Implementing and Monitoring Nursing Care: Assessment 1 (HLTEN512B)
VerifiedAdded on 2020/05/28
|10
|2391
|102
Homework Assignment
AI Summary
This assignment, addressing HLTEN512B, focuses on implementing and monitoring nursing care for clients with acute health problems. It covers several key areas, including the core duties of nurses like confidentiality, duty of care, patient advocacy, and the nurses codes of ethics. The assignment explores the nursing care of patients with conditions such as severe burns and hemorrhage. It also provides details on preoperative assessments, including identifying comorbidities that can contribute to surgical complications. The assignment also covers the use of local anesthetics and sedatives, and the importance of postoperative care, including medication administration and monitoring. Finally, it examines the management of various complications and provides guidance on patient education regarding potential issues and necessary actions. The assignment is supported by a list of relevant references.

Running head: ASSESSMENT 1 (QUESTIONING)
HLTEN512B Implement and monitor nursing care for clients with acute health problems
Name of the Student
Name of the University
Author Note
HLTEN512B Implement and monitor nursing care for clients with acute health problems
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1ASSESSMENT 1 (QUESTIONING)
Answer 1
a. Confidentiality
It is considered as the core duty of medical practice, which requires all healthcare
professionals to keep the personal health information of their patient as private unless they
provide their consent to disclose it (Griffith, 2015). Confidentiality forms the foundation of an
effective nurse-client relationship.
b. Duty of care
It refers to the legal obligation of health organizations and professionals to avoid acts that
can likely cause harm to their patients. It requires strict adherence to providing reasonable care, a
deviation from which can result in negligence and adverse effects (Cornock, 2014).
c. Advocacy
Patient advocacy refers to certain activities by the patient, family members, and friends
that can influence the decision of the carers and physicians, regarding implementation of
therapeutic interventions. It encompasses patient rights, confidentiality, support, education, and
privacy (Cole, Wellard & Mummery, 2014).
d. Public liability
This part of the law focuses on civil misdoings based on which an applicant can sue the
respondent due to the latter’s negligence, by utilizing the provisions of the common law (Yang &
Silverman, 2014).
NAME- | STUDENT ID-
Answer 1
a. Confidentiality
It is considered as the core duty of medical practice, which requires all healthcare
professionals to keep the personal health information of their patient as private unless they
provide their consent to disclose it (Griffith, 2015). Confidentiality forms the foundation of an
effective nurse-client relationship.
b. Duty of care
It refers to the legal obligation of health organizations and professionals to avoid acts that
can likely cause harm to their patients. It requires strict adherence to providing reasonable care, a
deviation from which can result in negligence and adverse effects (Cornock, 2014).
c. Advocacy
Patient advocacy refers to certain activities by the patient, family members, and friends
that can influence the decision of the carers and physicians, regarding implementation of
therapeutic interventions. It encompasses patient rights, confidentiality, support, education, and
privacy (Cole, Wellard & Mummery, 2014).
d. Public liability
This part of the law focuses on civil misdoings based on which an applicant can sue the
respondent due to the latter’s negligence, by utilizing the provisions of the common law (Yang &
Silverman, 2014).
NAME- | STUDENT ID-
2ASSESSMENT 1 (QUESTIONING)
e. Nurses Codes of Ethics (NMBA)
This Code of Ethics encompasses several domains namely, clinical, education,
management, and research and has been formulated for nurses working in Australia. The primary
aim of the code is making an outline of the commitment of nurses that is aimed towards
promoting, respecting, protecting and upholding the fundamental rights of the service users.
Thus, these codes help in identification of the fundamental standards of ethics and values and act
as a reference point for nurses to reflect on their practice (NMBA, 2008).
Answer 2
a. Severe burns
Upon admission to the ED, an initial assessment of the cardiovascular and respiratory
status should be performed. Minor burns should be cooled with sterile saline dipped towels. The
EN should wrap the fingers and toes of the patients individually with fluffed gauze. Open blisters
should be debrided and the tetanus status should be checked (Rowan et al., 2015). Severe or
third-degree burns often require intensive treatment such as, antibiotic prophylaxis that will
prevent infection from the burn wound. Gentamycin Prophylaxis 2mg/kg IV at a dose of 20mg,
1g flucolaxacillin IV stat plus can be used by the EN for manipulation of the wounds.
Furthermore, the patients should receive ≥ 30-40 mL/h fluid resuscitation based on the TBSA
percentage and inhalation injury (Borra et al., 2016).
b. Hemorrhage and shock
The primary treatment should be based on maximizing oxygen delivery of the patient by
ensuring the presence of adequate ventilation, restoration of blood flow and increasing the
NAME- | STUDENT ID-
e. Nurses Codes of Ethics (NMBA)
This Code of Ethics encompasses several domains namely, clinical, education,
management, and research and has been formulated for nurses working in Australia. The primary
aim of the code is making an outline of the commitment of nurses that is aimed towards
promoting, respecting, protecting and upholding the fundamental rights of the service users.
Thus, these codes help in identification of the fundamental standards of ethics and values and act
as a reference point for nurses to reflect on their practice (NMBA, 2008).
Answer 2
a. Severe burns
Upon admission to the ED, an initial assessment of the cardiovascular and respiratory
status should be performed. Minor burns should be cooled with sterile saline dipped towels. The
EN should wrap the fingers and toes of the patients individually with fluffed gauze. Open blisters
should be debrided and the tetanus status should be checked (Rowan et al., 2015). Severe or
third-degree burns often require intensive treatment such as, antibiotic prophylaxis that will
prevent infection from the burn wound. Gentamycin Prophylaxis 2mg/kg IV at a dose of 20mg,
1g flucolaxacillin IV stat plus can be used by the EN for manipulation of the wounds.
Furthermore, the patients should receive ≥ 30-40 mL/h fluid resuscitation based on the TBSA
percentage and inhalation injury (Borra et al., 2016).
b. Hemorrhage and shock
The primary treatment should be based on maximizing oxygen delivery of the patient by
ensuring the presence of adequate ventilation, restoration of blood flow and increasing the
NAME- | STUDENT ID-
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3ASSESSMENT 1 (QUESTIONING)
amount of oxygen saturation. Arterial line placement will help in continuous monitoring of blood
pressure. Resuscitative strategies can also be employed (Bouglé, Harrois & Duranteau, 2013).
Lactated ringer solution (1-2 L) can be used for initial fluid resuscitation (Rohrig et al., 2012).
Further blood loss should be controlled by administration of H2 blockers and vasopressin.
Answer 3
It refers to identification of co-morbidities that may contribute to complications during
surgical, anesthetic or post-operative period. The general examination involves identification of
abnormalities in the following system:
Abnormal breath sounds
Abdominal masses and previous scars in gastrointestinal system
Skeletal malformations like kyphoscoliosis (Chow et al., 2012)
Local skin irritation
Heart murmur
Presence of obesity
Presence of small mouth and short neck (Oresanya, Lyons & Finlayson, 2014)
Swelling of soft tissue at back of mouth
These preoperative assessments dectrease length of hospitalization and minimizing rates of
cancelled surgeries.
NAME- | STUDENT ID-
amount of oxygen saturation. Arterial line placement will help in continuous monitoring of blood
pressure. Resuscitative strategies can also be employed (Bouglé, Harrois & Duranteau, 2013).
Lactated ringer solution (1-2 L) can be used for initial fluid resuscitation (Rohrig et al., 2012).
Further blood loss should be controlled by administration of H2 blockers and vasopressin.
Answer 3
It refers to identification of co-morbidities that may contribute to complications during
surgical, anesthetic or post-operative period. The general examination involves identification of
abnormalities in the following system:
Abnormal breath sounds
Abdominal masses and previous scars in gastrointestinal system
Skeletal malformations like kyphoscoliosis (Chow et al., 2012)
Local skin irritation
Heart murmur
Presence of obesity
Presence of small mouth and short neck (Oresanya, Lyons & Finlayson, 2014)
Swelling of soft tissue at back of mouth
These preoperative assessments dectrease length of hospitalization and minimizing rates of
cancelled surgeries.
NAME- | STUDENT ID-
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4ASSESSMENT 1 (QUESTIONING)
Answer 4
A local anaesthetic agent can be administered at the surgical site for anesthetizing the
nerve endings and preventing pain sensation in the patient. It will help in sensation loss at
a small and specific area of the body (Ogle & Mahjoubi, 2012). The patient may also be
administered sedatives to provide relief from pain and reduce anxiety (anxiolysis).
Anticoagulants can also be administered in order to reduce the risk of blood clots and
heart attacks. These agents will seal the wounds and stop bleeding from the sites.
Warfarin or Rivaroxaban are most commonly applied (Chitsike et al., 2012).
Answer 5
Postoperative care begins at the end of an operation and continues throughout the
hospitalization period as well in the outpatient period. It involves the following:
The patients are extubated before they leave the operation theatre and secretions from the
airway are cleared.
Opiods are administered orally or patenterally for relieving pain. This also prevents
constipation (Stephens & Whitman, 2015).
Mental status is assessed. Fluid and electrolyte imbalances are restored.
Wound sites are checked twice regularly after removing operative dressing. Drain tubes
are monitored for the collected fluid.
Decrease risks of deep venous thrombosis.
Urine output is monitored. Catheters are used for patients with distended bladder.
Patients are made to sit up on their beds and are made to perform mild exercise to prevent
onset of sarcopenia (Nelson et al., 2016).
NAME- | STUDENT ID-
Answer 4
A local anaesthetic agent can be administered at the surgical site for anesthetizing the
nerve endings and preventing pain sensation in the patient. It will help in sensation loss at
a small and specific area of the body (Ogle & Mahjoubi, 2012). The patient may also be
administered sedatives to provide relief from pain and reduce anxiety (anxiolysis).
Anticoagulants can also be administered in order to reduce the risk of blood clots and
heart attacks. These agents will seal the wounds and stop bleeding from the sites.
Warfarin or Rivaroxaban are most commonly applied (Chitsike et al., 2012).
Answer 5
Postoperative care begins at the end of an operation and continues throughout the
hospitalization period as well in the outpatient period. It involves the following:
The patients are extubated before they leave the operation theatre and secretions from the
airway are cleared.
Opiods are administered orally or patenterally for relieving pain. This also prevents
constipation (Stephens & Whitman, 2015).
Mental status is assessed. Fluid and electrolyte imbalances are restored.
Wound sites are checked twice regularly after removing operative dressing. Drain tubes
are monitored for the collected fluid.
Decrease risks of deep venous thrombosis.
Urine output is monitored. Catheters are used for patients with distended bladder.
Patients are made to sit up on their beds and are made to perform mild exercise to prevent
onset of sarcopenia (Nelson et al., 2016).
NAME- | STUDENT ID-
5ASSESSMENT 1 (QUESTIONING)
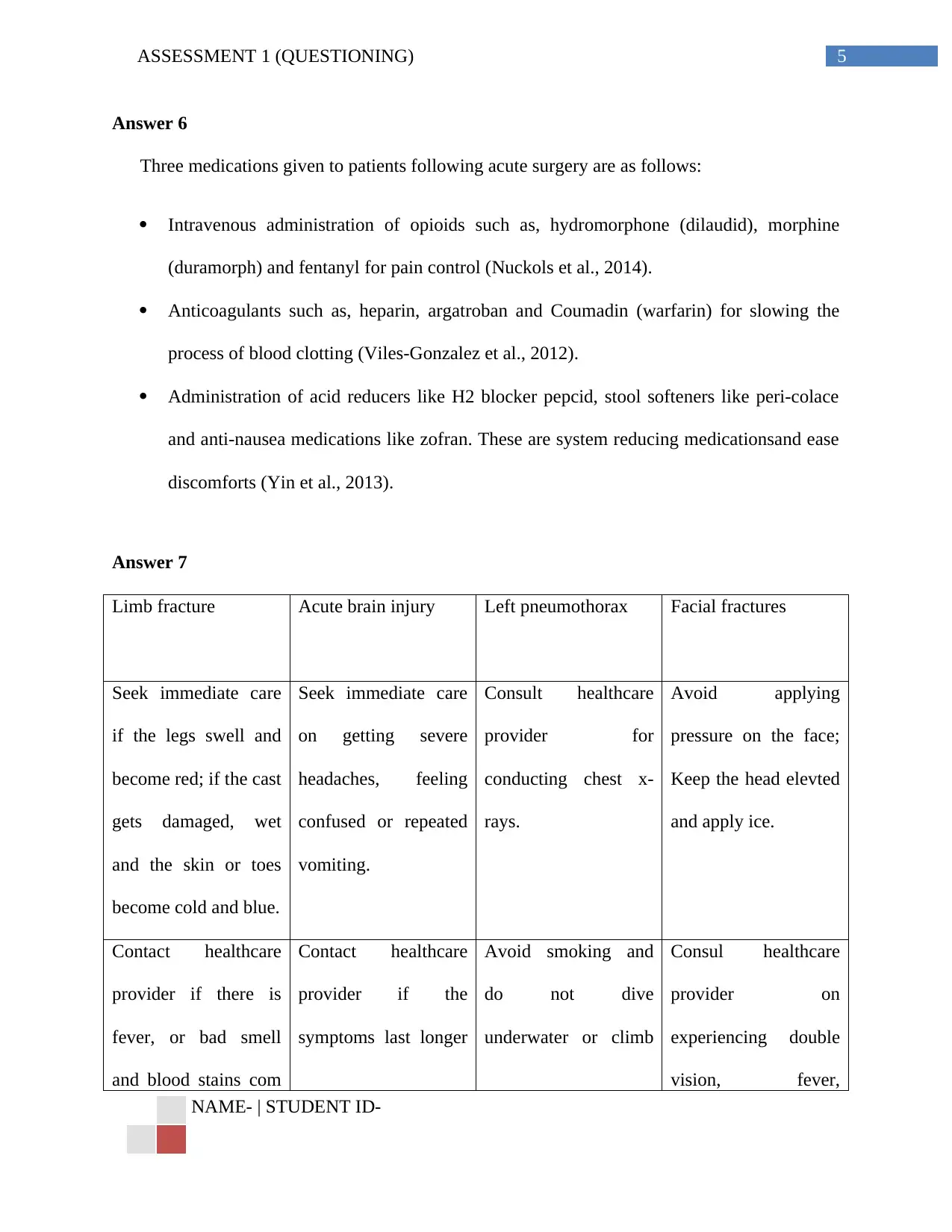
Answer 6
Three medications given to patients following acute surgery are as follows:
Intravenous administration of opioids such as, hydromorphone (dilaudid), morphine
(duramorph) and fentanyl for pain control (Nuckols et al., 2014).
Anticoagulants such as, heparin, argatroban and Coumadin (warfarin) for slowing the
process of blood clotting (Viles-Gonzalez et al., 2012).
Administration of acid reducers like H2 blocker pepcid, stool softeners like peri-colace
and anti-nausea medications like zofran. These are system reducing medicationsand ease
discomforts (Yin et al., 2013).
Answer 7
Limb fracture Acute brain injury Left pneumothorax Facial fractures
Seek immediate care
if the legs swell and
become red; if the cast
gets damaged, wet
and the skin or toes
become cold and blue.
Seek immediate care
on getting severe
headaches, feeling
confused or repeated
vomiting.
Consult healthcare
provider for
conducting chest x-
rays.
Avoid applying
pressure on the face;
Keep the head elevted
and apply ice.
Contact healthcare
provider if there is
fever, or bad smell
and blood stains com
Contact healthcare
provider if the
symptoms last longer
Avoid smoking and
do not dive
underwater or climb
Consul healthcare
provider on
experiencing double
vision, fever,
NAME- | STUDENT ID-
Answer 6
Three medications given to patients following acute surgery are as follows:
Intravenous administration of opioids such as, hydromorphone (dilaudid), morphine
(duramorph) and fentanyl for pain control (Nuckols et al., 2014).
Anticoagulants such as, heparin, argatroban and Coumadin (warfarin) for slowing the
process of blood clotting (Viles-Gonzalez et al., 2012).
Administration of acid reducers like H2 blocker pepcid, stool softeners like peri-colace
and anti-nausea medications like zofran. These are system reducing medicationsand ease
discomforts (Yin et al., 2013).
Answer 7
Limb fracture Acute brain injury Left pneumothorax Facial fractures
Seek immediate care
if the legs swell and
become red; if the cast
gets damaged, wet
and the skin or toes
become cold and blue.
Seek immediate care
on getting severe
headaches, feeling
confused or repeated
vomiting.
Consult healthcare
provider for
conducting chest x-
rays.
Avoid applying
pressure on the face;
Keep the head elevted
and apply ice.
Contact healthcare
provider if there is
fever, or bad smell
and blood stains com
Contact healthcare
provider if the
symptoms last longer
Avoid smoking and
do not dive
underwater or climb
Consul healthcare
provider on
experiencing double
vision, fever,
NAME- | STUDENT ID-
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6ASSESSMENT 1 (QUESTIONING)
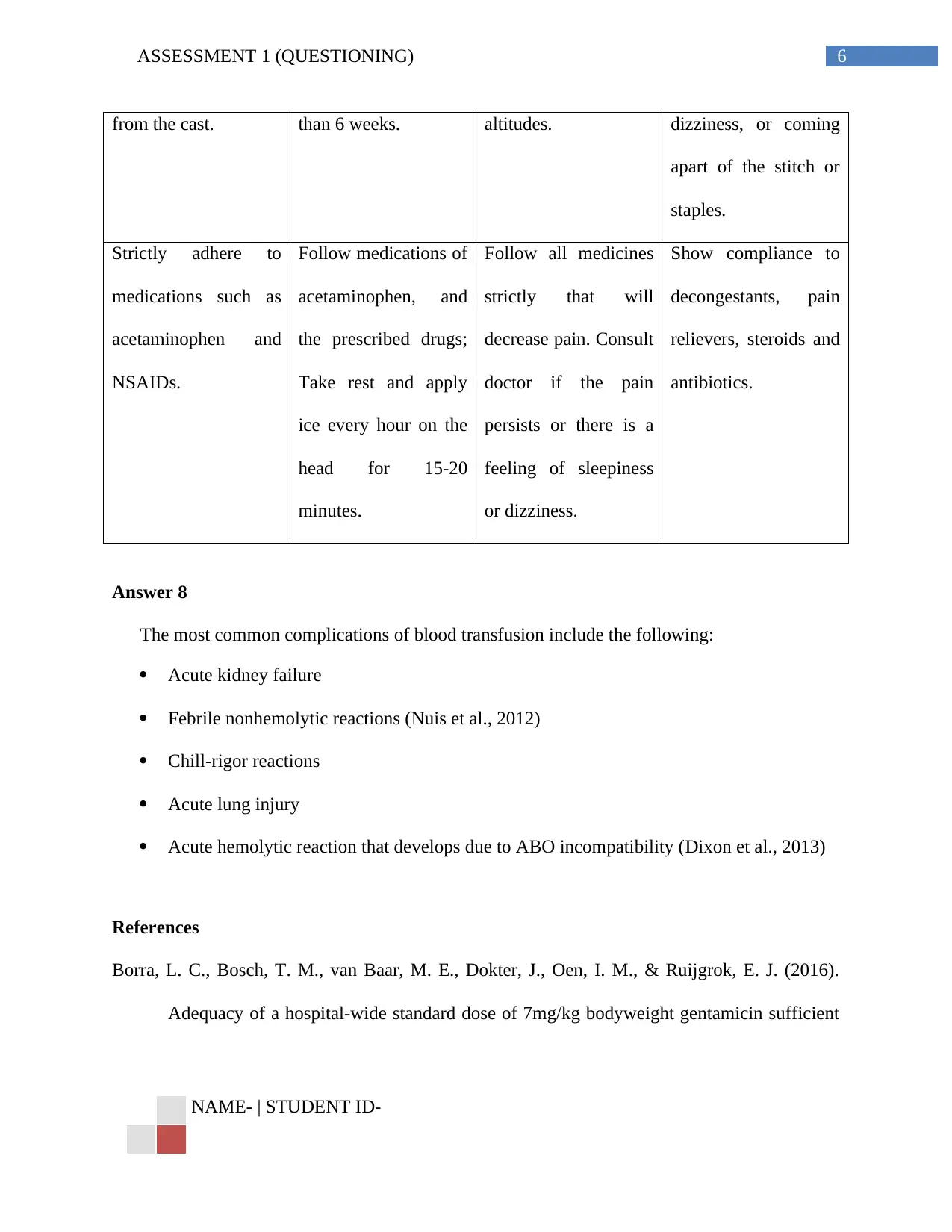
from the cast. than 6 weeks. altitudes. dizziness, or coming
apart of the stitch or
staples.
Strictly adhere to
medications such as
acetaminophen and
NSAIDs.
Follow medications of
acetaminophen, and
the prescribed drugs;
Take rest and apply
ice every hour on the
head for 15-20
minutes.
Follow all medicines
strictly that will
decrease pain. Consult
doctor if the pain
persists or there is a
feeling of sleepiness
or dizziness.
Show compliance to
decongestants, pain
relievers, steroids and
antibiotics.
Answer 8
The most common complications of blood transfusion include the following:
Acute kidney failure
Febrile nonhemolytic reactions (Nuis et al., 2012)
Chill-rigor reactions
Acute lung injury
Acute hemolytic reaction that develops due to ABO incompatibility (Dixon et al., 2013)
References
Borra, L. C., Bosch, T. M., van Baar, M. E., Dokter, J., Oen, I. M., & Ruijgrok, E. J. (2016).
Adequacy of a hospital-wide standard dose of 7mg/kg bodyweight gentamicin sufficient
NAME- | STUDENT ID-
from the cast. than 6 weeks. altitudes. dizziness, or coming
apart of the stitch or
staples.
Strictly adhere to
medications such as
acetaminophen and
NSAIDs.
Follow medications of
acetaminophen, and
the prescribed drugs;
Take rest and apply
ice every hour on the
head for 15-20
minutes.
Follow all medicines
strictly that will
decrease pain. Consult
doctor if the pain
persists or there is a
feeling of sleepiness
or dizziness.
Show compliance to
decongestants, pain
relievers, steroids and
antibiotics.
Answer 8
The most common complications of blood transfusion include the following:
Acute kidney failure
Febrile nonhemolytic reactions (Nuis et al., 2012)
Chill-rigor reactions
Acute lung injury
Acute hemolytic reaction that develops due to ABO incompatibility (Dixon et al., 2013)
References
Borra, L. C., Bosch, T. M., van Baar, M. E., Dokter, J., Oen, I. M., & Ruijgrok, E. J. (2016).
Adequacy of a hospital-wide standard dose of 7mg/kg bodyweight gentamicin sufficient
NAME- | STUDENT ID-
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7ASSESSMENT 1 (QUESTIONING)
to achieve an adequate prophylactic maximum serum concentration (C max) in burn
patients undergoing surgical burn wound treatment. Burns, 42(8), 1819-1824.
Bouglé, A., Harrois, A., & Duranteau, J. (2013). Resuscitative strategies in traumatic
hemorrhagic shock. Annals of intensive care, 3(1), 1.
Chitsike, R. S., Rodger, M. A., Kovacs, M. J., Betancourt, M. T., Wells, P. S., Anderson, D.
R., ... & Perrier, A. (2012). Risk of post‐thrombotic syndrome after subtherapeutic
warfarin anticoagulation for a first unprovoked deep vein thrombosis: results from the
REVERSE study. Journal of Thrombosis and Haemostasis, 10(10), 2039-2044.
Chow, W. B., Rosenthal, R. A., Merkow, R. P., Ko, C. Y., & Esnaola, N. F. (2012). Optimal
preoperative assessment of the geriatric surgical patient: a best practices guideline from
the American College of Surgeons National Surgical Quality Improvement Program and
the American Geriatrics Society. Journal of the American College of Surgeons, 215(4),
453-466.
Cole, C., Wellard, S., & Mummery, J. (2014). Problematising autonomy and advocacy in
nursing. Nursing ethics, 21(5), 576-582.
Cornock, M. (2014). Duty of care. Orthopaedic & Trauma Times, (24), 14-16.
Dixon, B., Santamaria, J. D., Reid, D., Collins, M., Rechnitzer, T., Newcomb, A. E., ... &
Campbell, D. J. (2013). The association of blood transfusion with mortality after cardiac
surgery: cause or confounding?(CME). Transfusion, 53(1), 19-27.
NAME- | STUDENT ID-
to achieve an adequate prophylactic maximum serum concentration (C max) in burn
patients undergoing surgical burn wound treatment. Burns, 42(8), 1819-1824.
Bouglé, A., Harrois, A., & Duranteau, J. (2013). Resuscitative strategies in traumatic
hemorrhagic shock. Annals of intensive care, 3(1), 1.
Chitsike, R. S., Rodger, M. A., Kovacs, M. J., Betancourt, M. T., Wells, P. S., Anderson, D.
R., ... & Perrier, A. (2012). Risk of post‐thrombotic syndrome after subtherapeutic
warfarin anticoagulation for a first unprovoked deep vein thrombosis: results from the
REVERSE study. Journal of Thrombosis and Haemostasis, 10(10), 2039-2044.
Chow, W. B., Rosenthal, R. A., Merkow, R. P., Ko, C. Y., & Esnaola, N. F. (2012). Optimal
preoperative assessment of the geriatric surgical patient: a best practices guideline from
the American College of Surgeons National Surgical Quality Improvement Program and
the American Geriatrics Society. Journal of the American College of Surgeons, 215(4),
453-466.
Cole, C., Wellard, S., & Mummery, J. (2014). Problematising autonomy and advocacy in
nursing. Nursing ethics, 21(5), 576-582.
Cornock, M. (2014). Duty of care. Orthopaedic & Trauma Times, (24), 14-16.
Dixon, B., Santamaria, J. D., Reid, D., Collins, M., Rechnitzer, T., Newcomb, A. E., ... &
Campbell, D. J. (2013). The association of blood transfusion with mortality after cardiac
surgery: cause or confounding?(CME). Transfusion, 53(1), 19-27.
NAME- | STUDENT ID-
8ASSESSMENT 1 (QUESTIONING)
Griffith, R. (2015). Understanding the Code: scope of the duty of confidentiality. British journal
of community nursing, 20(6), 304-306.
Nelson, G., Altman, A. D., Nick, A., Meyer, L. A., Ramirez, P. T., Achtari, C., ... & Acheson, N.
(2016). Guidelines for postoperative care in gynecologic/oncology surgery: Enhanced
Recovery After Surgery (ERAS®) Society recommendations—Part II. Gynecologic
oncology, 140(2), 323-332.
Nuckols, T. K., Anderson, L., Popescu, I., Diamant, A. L., Doyle, B., Di Capua, P., & Chou, R.
(2014). Opioid prescribing: a systematic review and critical appraisal of guidelines for
chronic pain. Annals of internal medicine, 160(1), 38-47.
Nuis, R. J., Rodés-Cabau, J., Sinning, J. M., van Garsse, L., Kefer, J., Bosmans, J., ... & Werner,
N. (2012). Blood transfusion and the risk of acute kidney injury after transcatheter aortic
valve implantation. Circulation: Cardiovascular Interventions, 5(5), 680-688.
Nursing and midwifery board of australia, N.M.B.A . (2008). Code of Ethics for Nurses in
Australia. Retrieved from http://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-
Statements/Professional-standards.aspx
Ogle, O. E., & Mahjoubi, G. (2012). Local anesthesia: agents, techniques, and
complications. Dental Clinics of North America, 56(1), 133-148.
Oresanya, L. B., Lyons, W. L., & Finlayson, E. (2014). Preoperative assessment of the older
patient: a narrative review. Jama, 311(20), 2110-2120.
NAME- | STUDENT ID-
Griffith, R. (2015). Understanding the Code: scope of the duty of confidentiality. British journal
of community nursing, 20(6), 304-306.
Nelson, G., Altman, A. D., Nick, A., Meyer, L. A., Ramirez, P. T., Achtari, C., ... & Acheson, N.
(2016). Guidelines for postoperative care in gynecologic/oncology surgery: Enhanced
Recovery After Surgery (ERAS®) Society recommendations—Part II. Gynecologic
oncology, 140(2), 323-332.
Nuckols, T. K., Anderson, L., Popescu, I., Diamant, A. L., Doyle, B., Di Capua, P., & Chou, R.
(2014). Opioid prescribing: a systematic review and critical appraisal of guidelines for
chronic pain. Annals of internal medicine, 160(1), 38-47.
Nuis, R. J., Rodés-Cabau, J., Sinning, J. M., van Garsse, L., Kefer, J., Bosmans, J., ... & Werner,
N. (2012). Blood transfusion and the risk of acute kidney injury after transcatheter aortic
valve implantation. Circulation: Cardiovascular Interventions, 5(5), 680-688.
Nursing and midwifery board of australia, N.M.B.A . (2008). Code of Ethics for Nurses in
Australia. Retrieved from http://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-
Statements/Professional-standards.aspx
Ogle, O. E., & Mahjoubi, G. (2012). Local anesthesia: agents, techniques, and
complications. Dental Clinics of North America, 56(1), 133-148.
Oresanya, L. B., Lyons, W. L., & Finlayson, E. (2014). Preoperative assessment of the older
patient: a narrative review. Jama, 311(20), 2110-2120.
NAME- | STUDENT ID-
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9ASSESSMENT 1 (QUESTIONING)
Rohrig, R., Rönn, T., Lendemans, S., Feldkamp, T., de Groot, H., & Petrat, F. (2012). Adverse
effects of resuscitation with lactated ringer compared with ringer solution after severe
hemorrhagic shock in rats. Shock, 38(2), 137-145.
Rowan, M. P., Cancio, L. C., Elster, E. A., Burmeister, D. M., Rose, L. F., Natesan, S., ... &
Chung, K. K. (2015). Burn wound healing and treatment: review and
advancements. Critical care, 19(1), 243.
Stephens, R. S., & Whitman, G. J. (2015). Postoperative critical care of the adult cardiac surgical
patient. Part I: routine postoperative care. Critical care medicine, 43(7), 1477-1497.
Viles-Gonzalez, J. F., Kar, S., Douglas, P., Dukkipati, S., Feldman, T., Horton, R., ... & Reddy,
V. Y. (2012). The clinical impact of incomplete left atrial appendage closure with the
Watchman Device in patients with atrial fibrillation: a PROTECT AF (Percutaneous
Closure of the Left Atrial Appendage Versus Warfarin Therapy for Prevention of Stroke
in Patients With Atrial Fibrillation) substudy. Journal of the American College of
Cardiology, 59(10), 923-929.
Yang, Y. T., & Silverman, R. D. (2014). Mobile health applications: the patchwork of legal and
liability issues suggests strategies to improve oversight. Health Affairs, 33(2), 222-227.
Yin, O. Q., Bédoucha, V., McCulloch, T., Zheng, C., Zhou, W., Hussaini, A., & Novick, S.
(2013). Effects of famotidine or an antacid preparation on the pharmacokinetics of
nilotinib in healthy volunteers. Cancer chemotherapy and pharmacology, 71(1), 219-226.
NAME- | STUDENT ID-
Rohrig, R., Rönn, T., Lendemans, S., Feldkamp, T., de Groot, H., & Petrat, F. (2012). Adverse
effects of resuscitation with lactated ringer compared with ringer solution after severe
hemorrhagic shock in rats. Shock, 38(2), 137-145.
Rowan, M. P., Cancio, L. C., Elster, E. A., Burmeister, D. M., Rose, L. F., Natesan, S., ... &
Chung, K. K. (2015). Burn wound healing and treatment: review and
advancements. Critical care, 19(1), 243.
Stephens, R. S., & Whitman, G. J. (2015). Postoperative critical care of the adult cardiac surgical
patient. Part I: routine postoperative care. Critical care medicine, 43(7), 1477-1497.
Viles-Gonzalez, J. F., Kar, S., Douglas, P., Dukkipati, S., Feldman, T., Horton, R., ... & Reddy,
V. Y. (2012). The clinical impact of incomplete left atrial appendage closure with the
Watchman Device in patients with atrial fibrillation: a PROTECT AF (Percutaneous
Closure of the Left Atrial Appendage Versus Warfarin Therapy for Prevention of Stroke
in Patients With Atrial Fibrillation) substudy. Journal of the American College of
Cardiology, 59(10), 923-929.
Yang, Y. T., & Silverman, R. D. (2014). Mobile health applications: the patchwork of legal and
liability issues suggests strategies to improve oversight. Health Affairs, 33(2), 222-227.
Yin, O. Q., Bédoucha, V., McCulloch, T., Zheng, C., Zhou, W., Hussaini, A., & Novick, S.
(2013). Effects of famotidine or an antacid preparation on the pharmacokinetics of
nilotinib in healthy volunteers. Cancer chemotherapy and pharmacology, 71(1), 219-226.
NAME- | STUDENT ID-
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.