Research Proposal: Predictive Factors for Hodgkin's Lymphoma Patients
VerifiedAdded on 2023/01/19
|25
|7129
|50
Project
AI Summary
This research proposal explores predictive factors associated with Hodgkin's lymphoma relapse. It begins with an introduction to cancer, life expectancy, and lymphoma, specifically focusing on Hodgkin's lymphoma, its stages, and the impact of aging. The proposal includes a literature review, detailing the search strategy and a review of relevant articles. It outlines the research question, aims, and objectives, providing an overview of the study's methodology, including study design, sample selection, data collection, and analysis. Ethical considerations, a study timetable, a Gantt chart, and resource allocation are also presented, along with plans for dissemination and a conclusion. The proposal aims to identify factors that predict patient outcomes after relapse, contributing to improved treatment strategies and patient care. The document is a comprehensive overview of the research process, from background information to detailed methodological approaches.

Running head: RESEARCH PROPOSAL
Predictive factors which associate patients with Hodgkin’s lymphoma after relapse
Name of the Student
Name of the University
Author Note
Predictive factors which associate patients with Hodgkin’s lymphoma after relapse
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
RESEARCH PROPOSAL
Table of Contents
Introduction...................................................................................................................2
Cancer and life expectancy.......................................................................................2
Lymphoma................................................................................................................3
Hodgkin’s Lymphoma............................................................................................4
Advanced stage........................................................................................................5
Hodgkin’s Lymphoma and aging...........................................................................5
Background to the study...........................................................................................7
Literature Review..........................................................................................................7
Literature Search Strategy........................................................................................7
Review of the Articles...............................................................................................8
Research question......................................................................................................11
Research aim..............................................................................................................12
Research objectives...................................................................................................12
Overview of the study.............................................................................................12
Methodology...............................................................................................................13
Study Design...........................................................................................................13
Sample........................................................................................................................15
Data collection............................................................................................................16
Data Analysis..............................................................................................................17
Ethical Issues..............................................................................................................17
Study Time Table........................................................................................................18
Grant Chart.............................................................................................................18
Resources...................................................................................................................19
Dissemination.............................................................................................................19
Conclusion..................................................................................................................20
References.................................................................................................................21
RESEARCH PROPOSAL
Table of Contents
Introduction...................................................................................................................2
Cancer and life expectancy.......................................................................................2
Lymphoma................................................................................................................3
Hodgkin’s Lymphoma............................................................................................4
Advanced stage........................................................................................................5
Hodgkin’s Lymphoma and aging...........................................................................5
Background to the study...........................................................................................7
Literature Review..........................................................................................................7
Literature Search Strategy........................................................................................7
Review of the Articles...............................................................................................8
Research question......................................................................................................11
Research aim..............................................................................................................12
Research objectives...................................................................................................12
Overview of the study.............................................................................................12
Methodology...............................................................................................................13
Study Design...........................................................................................................13
Sample........................................................................................................................15
Data collection............................................................................................................16
Data Analysis..............................................................................................................17
Ethical Issues..............................................................................................................17
Study Time Table........................................................................................................18
Grant Chart.............................................................................................................18
Resources...................................................................................................................19
Dissemination.............................................................................................................19
Conclusion..................................................................................................................20
References.................................................................................................................21
2
RESEARCH PROPOSAL
Introduction
Cancer and life expectancy
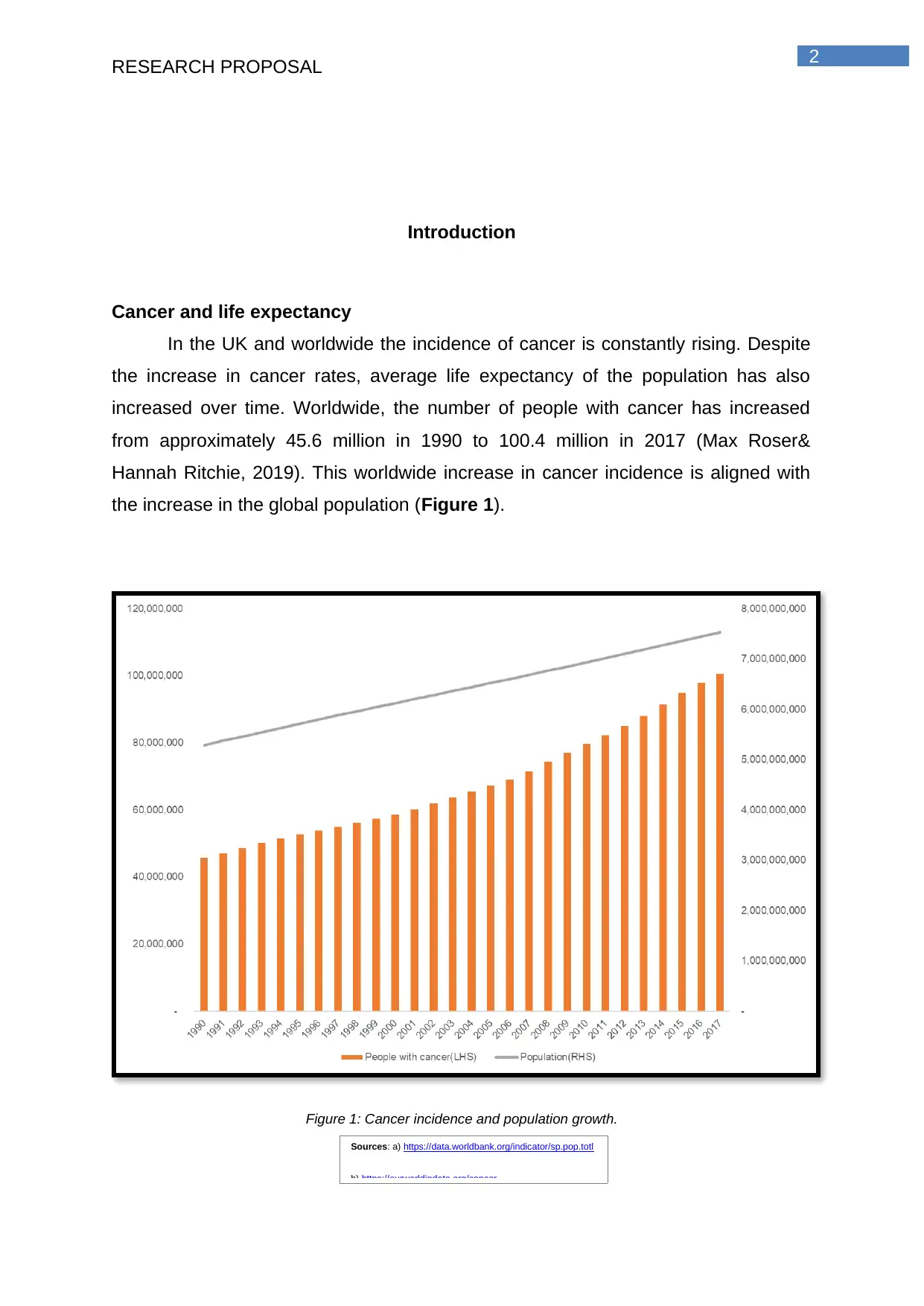
In the UK and worldwide the incidence of cancer is constantly rising. Despite
the increase in cancer rates, average life expectancy of the population has also
increased over time. Worldwide, the number of people with cancer has increased
from approximately 45.6 million in 1990 to 100.4 million in 2017 (Max Roser&
Hannah Ritchie, 2019). This worldwide increase in cancer incidence is aligned with
the increase in the global population (Figure 1).
Figure 1: Cancer incidence and population growth.
Sources: a) https://data.worldbank.org/indicator/sp.pop.totl
b) https://ourworldindata.org/cancer
RESEARCH PROPOSAL
Introduction
Cancer and life expectancy
In the UK and worldwide the incidence of cancer is constantly rising. Despite
the increase in cancer rates, average life expectancy of the population has also
increased over time. Worldwide, the number of people with cancer has increased
from approximately 45.6 million in 1990 to 100.4 million in 2017 (Max Roser&
Hannah Ritchie, 2019). This worldwide increase in cancer incidence is aligned with
the increase in the global population (Figure 1).
Figure 1: Cancer incidence and population growth.
Sources: a) https://data.worldbank.org/indicator/sp.pop.totl
b) https://ourworldindata.org/cancer
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
RESEARCH PROPOSAL
More specifically for the UK, the age-standardised cancer incidence rate has
increased for both men and women. The percentage include516.2 per 100,000
females in 2006 to 541.1 in 2016 and from 671.0 per 100,000 males in 2006 to 704.4
per 100,000 in 2013 (Office of National Statistics, 2019). Incidence rates forall
cancer types are strongly associated with the age of the cancer patients, with the
highest rate of incidence is observed among older people. Between 2013-2015 in the
UK, on average each year around 36% of reporting of new cases were in people
aged 75 and over (Cancer Research UK, 2019). Furthermore, cancer casesare
expected to rise even more in the next years. According to City of Hope (2019),
between 2010 and 2030, cancer incidence is expected to rise by around 67% in
those aged 65 or older. Also, the cancer incidence is expected to rise by 11% for
those under the age of 65.
Globally, deaths from cancer increased from 5.7million in 1990 to 9.5 million
in 2017(Max Roser& Hannah Ritchie, 2019). The number of deaths by cancer is not
only influenced by the actual change in the prevalence of cancer, but also from the
population size and age. One metric that corrects for the population size and age is
the age-standardised mortality rate. An age-standardised rate should not be affected
by any changes in the distribution of the population by age and size (WHO, 2019).
Although cancer incident numbers are increasing, the age-standardised death rate
from cancer is globally decreasing. According to Max Roser and Hannah Ritchie
(2019), the age-standardised mortality rate has decreased by between 15% to 20%
globally between 1990 and 2017.
Lymphoma
A big proportion of the blood cancers that occur are lymphomas or cancers of
the lymphatic system. Lymphomas are a group of lymphatic cancers that occur in the
lymphocytes. There are two types of Lymphomas, Hodgkin’s lymphoma and non-
Hodgkin’s lymphomas. Like many other type of cancers, the overall incidence of
lymphomas mainly increases by age, with a third of most newly diagnosed cases
diagnosed in those aged 75 years or older (Cancer Research UK, 2018).
Risk factors for lymphoma include:
RESEARCH PROPOSAL
More specifically for the UK, the age-standardised cancer incidence rate has
increased for both men and women. The percentage include516.2 per 100,000
females in 2006 to 541.1 in 2016 and from 671.0 per 100,000 males in 2006 to 704.4
per 100,000 in 2013 (Office of National Statistics, 2019). Incidence rates forall
cancer types are strongly associated with the age of the cancer patients, with the
highest rate of incidence is observed among older people. Between 2013-2015 in the
UK, on average each year around 36% of reporting of new cases were in people
aged 75 and over (Cancer Research UK, 2019). Furthermore, cancer casesare
expected to rise even more in the next years. According to City of Hope (2019),
between 2010 and 2030, cancer incidence is expected to rise by around 67% in
those aged 65 or older. Also, the cancer incidence is expected to rise by 11% for
those under the age of 65.
Globally, deaths from cancer increased from 5.7million in 1990 to 9.5 million
in 2017(Max Roser& Hannah Ritchie, 2019). The number of deaths by cancer is not
only influenced by the actual change in the prevalence of cancer, but also from the
population size and age. One metric that corrects for the population size and age is
the age-standardised mortality rate. An age-standardised rate should not be affected
by any changes in the distribution of the population by age and size (WHO, 2019).
Although cancer incident numbers are increasing, the age-standardised death rate
from cancer is globally decreasing. According to Max Roser and Hannah Ritchie
(2019), the age-standardised mortality rate has decreased by between 15% to 20%
globally between 1990 and 2017.
Lymphoma
A big proportion of the blood cancers that occur are lymphomas or cancers of
the lymphatic system. Lymphomas are a group of lymphatic cancers that occur in the
lymphocytes. There are two types of Lymphomas, Hodgkin’s lymphoma and non-
Hodgkin’s lymphomas. Like many other type of cancers, the overall incidence of
lymphomas mainly increases by age, with a third of most newly diagnosed cases
diagnosed in those aged 75 years or older (Cancer Research UK, 2018).
Risk factors for lymphoma include:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
RESEARCH PROPOSAL
● Relatively uncommon risk factors. The most common example of relatively
uncommon risk factors is immune-deficiency states. As it is mentioned by
Hatton, Collins andSweetenham (2014) the emergence of HIV/AIDS during
the 1980s and 1990s was reflected by the rising incidence of lymphoma
during this period. Furthermore, there has been a significant decrease of
AIDS-associated lymphoma since the introductionof highly active anti-
retroviral therapy (HAART).
● Common risk factors. Many studies have implicated incidence and
development of lymphoma with various environmental factors. Many of these
studies have the disadvantage of recall or selection bias.However, a non-
harmful environmental exposure which is not highly related with the incidence
of lymphoma can still contribute substantially to the rising incidence of
lymphoma if this exposure happens to a large number of people.
Different treatments forHodgkin’s and non-Hodgkin’s lymphomas include
systematic treatment like chemotherapy and immunotherapy, or localised treatments
such as radiotherapy.There are two treatment options which are
● Curative (i.e., eradicate the cancer completely)
● Palliative (i.e., alleviate symptoms of cancer)
The treatment option is selected based on the lymphoma type, previous
treatments, other health problems and patient wishes (National Institute for Clinical
Excellence, 2004).
Hodgkin’s Lymphoma
Hodgkin’s lymphoma is a type of lymphoma which emerges from a malignant
B-cell. Therefore, Hodgkin’s lymphoma is regarded as a B-cell lymphoma. It usually
affects young people and it can be cured in most cases.The most common signs of
adult Hodgkin’s lymphoma are swollen lymph nodes, high fever, night time sweats,
and extreme weight loss (National Cancer Institute,2019).
Hodgkin’s lymphoma is divided into the following two types:
RESEARCH PROPOSAL
● Relatively uncommon risk factors. The most common example of relatively
uncommon risk factors is immune-deficiency states. As it is mentioned by
Hatton, Collins andSweetenham (2014) the emergence of HIV/AIDS during
the 1980s and 1990s was reflected by the rising incidence of lymphoma
during this period. Furthermore, there has been a significant decrease of
AIDS-associated lymphoma since the introductionof highly active anti-
retroviral therapy (HAART).
● Common risk factors. Many studies have implicated incidence and
development of lymphoma with various environmental factors. Many of these
studies have the disadvantage of recall or selection bias.However, a non-
harmful environmental exposure which is not highly related with the incidence
of lymphoma can still contribute substantially to the rising incidence of
lymphoma if this exposure happens to a large number of people.
Different treatments forHodgkin’s and non-Hodgkin’s lymphomas include
systematic treatment like chemotherapy and immunotherapy, or localised treatments
such as radiotherapy.There are two treatment options which are
● Curative (i.e., eradicate the cancer completely)
● Palliative (i.e., alleviate symptoms of cancer)
The treatment option is selected based on the lymphoma type, previous
treatments, other health problems and patient wishes (National Institute for Clinical
Excellence, 2004).
Hodgkin’s Lymphoma
Hodgkin’s lymphoma is a type of lymphoma which emerges from a malignant
B-cell. Therefore, Hodgkin’s lymphoma is regarded as a B-cell lymphoma. It usually
affects young people and it can be cured in most cases.The most common signs of
adult Hodgkin’s lymphoma are swollen lymph nodes, high fever, night time sweats,
and extreme weight loss (National Cancer Institute,2019).
Hodgkin’s lymphoma is divided into the following two types:
5
RESEARCH PROPOSAL
Classic Hodgkin’s lymphoma (cHL): Approximately 1800 new cases of CHL
are diagnosed every year in the UK. The majority of the patients are between
15 and 35 years old (Hatton, Collins &Sweetenham, 2014).
Nodular lymphocyte-predominant Hodgkin’s lymphoma (nLPHL): nLPHL is
more rare and clinically different than cHL and the malignant cell is called
lymphocytic and histiocytic (L&H) call.
Management
Early stage cHL used to be treated by radiotherapy alone. The disadvantage
of this treatment was the association with high relapse rate and toxicities caused by
the radiotherapy. Recent treatments involve two to four cycles of chemotherapy
(e.g., ABVD) which sometimes is followed by radiotherapy. There are two groups of
treatments for early stage nLPHL patients(Lymphoma Action, 2019). Patients without
B symptoms usually have a surgery to remove all lymph nodes that contain
lymphoma, or radiotherapy alone, or a combination of a surgery followed by
radiotherapy. nLPHL patients with B symptoms need stronger treatments which
involve chemotherapy.
Advanced stage
Hodgkin’s Lymphoma and aging
Hodgkin lymphoma affects both children and adults and it is most commonly divided
in the following groups:
The first group contains people aged from 15 to 40years old and usually
young adults in their 20s.
The second group contains older people over 55 years old.
The average age of diagnosis is 39. However, the disease is rare in children who
are younger than 5 years. It is the most commonly diagnosed cancer in teens ages
15 to 19years(Cancer.Net, 2019).A 5-year survival rate is used to estimatethe
approximate percent of people live at least 5 years after the diagnosis of cancer. The
5-year survival rate for all people with Hodgkin lymphoma is 87%. Depending on the
stage the 5-year survival rates are the following:
Stage I – 92%
Stage II – 93%
RESEARCH PROPOSAL
Classic Hodgkin’s lymphoma (cHL): Approximately 1800 new cases of CHL
are diagnosed every year in the UK. The majority of the patients are between
15 and 35 years old (Hatton, Collins &Sweetenham, 2014).
Nodular lymphocyte-predominant Hodgkin’s lymphoma (nLPHL): nLPHL is
more rare and clinically different than cHL and the malignant cell is called
lymphocytic and histiocytic (L&H) call.
Management
Early stage cHL used to be treated by radiotherapy alone. The disadvantage
of this treatment was the association with high relapse rate and toxicities caused by
the radiotherapy. Recent treatments involve two to four cycles of chemotherapy
(e.g., ABVD) which sometimes is followed by radiotherapy. There are two groups of
treatments for early stage nLPHL patients(Lymphoma Action, 2019). Patients without
B symptoms usually have a surgery to remove all lymph nodes that contain
lymphoma, or radiotherapy alone, or a combination of a surgery followed by
radiotherapy. nLPHL patients with B symptoms need stronger treatments which
involve chemotherapy.
Advanced stage
Hodgkin’s Lymphoma and aging
Hodgkin lymphoma affects both children and adults and it is most commonly divided
in the following groups:
The first group contains people aged from 15 to 40years old and usually
young adults in their 20s.
The second group contains older people over 55 years old.
The average age of diagnosis is 39. However, the disease is rare in children who
are younger than 5 years. It is the most commonly diagnosed cancer in teens ages
15 to 19years(Cancer.Net, 2019).A 5-year survival rate is used to estimatethe
approximate percent of people live at least 5 years after the diagnosis of cancer. The
5-year survival rate for all people with Hodgkin lymphoma is 87%. Depending on the
stage the 5-year survival rates are the following:
Stage I – 92%
Stage II – 93%
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
RESEARCH PROPOSAL
Stage III – 83%
Stage IV – 73%
The rates may be affected by the cancer subtypes and the stages of Hodgkin
lymphoma and the age and gender of the patient (Cancer.Net, 2019).
RESEARCH PROPOSAL
Stage III – 83%
Stage IV – 73%
The rates may be affected by the cancer subtypes and the stages of Hodgkin
lymphoma and the age and gender of the patient (Cancer.Net, 2019).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
RESEARCH PROPOSAL
Background to the study
A review of previously published literature is important in order to gain proper
understanding about the topic of the research, the scope of the research, research
gap and research question (Kinght, 2002). “Claim making” then helps to connect
these understanding with the ideas that are pre-existing in the literature in order to
support the significance of the conduction of research. It also helps to set the
direction of the research of the path in which the research is required to be
undertaken (Kinght, 2002). The positioning of the research proposal in relation to the
review of literature is regarded as one of the primary pillar of the conceptual
framework generation of the research (Holliday, 2016).
Literature Review
Literature Search Strategy
The main databases that were used for the research of the literary article
include Medline, CINHAL, BNI and PsycINFO. The databases were accessed with
the help of NICE Healthcare Database Advanced Search (HDAS). These databases
were selected for the search of the previously published literary articles because
there databases are hub of literary papers that are aligned to nursing research, or
the scope of professional practice of allied healthcare professionals, mental health
therapists and health or social care workers. Since the main aim of the research was
to align with the nursing or medical practice, the selection of these databases was
justified.
The keywords were used that found to coincide with the research topic and
this include predictive factors, Hodgkin’s lymphoma and relapse. Other associated
keywords that are used include relapse factors, lymphomas, chemotherapy. Broader
keywords were used in order to increase the overall hits in the database search.
Boolean operators like AND, OR and NOT were used in order to narrow down and
expand the search result accordingly. Whenever required truncation of words were
used in order to vary or manipulate the ends or spellings. The searches of the literary
articles were restricted within last 10 years (2009 to 2019). English language and the
subty that were conducted over the human subjects were two other inclusion criteria
used for the study. The type of publication were restricted to book, clinical trial,
RESEARCH PROPOSAL
Background to the study
A review of previously published literature is important in order to gain proper
understanding about the topic of the research, the scope of the research, research
gap and research question (Kinght, 2002). “Claim making” then helps to connect
these understanding with the ideas that are pre-existing in the literature in order to
support the significance of the conduction of research. It also helps to set the
direction of the research of the path in which the research is required to be
undertaken (Kinght, 2002). The positioning of the research proposal in relation to the
review of literature is regarded as one of the primary pillar of the conceptual
framework generation of the research (Holliday, 2016).
Literature Review
Literature Search Strategy
The main databases that were used for the research of the literary article
include Medline, CINHAL, BNI and PsycINFO. The databases were accessed with
the help of NICE Healthcare Database Advanced Search (HDAS). These databases
were selected for the search of the previously published literary articles because
there databases are hub of literary papers that are aligned to nursing research, or
the scope of professional practice of allied healthcare professionals, mental health
therapists and health or social care workers. Since the main aim of the research was
to align with the nursing or medical practice, the selection of these databases was
justified.
The keywords were used that found to coincide with the research topic and
this include predictive factors, Hodgkin’s lymphoma and relapse. Other associated
keywords that are used include relapse factors, lymphomas, chemotherapy. Broader
keywords were used in order to increase the overall hits in the database search.
Boolean operators like AND, OR and NOT were used in order to narrow down and
expand the search result accordingly. Whenever required truncation of words were
used in order to vary or manipulate the ends or spellings. The searches of the literary
articles were restricted within last 10 years (2009 to 2019). English language and the
subty that were conducted over the human subjects were two other inclusion criteria
used for the study. The type of publication were restricted to book, clinical trial,
8
RESEARCH PROPOSAL
journal articles, systematic review and meta-analysis of randomised control trial,
meta-synthesis and other randomised control trial studies. The total number of
articles found after the initial search was 207. Of them 34 were found to coincide with
the scope of the study. Of them only 4 studies were qualitative studies and were
reviewed below based on the parameters highlighted by the qualitative framework of
Critical Appraisal Skills Programme (CASPs) (CASP, 2018).
Review of the Articles
The systematic review conducted by Townsend and Linch (2012) was
selected in order to get a brief overview of the prognosis and pathophysiology of
Hodgkin’s lymphoma. Getting a detailed insight of the pathophysiology of Hodgkin’s
lymphoma will help to ascertain the plausible caused behind the relapse of Hodgkin’s
lymphoma. Townsend and Linch (2012) stated that majority of the patients with
Hodgkin’s lymphoma are cured after the first line of therapy. However, the main
challenge in the disease treatment is management of the toxic disease outcome and
improvement in the overall survival rate of the patients who have relapsed with the
disease and have poor refractory advances. The review conducted by Townsend
and Linch (2012) highlighted that the main international prognostic index
(Hasencleverscore) for the advance stage of the Hodgkin’s lymphoma is age greater
than 45v years of age, sex is male, high concentration of the serum albumin (greater
than 40 gram per litre), poor level of haemoglobin concentration (less than 105 gram
per litre), the people who are in their stage IV of their disease. Other factors that
modulates the international prognostic index is high level of leucocytosis, (either
greater than or equals to 15 x 10^9 white cells per litre, low level of lymphopenia
(less than 0.6 x 10^9 lymphocytes per litre). Both the study conducted by Townsend
and Linch (2012) and Hosing et al. (2009) showed that low platelet count is one of
the predictive factor behind the possible chances of disease relapse in both Hodgkin
and non-Hodgkin’s lymphoma patients. However, Townsend and Linch (2012)also
highlighted in their study that the International prognostic index (Hasenclever score)
is a direct representative of negative progression of the disease and cannot be
regarded as predictive factors behind the relapse of Hodgkin’s lymphoma.
The study conducted by Majhailet al. (2009) was aimed towards identifying
the long-term outcomes for the autologous haematopoietic-cell transplantation for
the treatment of the advanced Hodgkin (HL) and non-Hodgkin lymphoma (NHL). The
RESEARCH PROPOSAL
journal articles, systematic review and meta-analysis of randomised control trial,
meta-synthesis and other randomised control trial studies. The total number of
articles found after the initial search was 207. Of them 34 were found to coincide with
the scope of the study. Of them only 4 studies were qualitative studies and were
reviewed below based on the parameters highlighted by the qualitative framework of
Critical Appraisal Skills Programme (CASPs) (CASP, 2018).
Review of the Articles
The systematic review conducted by Townsend and Linch (2012) was
selected in order to get a brief overview of the prognosis and pathophysiology of
Hodgkin’s lymphoma. Getting a detailed insight of the pathophysiology of Hodgkin’s
lymphoma will help to ascertain the plausible caused behind the relapse of Hodgkin’s
lymphoma. Townsend and Linch (2012) stated that majority of the patients with
Hodgkin’s lymphoma are cured after the first line of therapy. However, the main
challenge in the disease treatment is management of the toxic disease outcome and
improvement in the overall survival rate of the patients who have relapsed with the
disease and have poor refractory advances. The review conducted by Townsend
and Linch (2012) highlighted that the main international prognostic index
(Hasencleverscore) for the advance stage of the Hodgkin’s lymphoma is age greater
than 45v years of age, sex is male, high concentration of the serum albumin (greater
than 40 gram per litre), poor level of haemoglobin concentration (less than 105 gram
per litre), the people who are in their stage IV of their disease. Other factors that
modulates the international prognostic index is high level of leucocytosis, (either
greater than or equals to 15 x 10^9 white cells per litre, low level of lymphopenia
(less than 0.6 x 10^9 lymphocytes per litre). Both the study conducted by Townsend
and Linch (2012) and Hosing et al. (2009) showed that low platelet count is one of
the predictive factor behind the possible chances of disease relapse in both Hodgkin
and non-Hodgkin’s lymphoma patients. However, Townsend and Linch (2012)also
highlighted in their study that the International prognostic index (Hasenclever score)
is a direct representative of negative progression of the disease and cannot be
regarded as predictive factors behind the relapse of Hodgkin’s lymphoma.
The study conducted by Majhailet al. (2009) was aimed towards identifying
the long-term outcomes for the autologous haematopoietic-cell transplantation for
the treatment of the advanced Hodgkin (HL) and non-Hodgkin lymphoma (NHL). The
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
RESEARCH PROPOSAL
study included the recipients of the autologous HCT for NHL (960) and HL (407)
during the tenure of 1990 to 1998. These patients were under the complete
remission for at least 2 long years after the HCT. The selection of the large sample
size for both the HL and NHL group can be regarded as one of the strength of the
study. Marshall, Cardon, Poddar and Fontenot (2013) stated that large sample size
helps to interpret the results in a generalised format. The study pattern included
median follow-up for 104 months for HL and 107 months for NHL. The use of the
long follow-up sessions for the cancer patients study can be regarded as one of the
significant limitation as the number of total population might get reduced during the
follow-up sessions and thus limiting the sample size. The sourcing of the data was
done from the Centre for International Blood and Marrow Transplant Research
(CIBMTR). It is a voluntary group with more than 500 transplant centres worldwide.
Souring data from internationally operating group is strength of the study and it
helped to get an overview of the international aspect of the cancer scenario.The
study highlighted that the overall survival rate of at least 10 years is 77% for HL and
78% of NHL. The study also showed through the multi-variative analysis highlighted
that patients who are suffering from mantle-cell NHL have highest risk of late stage
mortality arising out of disease relapse. The relapse is regarded as one of the most
common cause of death between both NHL ad HL patients. Though the exact cause
of relapse was not highlighted in the study as it was not the direct scope of the study
however, Majhail et al. (2009) stated that people who are greater than 55 years of
age, gender is male, and lead an unhealthy lifestyle are more prone towards
becoming the victim of disease relapse in HL and NHL. The overall result of the
study showed that recipients of autologous HCT for both the NHL and HL who
remain in remission for at least 2 years have favourable condition for subsequent
long-term survival but the level of risk of relapse is high during late stage of life. The
study also showed that the rate of mortality is high among the lymphoma population
with patients after 10 years of post-transplantation. Overall the study highlighted
some common factors behind the relapse of the disease like the age and gender and
this is similar in with the factors highlighted in the study of Townsend and Linch
(2012). Townsend and Linch (2012) however, highlighted some common factors
behind the relapse of the disease and this is unhealthy lifestyle habits. Linsky,
Nyambose and Battaglia (2011) state that unhealthy lifestyle habits (smoking and
drinking) not only leads to poor propagation of the non-communicable disease but
RESEARCH PROPOSAL
study included the recipients of the autologous HCT for NHL (960) and HL (407)
during the tenure of 1990 to 1998. These patients were under the complete
remission for at least 2 long years after the HCT. The selection of the large sample
size for both the HL and NHL group can be regarded as one of the strength of the
study. Marshall, Cardon, Poddar and Fontenot (2013) stated that large sample size
helps to interpret the results in a generalised format. The study pattern included
median follow-up for 104 months for HL and 107 months for NHL. The use of the
long follow-up sessions for the cancer patients study can be regarded as one of the
significant limitation as the number of total population might get reduced during the
follow-up sessions and thus limiting the sample size. The sourcing of the data was
done from the Centre for International Blood and Marrow Transplant Research
(CIBMTR). It is a voluntary group with more than 500 transplant centres worldwide.
Souring data from internationally operating group is strength of the study and it
helped to get an overview of the international aspect of the cancer scenario.The
study highlighted that the overall survival rate of at least 10 years is 77% for HL and
78% of NHL. The study also showed through the multi-variative analysis highlighted
that patients who are suffering from mantle-cell NHL have highest risk of late stage
mortality arising out of disease relapse. The relapse is regarded as one of the most
common cause of death between both NHL ad HL patients. Though the exact cause
of relapse was not highlighted in the study as it was not the direct scope of the study
however, Majhail et al. (2009) stated that people who are greater than 55 years of
age, gender is male, and lead an unhealthy lifestyle are more prone towards
becoming the victim of disease relapse in HL and NHL. The overall result of the
study showed that recipients of autologous HCT for both the NHL and HL who
remain in remission for at least 2 years have favourable condition for subsequent
long-term survival but the level of risk of relapse is high during late stage of life. The
study also showed that the rate of mortality is high among the lymphoma population
with patients after 10 years of post-transplantation. Overall the study highlighted
some common factors behind the relapse of the disease like the age and gender and
this is similar in with the factors highlighted in the study of Townsend and Linch
(2012). Townsend and Linch (2012) however, highlighted some common factors
behind the relapse of the disease and this is unhealthy lifestyle habits. Linsky,
Nyambose and Battaglia (2011) state that unhealthy lifestyle habits (smoking and
drinking) not only leads to poor propagation of the non-communicable disease but
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
RESEARCH PROPOSAL
also increase the tendency of relapse of cancer. The unique approach highlighted in
the study, irrespective of the nature of the disease like the Hodgkin's and non-
Hodgkin's lymphoma, eve under the treatment of the bone-marrow transplant, the
disease mainly relapse within 10 years. Review of this study also helped us to
understand that irrespective of the best treatment given to the NHL, the relapse of
the disease is inevitable.
The study conducted by Casuloet al. (2015) was based on the follicular
lymphoma (FL). The study was selected as it coincided with the boarder keywords
that were used in the database search. The aim of the study was to identify the
prognostic FL factors that are interlinked with the prognosis of the disease (POD).
The study also helped in highlighting whether early POD are at high risk for disease
relapsing and recurrence. Casulo et al. (2015) screened 588 patients who are in their
stage two of the FL factors who are receiving their first-line R-CHOP therapy
(rituximan plus cyclophosphamaide, doxorubicin, vincristine and prednisone). The
mainly use an independent validation set of 147 patients with FL who have received
their first line of RCHOP and the results was analysed based for reproducibility. The
results showed that 588 patients that are 19% had early POD and 71% were under
the reference group and 8% were lost in the follow-up and 2% died during the course
of the study. The decrease in the sample size during the follow-up session can be
regarded as one of the limitation of the study as it restricted generaisability of the
data. The analysis of the results highlighted that the FL patients who received first-
line of R-CHOP, POD within their 2 years of disease diagnosis was associated with
poor outcomes. Thus further validation is required to be undertaken at standard point
of time by the use of the chemo-immunotherapy trials of the untreated FL. The
overall study showed that high-risk FL population must be studied further in order to
highlight the predictive factors for the disease recurrence. The study mainly showed
that starting disease treatment with the use of chemotherapy within 2 years of the
disease diagnosis help to increase the relapse of the disease.
The study conducted by Martinez et al. (2013) is based on the Hodgkin’s
lymphoma patients how are fighting through disease relapse after autologous
transplantation of stem cells. The aim of the study is to elucidate new information
about the predictors of the outcomes for the patients whose Hodgkin’s disease has
reoccur after the autologous stem cell transplant (ASCT). The study included 511
RESEARCH PROPOSAL
also increase the tendency of relapse of cancer. The unique approach highlighted in
the study, irrespective of the nature of the disease like the Hodgkin's and non-
Hodgkin's lymphoma, eve under the treatment of the bone-marrow transplant, the
disease mainly relapse within 10 years. Review of this study also helped us to
understand that irrespective of the best treatment given to the NHL, the relapse of
the disease is inevitable.
The study conducted by Casuloet al. (2015) was based on the follicular
lymphoma (FL). The study was selected as it coincided with the boarder keywords
that were used in the database search. The aim of the study was to identify the
prognostic FL factors that are interlinked with the prognosis of the disease (POD).
The study also helped in highlighting whether early POD are at high risk for disease
relapsing and recurrence. Casulo et al. (2015) screened 588 patients who are in their
stage two of the FL factors who are receiving their first-line R-CHOP therapy
(rituximan plus cyclophosphamaide, doxorubicin, vincristine and prednisone). The
mainly use an independent validation set of 147 patients with FL who have received
their first line of RCHOP and the results was analysed based for reproducibility. The
results showed that 588 patients that are 19% had early POD and 71% were under
the reference group and 8% were lost in the follow-up and 2% died during the course
of the study. The decrease in the sample size during the follow-up session can be
regarded as one of the limitation of the study as it restricted generaisability of the
data. The analysis of the results highlighted that the FL patients who received first-
line of R-CHOP, POD within their 2 years of disease diagnosis was associated with
poor outcomes. Thus further validation is required to be undertaken at standard point
of time by the use of the chemo-immunotherapy trials of the untreated FL. The
overall study showed that high-risk FL population must be studied further in order to
highlight the predictive factors for the disease recurrence. The study mainly showed
that starting disease treatment with the use of chemotherapy within 2 years of the
disease diagnosis help to increase the relapse of the disease.
The study conducted by Martinez et al. (2013) is based on the Hodgkin’s
lymphoma patients how are fighting through disease relapse after autologous
transplantation of stem cells. The aim of the study is to elucidate new information
about the predictors of the outcomes for the patients whose Hodgkin’s disease has
reoccur after the autologous stem cell transplant (ASCT). The study included 511
11
RESEARCH PROPOSAL
adult patients with relapsed HL after getting ASCT. Theinformation was extracted
from the EBMT-GITMO databases. The results showed that the main treatments
administered after the AST failure are conventional chemotherapy and/or
radiotherapy and the requirement of the second line of these therapy was evident
from at least 90% of the population is highlighted from the data of the 49 months of
follow up. The mains factors that promoted increase severity of the disease relapse
is people who are in their stage IV of the disease, have the age group of more than
50 years and with poor performance status of the disease are more likely to become
victim of the disease relapse (Martinez et al., 2013). This again coincided with the
study of Townsend and Linch (2012) that also showed that predictive factors of
disease relapse in case of Hodgkin's lymphoma is age, stage of the disease and
lifestyle habits. One of the limitations of the diseaseis they study only the population
that has availed the ASCT and not other therapy of the
The scared availability of papers in the electronic database highlighted in that
there is a limited availability of papers in the domain of Hodgkin's lymphoma and the
predictive factors associated with disease relapse. The analysis of the paper
however, helped in the identification that Hodgkin's lymphoma disease has a high
rate of relapse irrespective of the nature of the treatment like AST, chemotherapy
and radiotherapy. Review of the papers also indentified few common predictive
factors behind the disease relapse and this includes age of the patients, gender of
the patients, poor platelets and haemoglobin counts and lifestyle of the patients.
Hosinget al. (2009) are of the opinion that proper identification of the predictive
factors for the disease relapse in case of Hodgkin's lymphoma will help to devise
proper therapy plan for the disease treatment and disease relapse prevention.
Hosing et al. (2009) state that having proper knowledge about the lymphoma will
help to design person-centred care and thereby helping to promote successful
outcome of the disease prognosis.
Research question
Since there was no research conducted so far to highlight the perspective of
the healthcare professional over the predictive factors behind the relapse of the
Hodgkin’s lymphoma, thus the main research question will be:
RESEARCH PROPOSAL
adult patients with relapsed HL after getting ASCT. Theinformation was extracted
from the EBMT-GITMO databases. The results showed that the main treatments
administered after the AST failure are conventional chemotherapy and/or
radiotherapy and the requirement of the second line of these therapy was evident
from at least 90% of the population is highlighted from the data of the 49 months of
follow up. The mains factors that promoted increase severity of the disease relapse
is people who are in their stage IV of the disease, have the age group of more than
50 years and with poor performance status of the disease are more likely to become
victim of the disease relapse (Martinez et al., 2013). This again coincided with the
study of Townsend and Linch (2012) that also showed that predictive factors of
disease relapse in case of Hodgkin's lymphoma is age, stage of the disease and
lifestyle habits. One of the limitations of the diseaseis they study only the population
that has availed the ASCT and not other therapy of the
The scared availability of papers in the electronic database highlighted in that
there is a limited availability of papers in the domain of Hodgkin's lymphoma and the
predictive factors associated with disease relapse. The analysis of the paper
however, helped in the identification that Hodgkin's lymphoma disease has a high
rate of relapse irrespective of the nature of the treatment like AST, chemotherapy
and radiotherapy. Review of the papers also indentified few common predictive
factors behind the disease relapse and this includes age of the patients, gender of
the patients, poor platelets and haemoglobin counts and lifestyle of the patients.
Hosinget al. (2009) are of the opinion that proper identification of the predictive
factors for the disease relapse in case of Hodgkin's lymphoma will help to devise
proper therapy plan for the disease treatment and disease relapse prevention.
Hosing et al. (2009) state that having proper knowledge about the lymphoma will
help to design person-centred care and thereby helping to promote successful
outcome of the disease prognosis.
Research question
Since there was no research conducted so far to highlight the perspective of
the healthcare professional over the predictive factors behind the relapse of the
Hodgkin’s lymphoma, thus the main research question will be:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 25
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.