Intracerebral Hemorrhagic Stroke: Case Study Analysis, Treatment
VerifiedAdded on 2022/08/22
|6
|1674
|55
Case Study
AI Summary
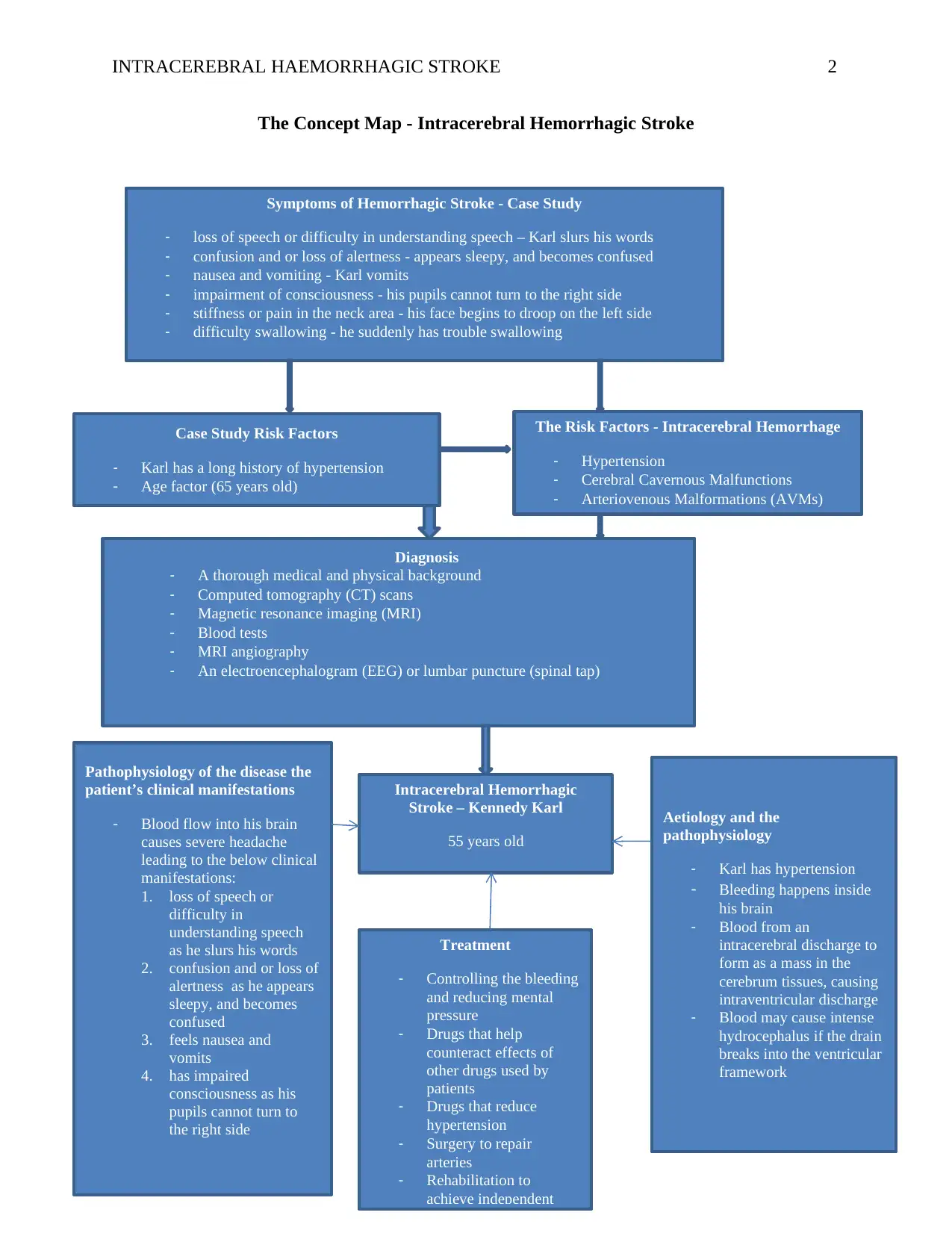
This case study focuses on an intracerebral hemorrhagic stroke (ICH) experienced by a 65-year-old patient, Karl Kennedy, with a history of hypertension. The assignment analyzes the patient's symptoms, including loss of speech, confusion, nausea, and impaired consciousness, linking them to the pathophysiology of ICH. The document explores the risk factors, aetiology, and the step-by-step sequence between aetiology and pathophysiology. It details the diagnostic investigations, such as CT scans and MRIs, and discusses treatment modalities aimed at controlling bleeding, reducing pressure, and rehabilitation. The analysis emphasizes the importance of early diagnosis and intervention in managing this medical emergency. The paper also highlights the role of hypertension and age as key risk factors and the potential for complications such as hydrocephalus and herniation. The student provides a comprehensive overview of the case, supported by evidence-based literature.

1 out of 6
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.