Examining the Intersection of Homelessness and Public Health Concerns
VerifiedAdded on 2020/05/28
|26
|5530
|115
AI Summary
The assignment explores the intricate connections between homelessness and health by analyzing existing literature that addresses how these issues intersect and affect vulnerable populations. Key topics include the prevalence of multimorbidity among the homeless, mental health concerns such as PTSD and psychological distress, barriers to healthcare access like insurance coverage and stigmatization, and specific vulnerabilities faced by subgroups including youth, women, and racial minorities within the homeless community. Research articles from multiple sources highlight these issues, showing how public policy can either mitigate or exacerbate the challenges faced by homeless individuals. The summary underscores the importance of targeted interventions and comprehensive public health strategies to improve outcomes for this marginalized group.

Running head: Homelessness as a public health risk
Homelessness a public health risk
Name of the Student
Name of the University
Author Note
Homelessness a public health risk
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1Homelessness as a public health risk
Contents
Introduction:...............................................................................................................................2
Facts about homelessness:......................................................................................................2
Homelessness in UK:.............................................................................................................2
Importance of discussing public health challenges:...................................................................3
Literature review: Public health perspectives on Homelessness:..............................................9
What could be done to address the challenge?.........................................................................12
Provision of Service:............................................................................................................12
Preventative Measures:........................................................................................................12
Accommodation:..................................................................................................................13
Social Networking:...............................................................................................................13
Promoting individual well being:.........................................................................................14
Barriers and Recommendations:..............................................................................................15
Barriers:................................................................................................................................15
Recommendations:...............................................................................................................17
Conclusion:..............................................................................................................................18
References:...............................................................................................................................20
Contents
Introduction:...............................................................................................................................2
Facts about homelessness:......................................................................................................2
Homelessness in UK:.............................................................................................................2
Importance of discussing public health challenges:...................................................................3
Literature review: Public health perspectives on Homelessness:..............................................9
What could be done to address the challenge?.........................................................................12
Provision of Service:............................................................................................................12
Preventative Measures:........................................................................................................12
Accommodation:..................................................................................................................13
Social Networking:...............................................................................................................13
Promoting individual well being:.........................................................................................14
Barriers and Recommendations:..............................................................................................15
Barriers:................................................................................................................................15
Recommendations:...............................................................................................................17
Conclusion:..............................................................................................................................18
References:...............................................................................................................................20
2Homelessness as a public health risk
Introduction:
Facts about homelessness:
Homelessness or lack of home can be a devastating, dangerous and isolating
experience, which can increase the risk of morbidity and mortality (due to the lack of security
and healthcare, as well as the risk of psychological trauma and suicide risk. It can be caused
due to socio-economic factors like a lack of affordable accommodation, poverty, lack of jobs,
and personal life events leading to homelessness, apart from mental and physical health
issues, addition issues and psychological trauma. Additionally, being homeless can further
increase risks for morbidity and mortality, and further complicate the health risks.
Homelessness can be categorized into three types: Rough Sleeping, Statutory Homelessness
and Hidden Homelessness (Crisis 2018). Rough sleeping refers to the individuals sleeping
rough on the streets, Statutory Homelessness refers to individuals who lack a secure place to
live, while hidden homelessness refers to individuals who have not approached or divulged
their lack of home to the authorities, and hence have not been listed homeless. United Nations
describes ‘absolute homelessness’ as a condition arising due to a lack of physical shelter,
causing people to sleep outdoors, in vehicles, abandoned buildings, or places not intended for
human settlement, while describing ’relative homelessness’ who have physical shelters that
does not meet basic health and safety standards (Hwang 2018).
Homelessness in UK:
Reports from November, 2017 shows that as estimated 307,000 (one out of every 200
people) people sleeping rough or lack adequate housing in the UK, with London having the
highest number of homeless people, and increasing problems of homelessness in places like
Broxbourne, Luton and Chelmsford (Butler 2017).
Introduction:
Facts about homelessness:
Homelessness or lack of home can be a devastating, dangerous and isolating
experience, which can increase the risk of morbidity and mortality (due to the lack of security
and healthcare, as well as the risk of psychological trauma and suicide risk. It can be caused
due to socio-economic factors like a lack of affordable accommodation, poverty, lack of jobs,
and personal life events leading to homelessness, apart from mental and physical health
issues, addition issues and psychological trauma. Additionally, being homeless can further
increase risks for morbidity and mortality, and further complicate the health risks.
Homelessness can be categorized into three types: Rough Sleeping, Statutory Homelessness
and Hidden Homelessness (Crisis 2018). Rough sleeping refers to the individuals sleeping
rough on the streets, Statutory Homelessness refers to individuals who lack a secure place to
live, while hidden homelessness refers to individuals who have not approached or divulged
their lack of home to the authorities, and hence have not been listed homeless. United Nations
describes ‘absolute homelessness’ as a condition arising due to a lack of physical shelter,
causing people to sleep outdoors, in vehicles, abandoned buildings, or places not intended for
human settlement, while describing ’relative homelessness’ who have physical shelters that
does not meet basic health and safety standards (Hwang 2018).
Homelessness in UK:
Reports from November, 2017 shows that as estimated 307,000 (one out of every 200
people) people sleeping rough or lack adequate housing in the UK, with London having the
highest number of homeless people, and increasing problems of homelessness in places like
Broxbourne, Luton and Chelmsford (Butler 2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3Homelessness as a public health risk
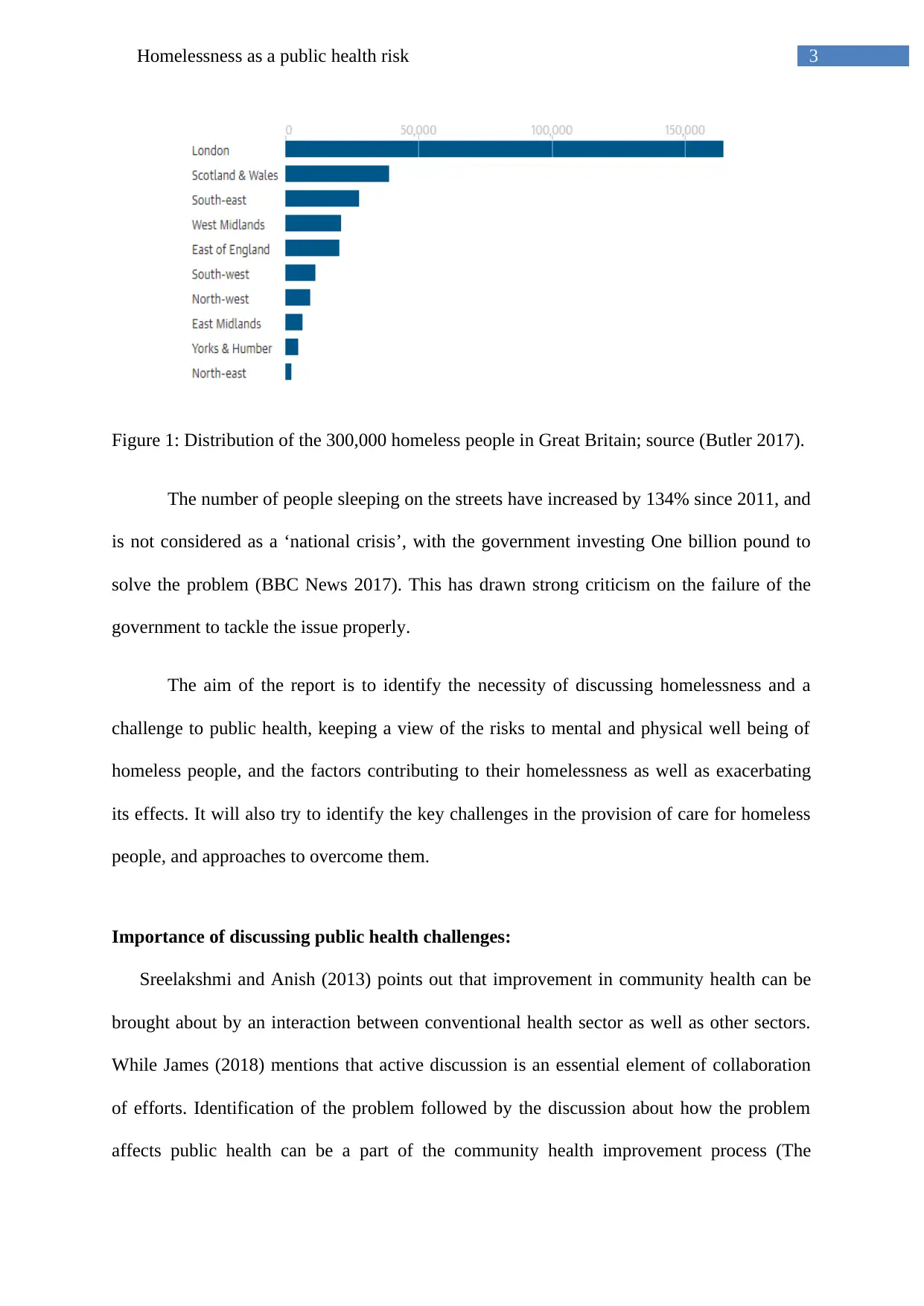
Figure 1: Distribution of the 300,000 homeless people in Great Britain; source (Butler 2017).
The number of people sleeping on the streets have increased by 134% since 2011, and
is not considered as a ‘national crisis’, with the government investing One billion pound to
solve the problem (BBC News 2017). This has drawn strong criticism on the failure of the
government to tackle the issue properly.
The aim of the report is to identify the necessity of discussing homelessness and a
challenge to public health, keeping a view of the risks to mental and physical well being of
homeless people, and the factors contributing to their homelessness as well as exacerbating
its effects. It will also try to identify the key challenges in the provision of care for homeless
people, and approaches to overcome them.
Importance of discussing public health challenges:
Sreelakshmi and Anish (2013) points out that improvement in community health can be
brought about by an interaction between conventional health sector as well as other sectors.
While James (2018) mentions that active discussion is an essential element of collaboration
of efforts. Identification of the problem followed by the discussion about how the problem
affects public health can be a part of the community health improvement process (The
Figure 1: Distribution of the 300,000 homeless people in Great Britain; source (Butler 2017).
The number of people sleeping on the streets have increased by 134% since 2011, and
is not considered as a ‘national crisis’, with the government investing One billion pound to
solve the problem (BBC News 2017). This has drawn strong criticism on the failure of the
government to tackle the issue properly.
The aim of the report is to identify the necessity of discussing homelessness and a
challenge to public health, keeping a view of the risks to mental and physical well being of
homeless people, and the factors contributing to their homelessness as well as exacerbating
its effects. It will also try to identify the key challenges in the provision of care for homeless
people, and approaches to overcome them.
Importance of discussing public health challenges:
Sreelakshmi and Anish (2013) points out that improvement in community health can be
brought about by an interaction between conventional health sector as well as other sectors.
While James (2018) mentions that active discussion is an essential element of collaboration
of efforts. Identification of the problem followed by the discussion about how the problem
affects public health can be a part of the community health improvement process (The
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4Homelessness as a public health risk
National Academics of Sciences, Engineering and Medicine 2018). Keeping in mind such
considerations, this report will discuss Homelessness as a public health challenge in the UK.
It has been pointed that homelessness can increase the risk for different types of chronic
and acute health conditions. Inter relation between health and homelessness can be
categorized into three types:
a) Health conditions that can lead to homelessness
b) Health conditions that can occur due to homelessness
c) Challenges in the treatment of homeless individuals
(Comittee on Health Care for Homeless People INSTITUTE OF MEDICINE 2018).
Kelly (1985) pointed out that the risk of health issues like skin disorder, or trauma can
be greatly increased due to homelessness, and can also cause a rapid deterioration of a minor
health condition into a serious one. Other health risks can include malnutrition, oral health
issues, parasitic infections, degenerative diseases, cirrhosis of liver, venereal disease,
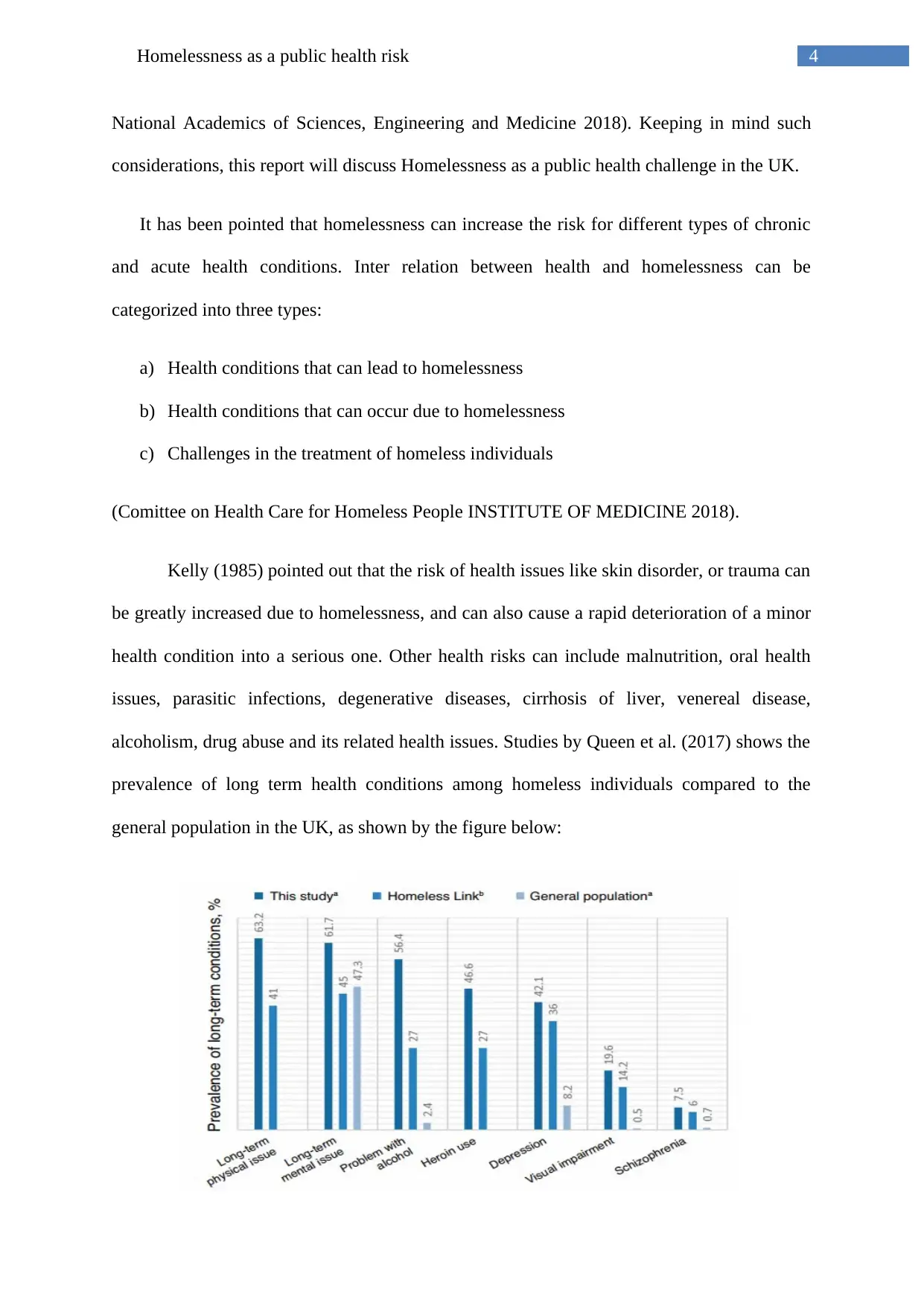
alcoholism, drug abuse and its related health issues. Studies by Queen et al. (2017) shows the
prevalence of long term health conditions among homeless individuals compared to the
general population in the UK, as shown by the figure below:
National Academics of Sciences, Engineering and Medicine 2018). Keeping in mind such
considerations, this report will discuss Homelessness as a public health challenge in the UK.
It has been pointed that homelessness can increase the risk for different types of chronic
and acute health conditions. Inter relation between health and homelessness can be
categorized into three types:
a) Health conditions that can lead to homelessness
b) Health conditions that can occur due to homelessness
c) Challenges in the treatment of homeless individuals
(Comittee on Health Care for Homeless People INSTITUTE OF MEDICINE 2018).
Kelly (1985) pointed out that the risk of health issues like skin disorder, or trauma can
be greatly increased due to homelessness, and can also cause a rapid deterioration of a minor
health condition into a serious one. Other health risks can include malnutrition, oral health
issues, parasitic infections, degenerative diseases, cirrhosis of liver, venereal disease,
alcoholism, drug abuse and its related health issues. Studies by Queen et al. (2017) shows the
prevalence of long term health conditions among homeless individuals compared to the
general population in the UK, as shown by the figure below:
5Homelessness as a public health risk
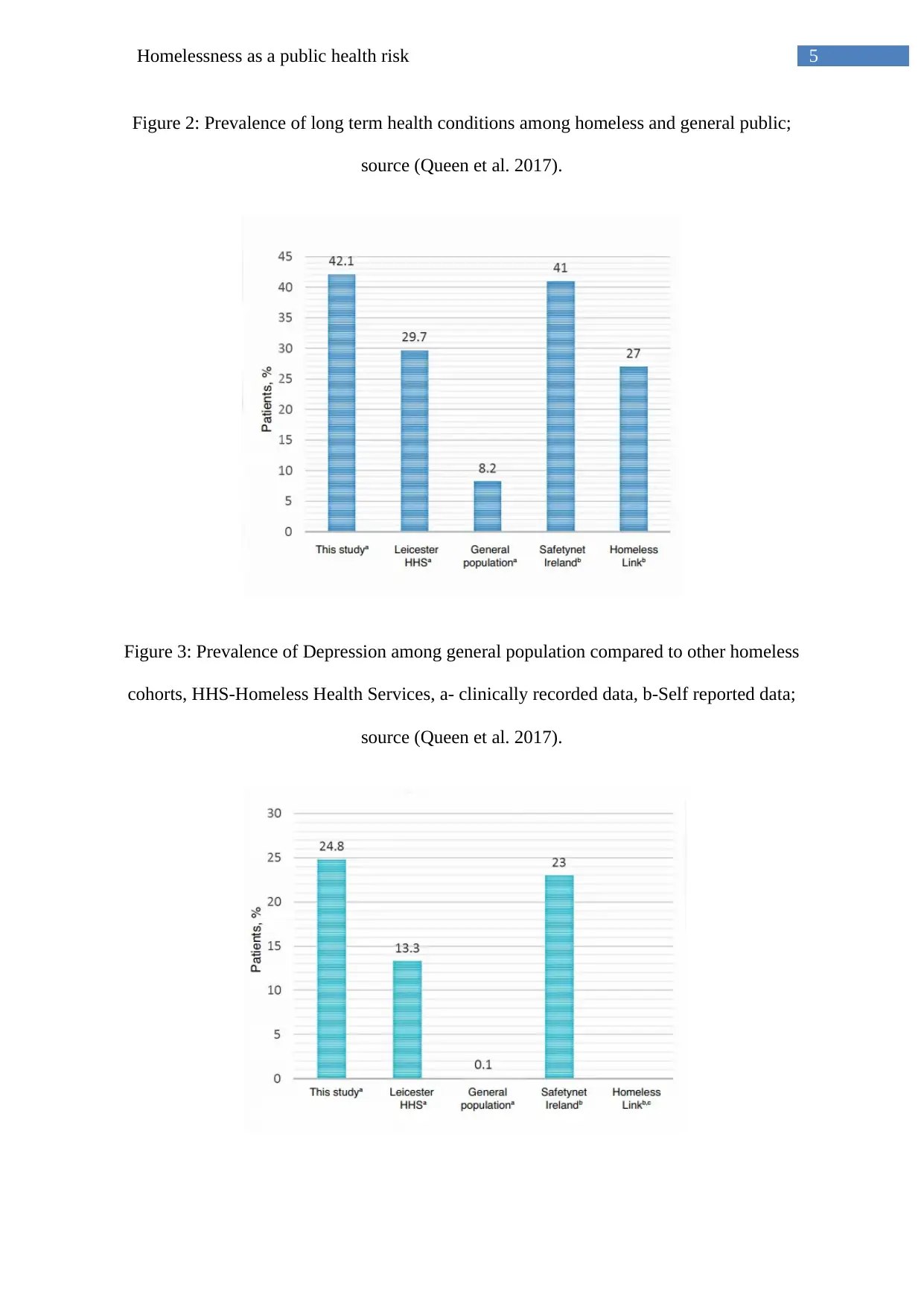
Figure 2: Prevalence of long term health conditions among homeless and general public;
source (Queen et al. 2017).
Figure 3: Prevalence of Depression among general population compared to other homeless
cohorts, HHS-Homeless Health Services, a- clinically recorded data, b-Self reported data;
source (Queen et al. 2017).
Figure 2: Prevalence of long term health conditions among homeless and general public;
source (Queen et al. 2017).
Figure 3: Prevalence of Depression among general population compared to other homeless
cohorts, HHS-Homeless Health Services, a- clinically recorded data, b-Self reported data;
source (Queen et al. 2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6Homelessness as a public health risk
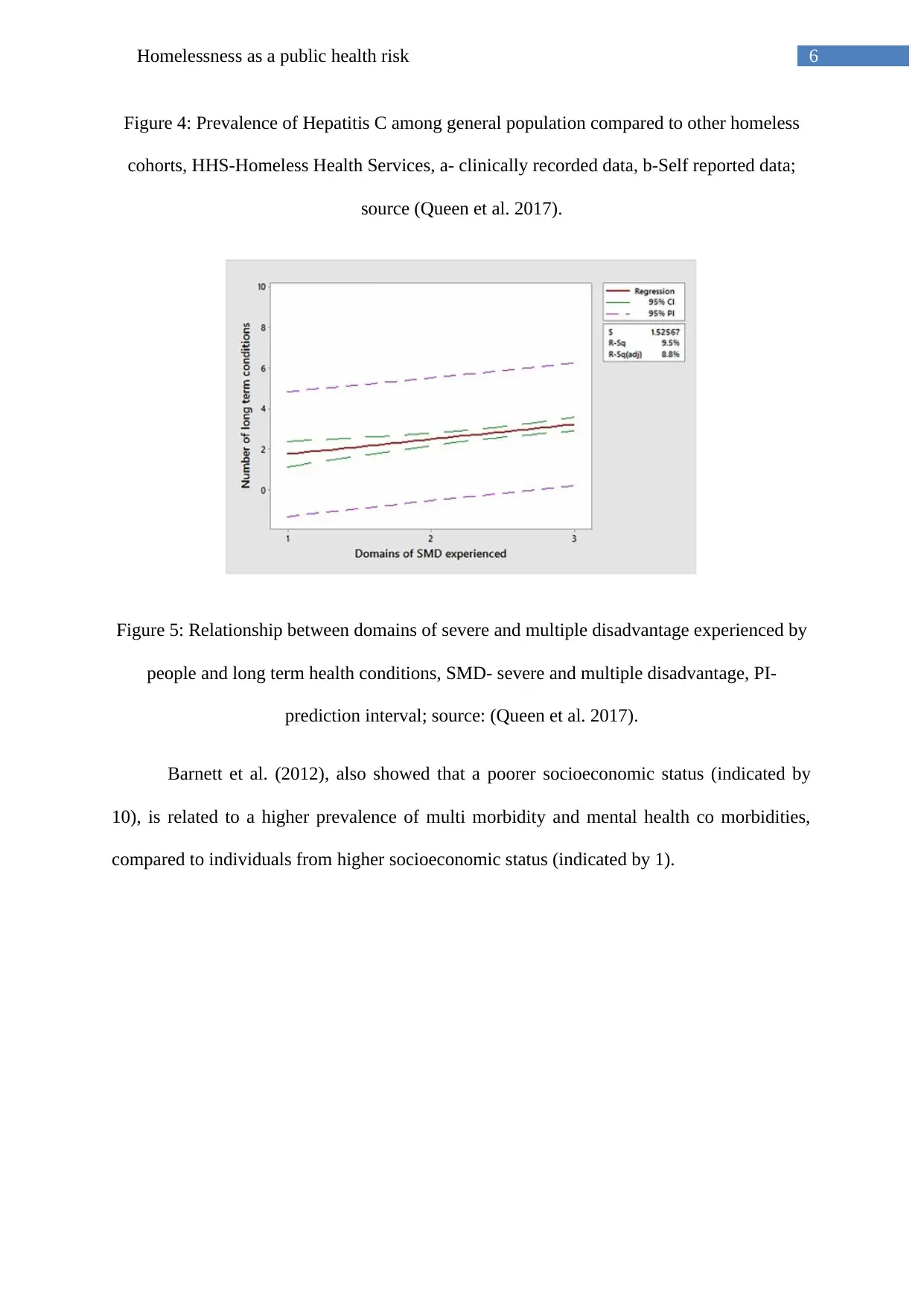
Figure 4: Prevalence of Hepatitis C among general population compared to other homeless
cohorts, HHS-Homeless Health Services, a- clinically recorded data, b-Self reported data;
source (Queen et al. 2017).
Figure 5: Relationship between domains of severe and multiple disadvantage experienced by
people and long term health conditions, SMD- severe and multiple disadvantage, PI-
prediction interval; source: (Queen et al. 2017).
Barnett et al. (2012), also showed that a poorer socioeconomic status (indicated by
10), is related to a higher prevalence of multi morbidity and mental health co morbidities,
compared to individuals from higher socioeconomic status (indicated by 1).
Figure 4: Prevalence of Hepatitis C among general population compared to other homeless
cohorts, HHS-Homeless Health Services, a- clinically recorded data, b-Self reported data;
source (Queen et al. 2017).
Figure 5: Relationship between domains of severe and multiple disadvantage experienced by
people and long term health conditions, SMD- severe and multiple disadvantage, PI-
prediction interval; source: (Queen et al. 2017).
Barnett et al. (2012), also showed that a poorer socioeconomic status (indicated by
10), is related to a higher prevalence of multi morbidity and mental health co morbidities,
compared to individuals from higher socioeconomic status (indicated by 1).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7Homelessness as a public health risk
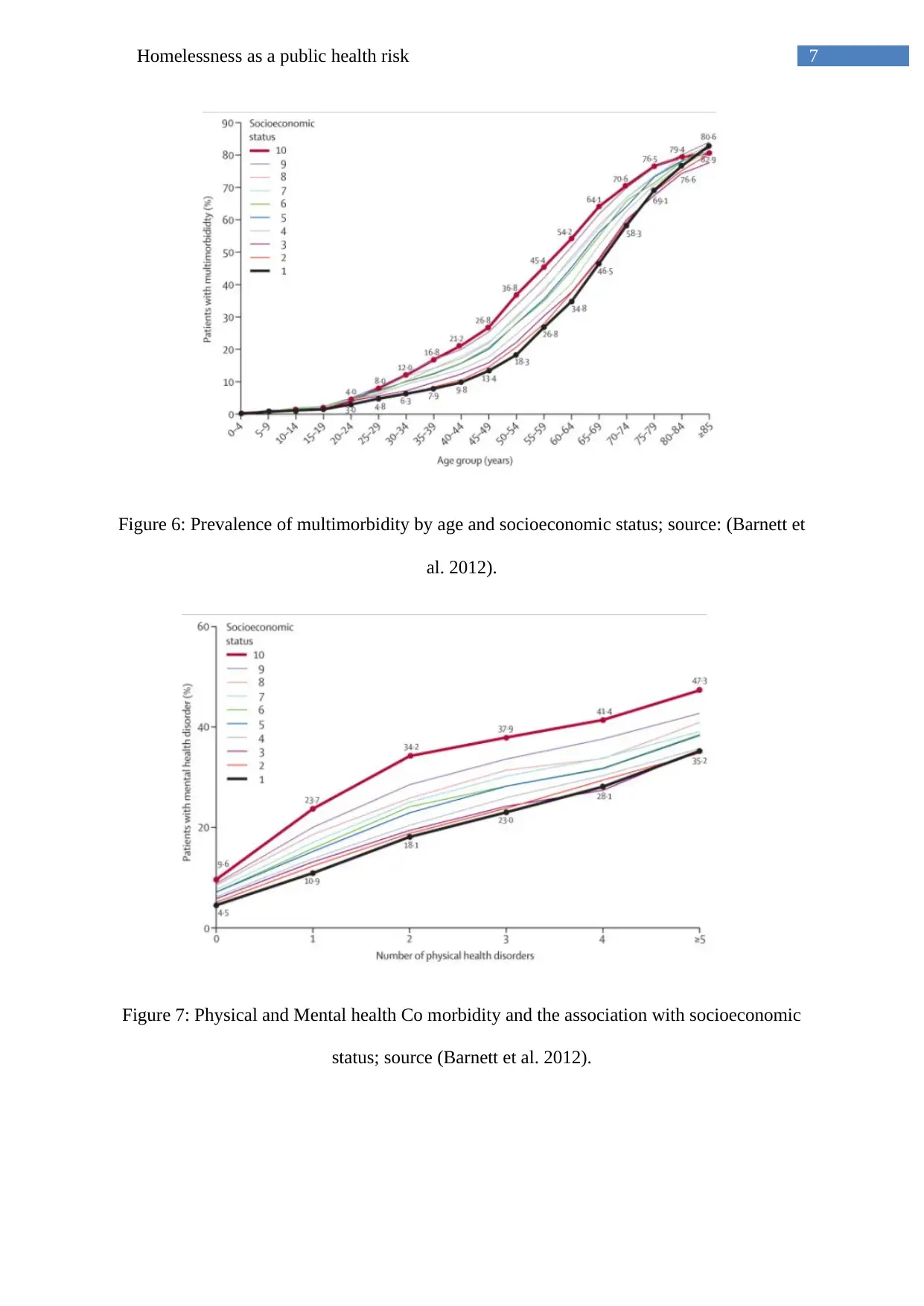
Figure 6: Prevalence of multimorbidity by age and socioeconomic status; source: (Barnett et
al. 2012).
Figure 7: Physical and Mental health Co morbidity and the association with socioeconomic
status; source (Barnett et al. 2012).
Figure 6: Prevalence of multimorbidity by age and socioeconomic status; source: (Barnett et
al. 2012).
Figure 7: Physical and Mental health Co morbidity and the association with socioeconomic
status; source (Barnett et al. 2012).
8Homelessness as a public health risk
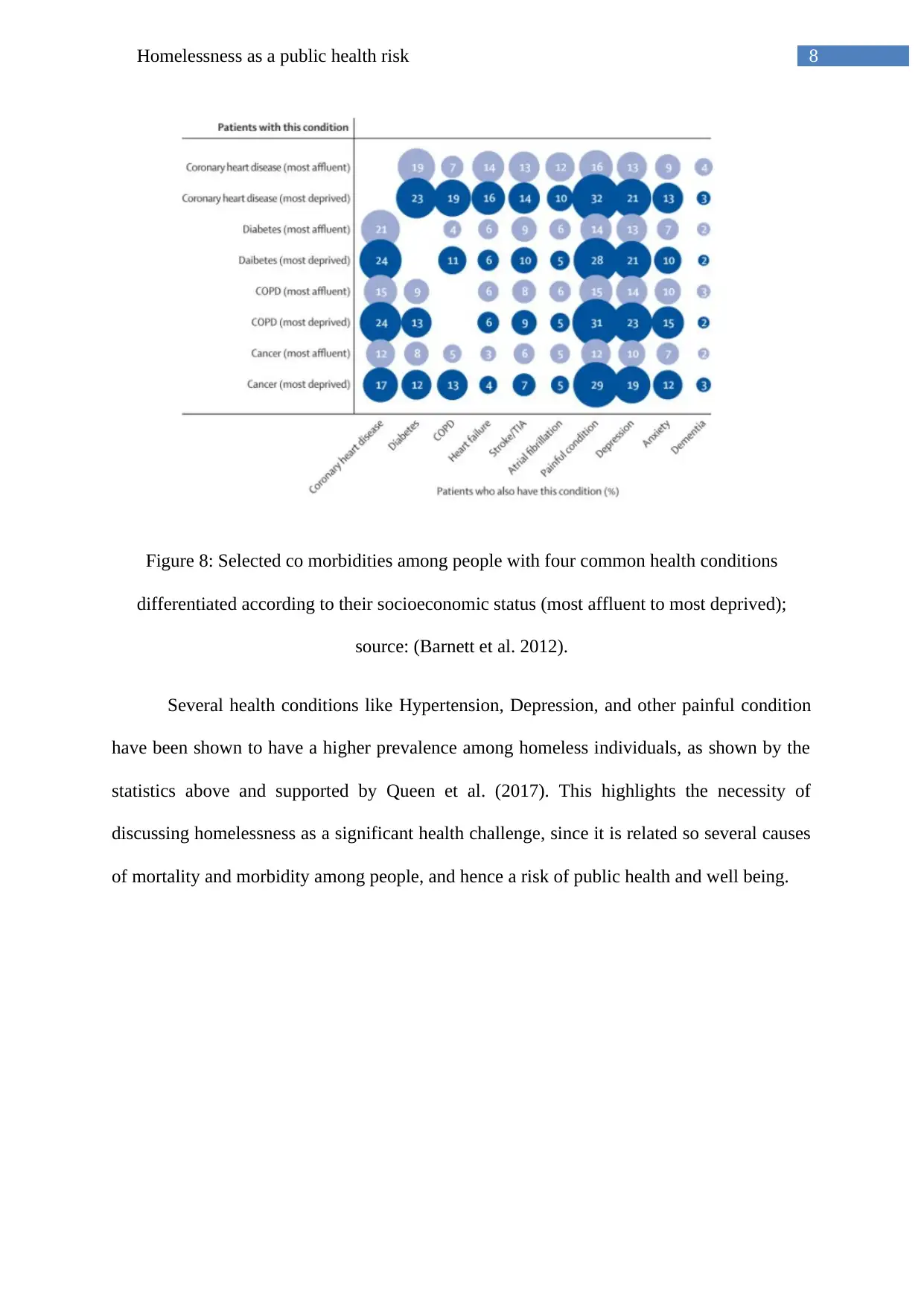
Figure 8: Selected co morbidities among people with four common health conditions
differentiated according to their socioeconomic status (most affluent to most deprived);
source: (Barnett et al. 2012).
Several health conditions like Hypertension, Depression, and other painful condition
have been shown to have a higher prevalence among homeless individuals, as shown by the
statistics above and supported by Queen et al. (2017). This highlights the necessity of
discussing homelessness as a significant health challenge, since it is related so several causes
of mortality and morbidity among people, and hence a risk of public health and well being.
Figure 8: Selected co morbidities among people with four common health conditions
differentiated according to their socioeconomic status (most affluent to most deprived);
source: (Barnett et al. 2012).
Several health conditions like Hypertension, Depression, and other painful condition
have been shown to have a higher prevalence among homeless individuals, as shown by the
statistics above and supported by Queen et al. (2017). This highlights the necessity of
discussing homelessness as a significant health challenge, since it is related so several causes
of mortality and morbidity among people, and hence a risk of public health and well being.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9Homelessness as a public health risk
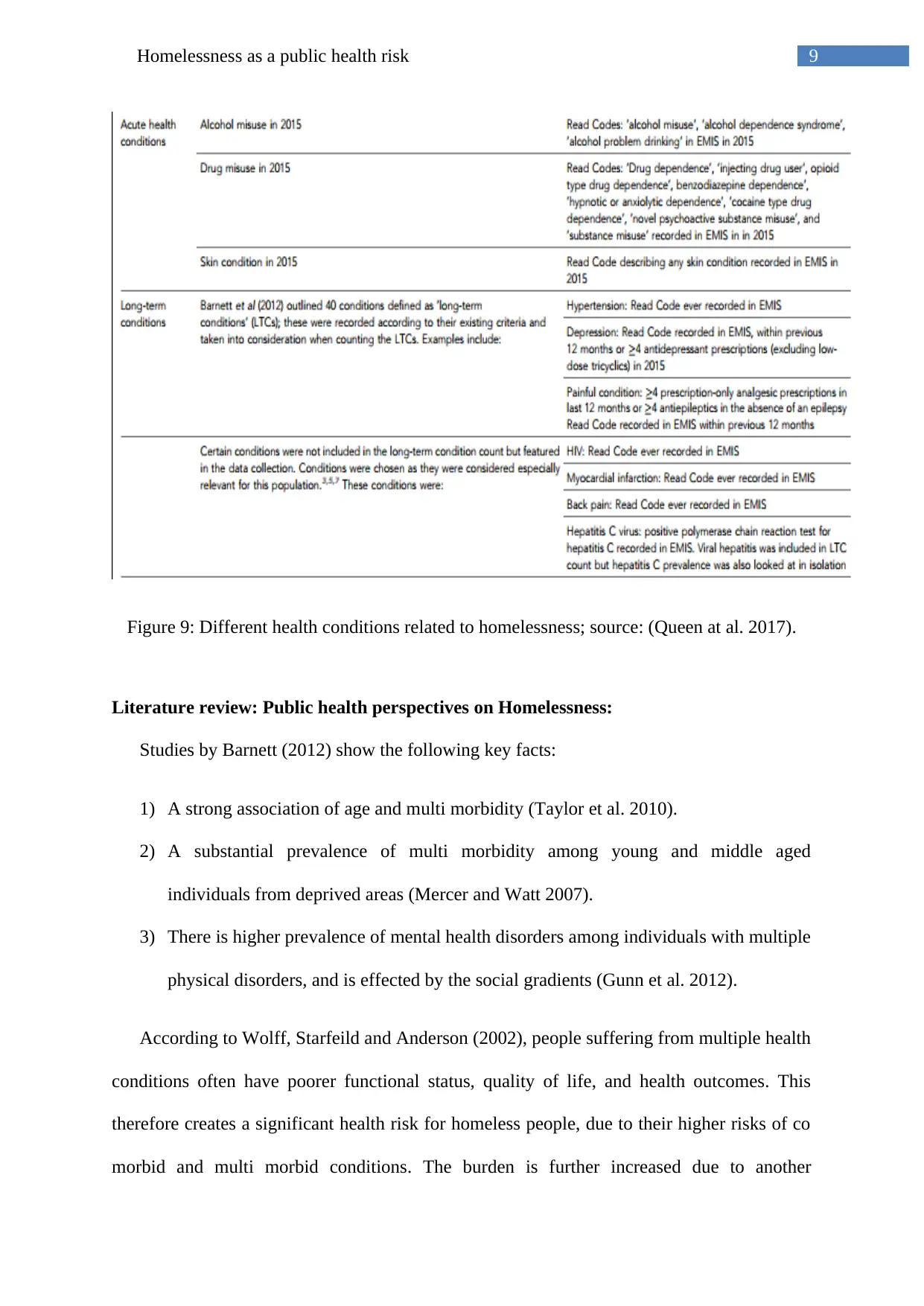
Figure 9: Different health conditions related to homelessness; source: (Queen at al. 2017).
Literature review: Public health perspectives on Homelessness:
Studies by Barnett (2012) show the following key facts:
1) A strong association of age and multi morbidity (Taylor et al. 2010).
2) A substantial prevalence of multi morbidity among young and middle aged
individuals from deprived areas (Mercer and Watt 2007).
3) There is higher prevalence of mental health disorders among individuals with multiple
physical disorders, and is effected by the social gradients (Gunn et al. 2012).
According to Wolff, Starfeild and Anderson (2002), people suffering from multiple health
conditions often have poorer functional status, quality of life, and health outcomes. This
therefore creates a significant health risk for homeless people, due to their higher risks of co
morbid and multi morbid conditions. The burden is further increased due to another
Figure 9: Different health conditions related to homelessness; source: (Queen at al. 2017).
Literature review: Public health perspectives on Homelessness:
Studies by Barnett (2012) show the following key facts:
1) A strong association of age and multi morbidity (Taylor et al. 2010).
2) A substantial prevalence of multi morbidity among young and middle aged
individuals from deprived areas (Mercer and Watt 2007).
3) There is higher prevalence of mental health disorders among individuals with multiple
physical disorders, and is effected by the social gradients (Gunn et al. 2012).
According to Wolff, Starfeild and Anderson (2002), people suffering from multiple health
conditions often have poorer functional status, quality of life, and health outcomes. This
therefore creates a significant health risk for homeless people, due to their higher risks of co
morbid and multi morbid conditions. The burden is further increased due to another
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10Homelessness as a public health risk
significant challenge of the provision of care for the homeless individuals (Comittee on
Health Care for Homeless People INSTITUTE OF MEDICINE 2018). For example,
treatment of diseases like Diabetes, which requires daily injections of insulin, which needs
refrigeration, and specialized diets, both of which are hard to be availed by a homeless
person. Also, the lack of health insurance among homeless individuals makes them unable to
afford any or most forms of treatment in case of emergencies, further increasing the risks of
morbidity or mortality. Poverty is one of the crucial factors that lead to homelessness, and
studies have shown that poverty can have strong causal effect on both mental and physical
health of individuals (Marmot 2015). Bramley et al. (2015) also adds that poverty is also
related to the emergence of spatial concentration of drug abuse, and chronic offenses.
Studies by Woliski, Kidder and Fenton (2007) also showed the increased risks of HIV
AIDS among homeless individuals are found to be three to nine times higher among
homeless individuals compared to the general public (Allen et al. 1994; Culhane et al. 2001;
Estebanez et al. 2000). The prevalence of HIV adds to the health risks of the homeless
individuals as well as being a significant public health concern, due to its communicable
nature.
Kennedy (2007) pointed out that homelessness increases the incidence of exposure to
violence and lower rate of social support, also causing a negative attitude towards schooling
or participation in schools. This further reduces their chances of employability and therefore
affects their socioeconomic status. The increased exposure to violence can also cause mental
health issues, and even give rise to violent, erratic or deviant behaviour, which also can be a
significant concern for public well being. Mental health issues and violence are also
interrelated, as per several studies (Rogers and Pilgrim 2014). This view is supported by Tsai
et al. (2015) who pointed out that exposure to violence increases the psychological
significant challenge of the provision of care for the homeless individuals (Comittee on
Health Care for Homeless People INSTITUTE OF MEDICINE 2018). For example,
treatment of diseases like Diabetes, which requires daily injections of insulin, which needs
refrigeration, and specialized diets, both of which are hard to be availed by a homeless
person. Also, the lack of health insurance among homeless individuals makes them unable to
afford any or most forms of treatment in case of emergencies, further increasing the risks of
morbidity or mortality. Poverty is one of the crucial factors that lead to homelessness, and
studies have shown that poverty can have strong causal effect on both mental and physical
health of individuals (Marmot 2015). Bramley et al. (2015) also adds that poverty is also
related to the emergence of spatial concentration of drug abuse, and chronic offenses.
Studies by Woliski, Kidder and Fenton (2007) also showed the increased risks of HIV
AIDS among homeless individuals are found to be three to nine times higher among
homeless individuals compared to the general public (Allen et al. 1994; Culhane et al. 2001;
Estebanez et al. 2000). The prevalence of HIV adds to the health risks of the homeless
individuals as well as being a significant public health concern, due to its communicable
nature.
Kennedy (2007) pointed out that homelessness increases the incidence of exposure to
violence and lower rate of social support, also causing a negative attitude towards schooling
or participation in schools. This further reduces their chances of employability and therefore
affects their socioeconomic status. The increased exposure to violence can also cause mental
health issues, and even give rise to violent, erratic or deviant behaviour, which also can be a
significant concern for public well being. Mental health issues and violence are also
interrelated, as per several studies (Rogers and Pilgrim 2014). This view is supported by Tsai
et al. (2015) who pointed out that exposure to violence increases the psychological
11Homelessness as a public health risk
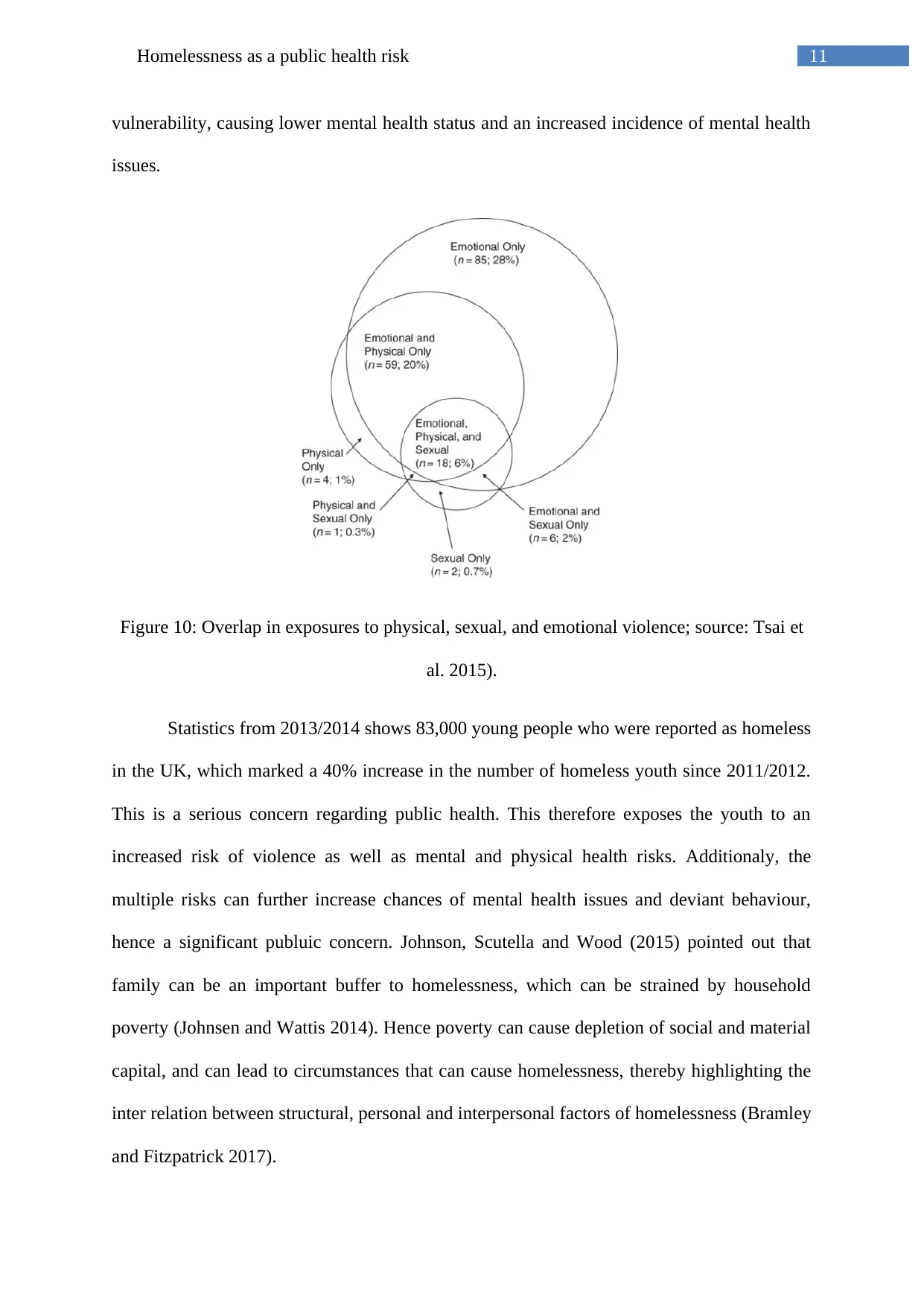
vulnerability, causing lower mental health status and an increased incidence of mental health
issues.
Figure 10: Overlap in exposures to physical, sexual, and emotional violence; source: Tsai et
al. 2015).
Statistics from 2013/2014 shows 83,000 young people who were reported as homeless
in the UK, which marked a 40% increase in the number of homeless youth since 2011/2012.
This is a serious concern regarding public health. This therefore exposes the youth to an
increased risk of violence as well as mental and physical health risks. Additionaly, the
multiple risks can further increase chances of mental health issues and deviant behaviour,
hence a significant publuic concern. Johnson, Scutella and Wood (2015) pointed out that
family can be an important buffer to homelessness, which can be strained by household
poverty (Johnsen and Wattis 2014). Hence poverty can cause depletion of social and material
capital, and can lead to circumstances that can cause homelessness, thereby highlighting the
inter relation between structural, personal and interpersonal factors of homelessness (Bramley
and Fitzpatrick 2017).
vulnerability, causing lower mental health status and an increased incidence of mental health
issues.
Figure 10: Overlap in exposures to physical, sexual, and emotional violence; source: Tsai et
al. 2015).
Statistics from 2013/2014 shows 83,000 young people who were reported as homeless
in the UK, which marked a 40% increase in the number of homeless youth since 2011/2012.
This is a serious concern regarding public health. This therefore exposes the youth to an
increased risk of violence as well as mental and physical health risks. Additionaly, the
multiple risks can further increase chances of mental health issues and deviant behaviour,
hence a significant publuic concern. Johnson, Scutella and Wood (2015) pointed out that
family can be an important buffer to homelessness, which can be strained by household
poverty (Johnsen and Wattis 2014). Hence poverty can cause depletion of social and material
capital, and can lead to circumstances that can cause homelessness, thereby highlighting the
inter relation between structural, personal and interpersonal factors of homelessness (Bramley
and Fitzpatrick 2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 26
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.