Furthermore, it discusses the psychological distress and discrimination faced by HIV-positive individuals and suggests strategies for successful AIDS education, focusing on therapeutic relationships, health promotion programs, and the elimination of myths. The document references several research papers to support its findings and recommendations.


1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.