Case Study: Hypoglycemia Assessment, Pathophysiology, and Care Plan
VerifiedAdded on 2023/06/10
|20
|3444
|355
Case Study
AI Summary
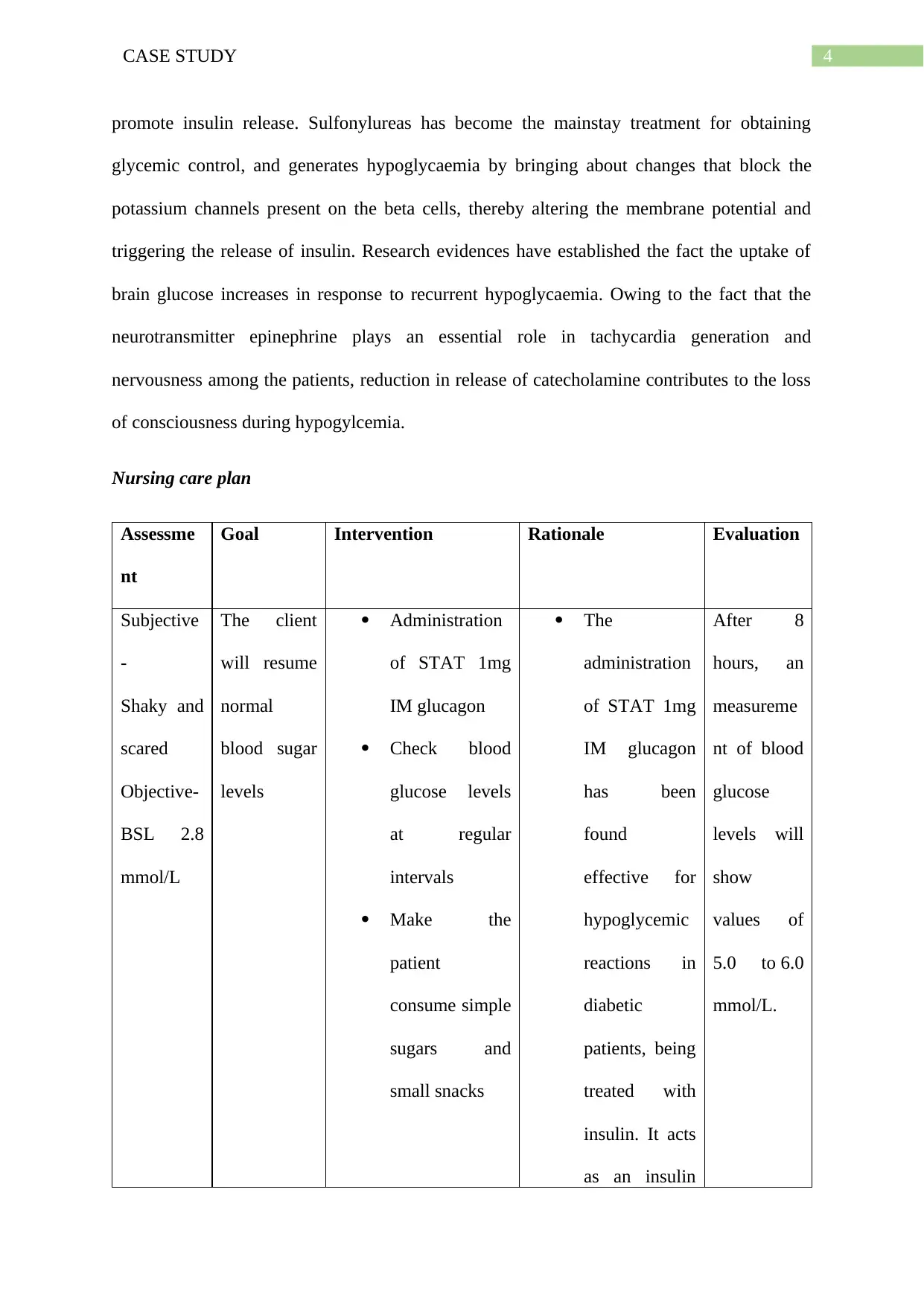
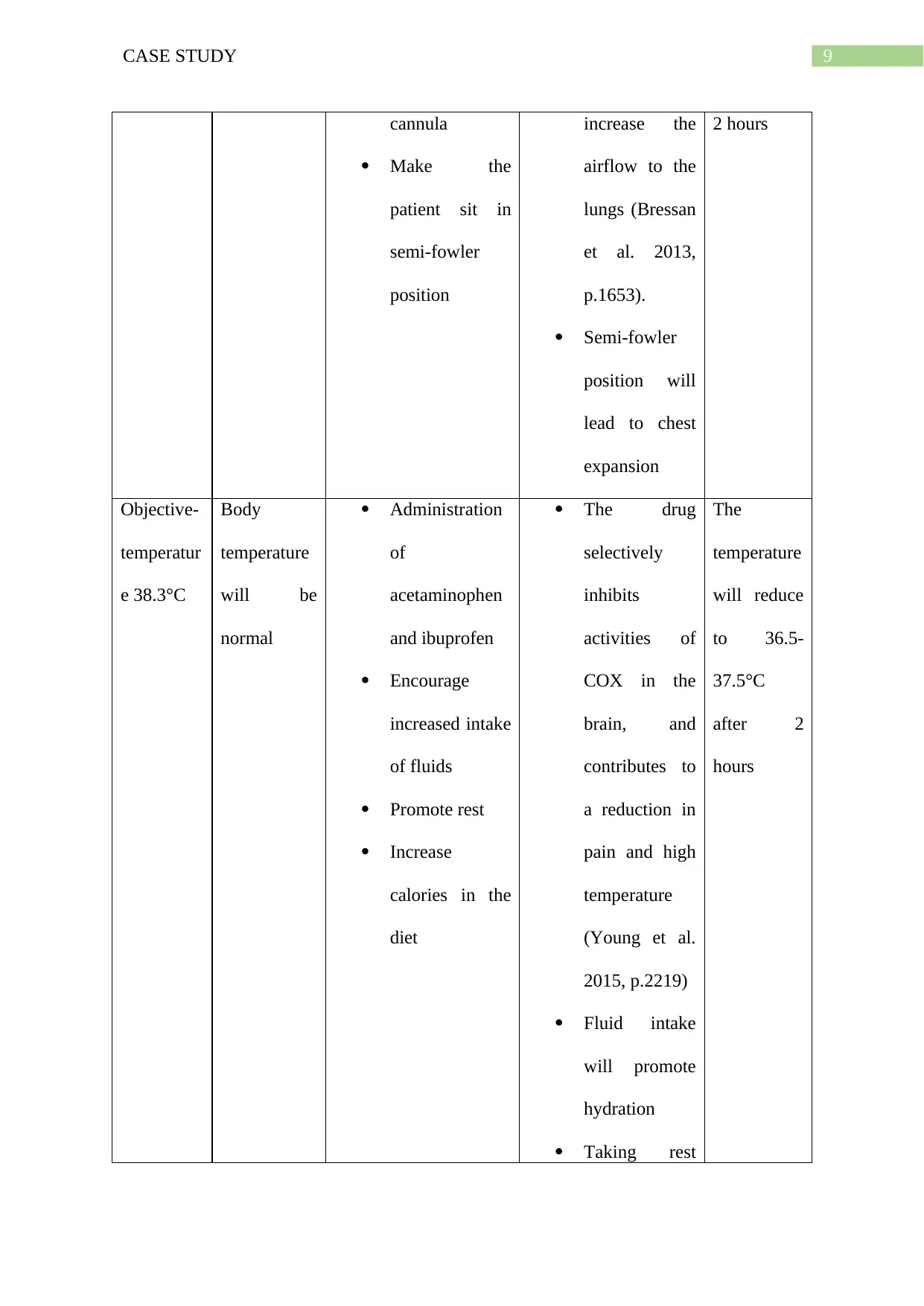
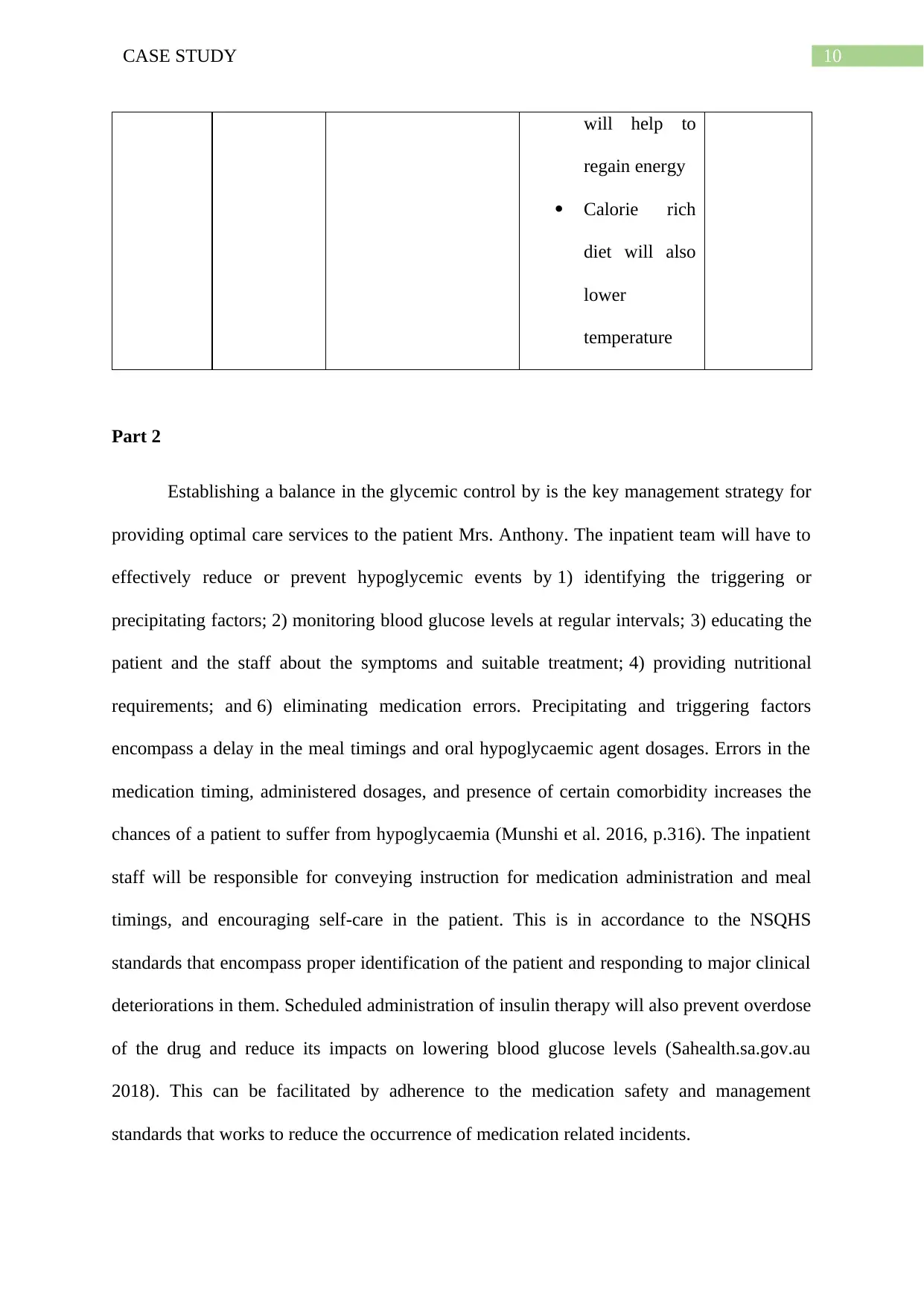
This case study focuses on Mrs. Anthony, a 35-year-old patient admitted to the emergency department with multiple fractures, loss of consciousness, and smoke inhalation. The case details her type 2 diabetes diagnosis and presenting symptoms, including hypotension, tachycardia, hypoxemia, and a low blood glucose level of 2.8 mmol/L, indicating hypoglycemia. The assignment explores the pathophysiology of hypoglycemia, explaining how insufficient glucose impacts brain function and triggers hormonal and metabolic responses. It also outlines a comprehensive nursing care plan, including assessment, interventions such as glucagon administration and oxygen therapy, and rationales for each intervention, aiming to restore blood glucose levels, improve vital signs, and address the patient's various symptoms. The essay also highlights the importance of glycemic control, identifying precipitating factors, regular blood glucose monitoring, patient education, and medication safety to prevent future hypoglycemic events. The case study emphasizes the need for a multidisciplinary approach and the importance of patient and family education for effective self-management of glucose levels.

1 out of 20
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.