Case Study: Analysis of SOAP Note for Hypertension Management
VerifiedAdded on 2022/09/27
|5
|960
|25
Case Study
AI Summary
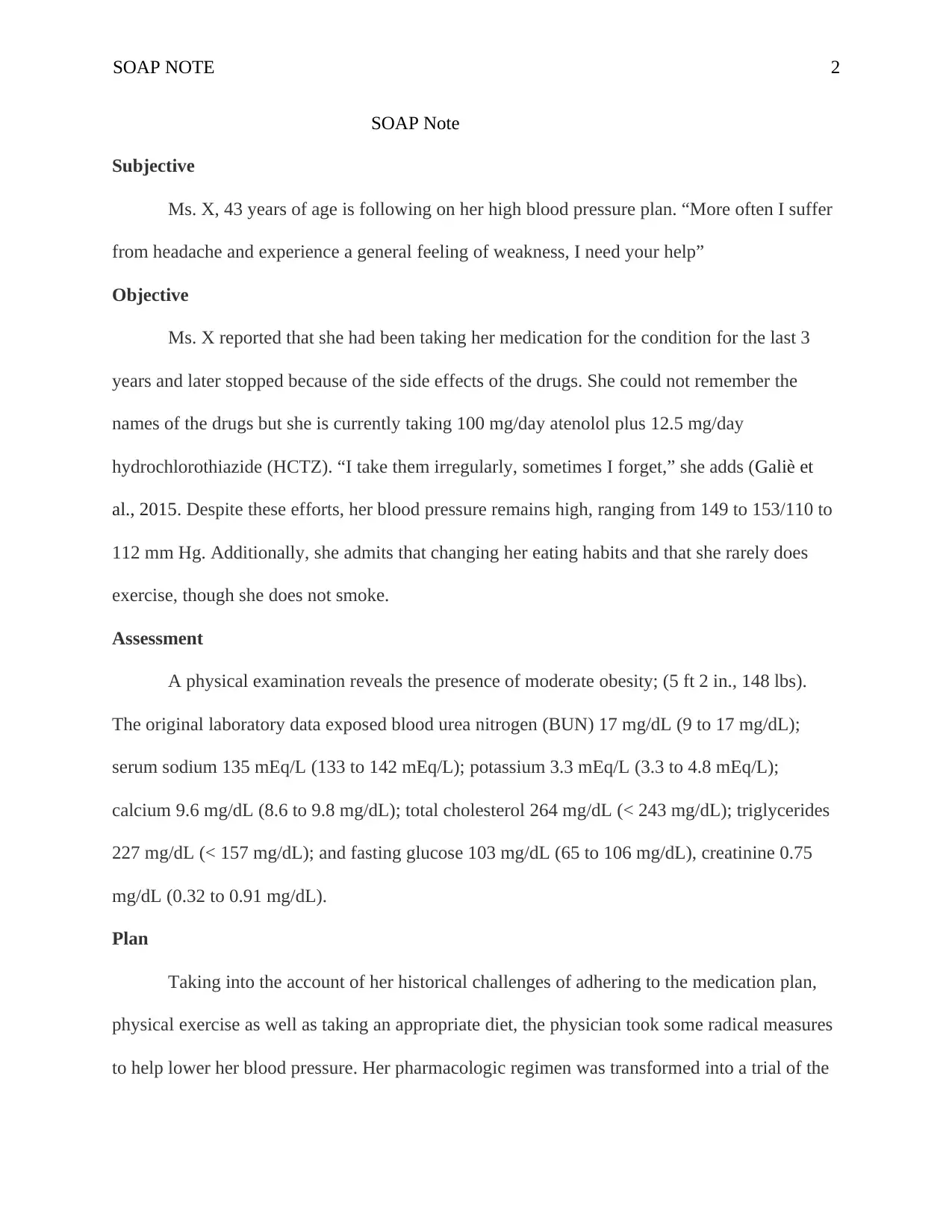
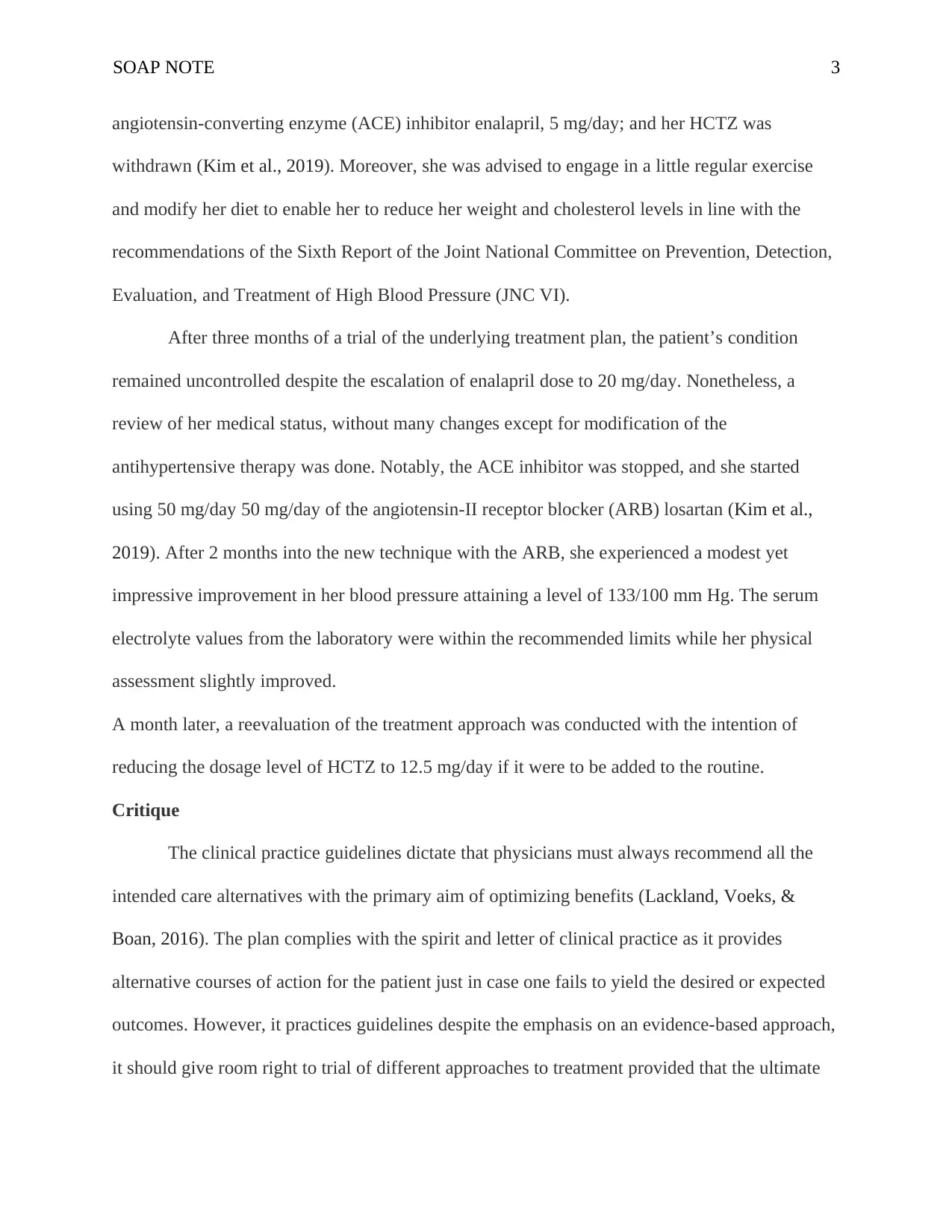
This case study presents a SOAP note for a 43-year-old female, Ms. X, managing hypertension. The subjective section details her symptoms (headaches, weakness) and medication history (atenolol and hydrochlorothiazide). The objective section reveals high blood pressure readings and lab results, including elevated cholesterol and triglycerides. The assessment identifies moderate obesity. The plan involves transitioning her pharmacologic regimen, first to enalapril and then to losartan, along with lifestyle recommendations (exercise, diet). After the initial treatment plan failed, the ARB was started with positive results. The critique highlights adherence to clinical practice guidelines, emphasizing the importance of considering alternative treatment options to improve patient outcomes. References to supporting research on hypertension management are also provided.


1 out of 5
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.