Health Workforce Planning Report: India's Five-Year Plan
VerifiedAdded on 2023/01/20
|15
|3916
|74
Report
AI Summary
This report presents a comprehensive health workforce plan for India, focusing on a five-year strategy to address critical issues within the healthcare system. It begins with an executive summary highlighting the need for reform and increased government spending on infrastructure to bridge gaps in healthcare quality. The introduction outlines the strategic workforce planning tool and defines the health workforce, encompassing both public and private sectors. The report then analyzes the evolution of health workforce norms in India, referencing key committees and standards, and conducts an environmental scan to identify strengths, weaknesses, opportunities, and threats. It highlights current shortfalls in health manpower, including reasons for these deficits, and provides a data profile of health workers by category using WHO data. The report identifies critical issues, such as the concentration of health workers in urban areas and brain drain in rural areas, and discusses WHO recommendations for improvement. Finally, it proposes strategies to implement these recommendations, including investments in job creation, education, service model reforms, technology, humanitarian efforts, financial resources, and international collaboration. The report aims to provide a roadmap for strengthening India's health workforce and improving healthcare outcomes.
Running head: Health Work force Planning 1
HEALTH WORK FORCE PLANNING
HEALTH WORK FORCE PLANNING
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Health work force planning 2
TABLE OF CONTENTS-
CONTENTS PAGE NUMBER
1. Executive summary 3
2. Introduction of Health workforce
plan
4
3. Environmental scan 6
4. Critical issues to be addressed in the
workforce plan
8
5. 10 recommendations developed in
WHO 2016 report working for health
and growth
9
6. Strategies to implement in the health
workforce plan according to the
recommendations
9
7. Health workforce statistics of India 11
8. Conclusion 13
9. References 14
TABLE OF CONTENTS-
CONTENTS PAGE NUMBER
1. Executive summary 3
2. Introduction of Health workforce
plan
4
3. Environmental scan 6
4. Critical issues to be addressed in the
workforce plan
8
5. 10 recommendations developed in
WHO 2016 report working for health
and growth
9
6. Strategies to implement in the health
workforce plan according to the
recommendations
9
7. Health workforce statistics of India 11
8. Conclusion 13
9. References 14
Health work force planning 3
EXECUTIVE SUMMARY
Health systems and outcomes in India lagged behind in quality healthcare when compared to
the other nations . Mixed progress was made in the last decade and the situation is further
complicated by the in equality in India’s health workforce .There is a need to reform and
certain recommendations are introduced which should be implemented by developing robust
strategies urgently. The government needs to spend more on the proper infrastructure in to fill
the gaps between infrastructure and quality healthcare. Utilization of workforce and its
scarcity in different sectors of the country needs to be assessed and appropriate amendments
to be made soon .
The private sector and the government should collaborate in such a manner so that the quality
in the health care should gain momentum in the country. At the same time variations in
epidemiology and demographics will be beneficial for the private sector as it will be able to
gain more oppurtunities. The national density of doctors was 79.7 per lakh population, of
nurses and midwives 61.3 per lakh, and of dentists just 2.4 per lakh. Only 38.0% health
workers are female . Male to female ratio in case of doctors case of doctors is 5.1, and 0.2 in
case of nurses and midwives. These census data provide in depth and comprehensive picture
of health workers in each district including both rural and urban parts of the country .
Detailed data sources related to the health care personnel those who are employed in the
public sector are incomplete because of noncoverage of certain areas of health care as they do
not reflect retirement, death or migration in the professions covered.
Through National Rural Health Mission (NRHM), India has recruited additional 160 000
health workforce including doctors, nurses and midwives and around 900 000 community
health workers called Accredited Social Health Activists (ASHAs) to facilitate and mobilize
the interface between the communities and healthcare system. Currently, India produces
51800 doctors and 24000 specialists annually from 387 medical colleges in the country and it
has a potential of producing 279 000 nurses and midwives annually from 7401 institutions.
EXECUTIVE SUMMARY
Health systems and outcomes in India lagged behind in quality healthcare when compared to
the other nations . Mixed progress was made in the last decade and the situation is further
complicated by the in equality in India’s health workforce .There is a need to reform and
certain recommendations are introduced which should be implemented by developing robust
strategies urgently. The government needs to spend more on the proper infrastructure in to fill
the gaps between infrastructure and quality healthcare. Utilization of workforce and its
scarcity in different sectors of the country needs to be assessed and appropriate amendments
to be made soon .
The private sector and the government should collaborate in such a manner so that the quality
in the health care should gain momentum in the country. At the same time variations in
epidemiology and demographics will be beneficial for the private sector as it will be able to
gain more oppurtunities. The national density of doctors was 79.7 per lakh population, of
nurses and midwives 61.3 per lakh, and of dentists just 2.4 per lakh. Only 38.0% health
workers are female . Male to female ratio in case of doctors case of doctors is 5.1, and 0.2 in
case of nurses and midwives. These census data provide in depth and comprehensive picture
of health workers in each district including both rural and urban parts of the country .
Detailed data sources related to the health care personnel those who are employed in the
public sector are incomplete because of noncoverage of certain areas of health care as they do
not reflect retirement, death or migration in the professions covered.
Through National Rural Health Mission (NRHM), India has recruited additional 160 000
health workforce including doctors, nurses and midwives and around 900 000 community
health workers called Accredited Social Health Activists (ASHAs) to facilitate and mobilize
the interface between the communities and healthcare system. Currently, India produces
51800 doctors and 24000 specialists annually from 387 medical colleges in the country and it
has a potential of producing 279 000 nurses and midwives annually from 7401 institutions.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Health work force planning 4
INTRODUCTION OF HEALTH WORK FORCE PLAN-
The Strategic Workforce Planning Tool defines workforce planning as long-term strategic ,
oriented planning which is integrated with the organisation’s process and basically foccusses
on the size and the workforce quality. It mainly involves health workers by planning , trainig
and education and finally recruitment. Health workforce is the referred to group of all
individuals available with the healthcare systems who all are involved in its smooth
functioning like physicians , nurses, midwives and other community health workers (WHO
Health Statistics Report,2015) which includes individuals from both private and public
sectors and different sectors like preventive care, non-personal public health interventions,
disease prevention, management , health protection and promotion services and research.
Human resources actually which are engaged in the health system are known as the health
system workforce .
HEALTH WORKFORCE PLAN FOR INDIA
Rationale for selecting the country-
1. Living conditions and working environment is poor.
2. Workload of healthcare is high.
3. Country faces an acute shortage of trained health workforce
Health manpower means trained individuals who are involved in promoting health, to
prevent and cure disease or rehabilitation processes. . Estimates of the health workers differ
from one place to another . Data is to be furnished with the help of different methods like
labour and employment surveys, routine collection of data, and determination of population
INTRODUCTION OF HEALTH WORK FORCE PLAN-
The Strategic Workforce Planning Tool defines workforce planning as long-term strategic ,
oriented planning which is integrated with the organisation’s process and basically foccusses
on the size and the workforce quality. It mainly involves health workers by planning , trainig
and education and finally recruitment. Health workforce is the referred to group of all
individuals available with the healthcare systems who all are involved in its smooth
functioning like physicians , nurses, midwives and other community health workers (WHO
Health Statistics Report,2015) which includes individuals from both private and public
sectors and different sectors like preventive care, non-personal public health interventions,
disease prevention, management , health protection and promotion services and research.
Human resources actually which are engaged in the health system are known as the health
system workforce .
HEALTH WORKFORCE PLAN FOR INDIA
Rationale for selecting the country-
1. Living conditions and working environment is poor.
2. Workload of healthcare is high.
3. Country faces an acute shortage of trained health workforce
Health manpower means trained individuals who are involved in promoting health, to
prevent and cure disease or rehabilitation processes. . Estimates of the health workers differ
from one place to another . Data is to be furnished with the help of different methods like
labour and employment surveys, routine collection of data, and determination of population
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Health work force planning 5
censuses. WHO global health workforce statistics disaggregated health workforce and
metadata discriptors (WHO Global Health Workforce Statistics. 2015)
EVOLUTION OF HEALTH WORKFORCE NORMS IN INDIA AND THE
WORKFORCE PLAN (Hazarika, I. 2013) -
Bhore committee 1946 : Each PHC- 40,000 population should have 2 Medical officers, 4
PHNs, 1Nurse, midwives-4, trained dais-4, health assistants-2, and 4 other class four
employees.
Chadha Committee(1963); a laboratory technician per 30,000 population and a health
inspector which is per 20,000 population. A basic health worker per 10,000 population.
Kartar Singh Committee 1974): one male and female health worker each for 3,000 - 3,500
population at the grassroots, i.e. within a distance of less than 5 kilometers.
Indian Public Health Standards (IPHS) (2007, 2012): 1 Sub center: 3000-5000 with 2 health
worker( M& F)
1 PHC: 20000- 30000 with 3 medical officer, 1 AYUSH practitioner, and 20 other staff
1 CHC: 80000-100000 with 5 specialist doctors 1 public health manager, 1 dental surgeon, 6
GDMO 1 AYUSH Specialist and 1GDMO AYUSH and 64 other staff
A competent team of around field researchers were allocated collect data from the facilities
across seven randomly selected underprivileged zones. They were required to do the the data
entry both qualitative and quantitative , group transcription and group analysis (McMenamin,
A.,at al. 2017)
Newer initiatives from the Recommendations Of High Level Expert Group Report On
Universal Health Coverage (HLEG) For India-
Community Health Worker (CHW) at the village level are employed for the completion of
the healthcare task .The job regarding control of various diseases prevailing in the community
communicable and non- communicable both may be assigned to the CHW with specific job
responsibilities including (Devitt, R., et al., 2005) . The performance based monthly
compensation of Rs.1500 should be through ANMs in rural areas and their corresponding
censuses. WHO global health workforce statistics disaggregated health workforce and
metadata discriptors (WHO Global Health Workforce Statistics. 2015)
EVOLUTION OF HEALTH WORKFORCE NORMS IN INDIA AND THE
WORKFORCE PLAN (Hazarika, I. 2013) -
Bhore committee 1946 : Each PHC- 40,000 population should have 2 Medical officers, 4
PHNs, 1Nurse, midwives-4, trained dais-4, health assistants-2, and 4 other class four
employees.
Chadha Committee(1963); a laboratory technician per 30,000 population and a health
inspector which is per 20,000 population. A basic health worker per 10,000 population.
Kartar Singh Committee 1974): one male and female health worker each for 3,000 - 3,500
population at the grassroots, i.e. within a distance of less than 5 kilometers.
Indian Public Health Standards (IPHS) (2007, 2012): 1 Sub center: 3000-5000 with 2 health
worker( M& F)
1 PHC: 20000- 30000 with 3 medical officer, 1 AYUSH practitioner, and 20 other staff
1 CHC: 80000-100000 with 5 specialist doctors 1 public health manager, 1 dental surgeon, 6
GDMO 1 AYUSH Specialist and 1GDMO AYUSH and 64 other staff
A competent team of around field researchers were allocated collect data from the facilities
across seven randomly selected underprivileged zones. They were required to do the the data
entry both qualitative and quantitative , group transcription and group analysis (McMenamin,
A.,at al. 2017)
Newer initiatives from the Recommendations Of High Level Expert Group Report On
Universal Health Coverage (HLEG) For India-
Community Health Worker (CHW) at the village level are employed for the completion of
the healthcare task .The job regarding control of various diseases prevailing in the community
communicable and non- communicable both may be assigned to the CHW with specific job
responsibilities including (Devitt, R., et al., 2005) . The performance based monthly
compensation of Rs.1500 should be through ANMs in rural areas and their corresponding
Health work force planning 6
equivalent in urban areas. (Curson, J.,et al 2015) The estimated availability of roughly 19
lakh CHWs by 2022.
Increase HRH density to achieve WHO norms of at least 23 health workers (doctors, nurses,
and midwives) per 10,000 population .This will be facilitated by increasing financial aids to
strengthen the infra-structure for SC, PHC & CHCs and creating a new medical college at
each district. (Williams, J.,et al 2016)
To fulfill these recommendations Simultaneously progress towards making available at least
one ANM school in all districts with over 5 lakh population and Strengthen Lady Health
Visitor (LHV) training centres to ensure adequately trained CHW and ANM supervisor.
(Thakur, J. 2019).
ENVIRONMENTAL SCANNING -
The most reliable and common approach to strategic healthforce planning is an external
environmental scanning or analysis to identify the possibilities and threats facing the
organization, and internal scan to analyse the organization’s risk and upcoming opputunities.
(Koo, D., et al.,2016)
EXTERNAl SCANNING- Involves core environmental trends like little population growth in
a region since last 5 decades and this trend is likely to continue .Population in the region is
aging the younger population is leaving the region .Service sector employment especially in
health care .Government funding in health care needs
INTERNAL SCAN – SWOT analysis
Strength- Excellent health care facility and staff with strong qualifications Energetic and
innovative administration .Affordable and accessible quality programs
Weekness- Funding ,Communication,Teamwork
Oppurtunities-Population aging or decreasing ,State funding, More competition
Threats – like Population aging and decreasing, No state funding , Increasing competition
SHORTFALL IN CURRENT HEALTH MANPOWER
As on 31st March, 2015, there are 153655 Sub Centres, 25308 PHCs & 5396 Community
health centers functioning in the country. Total number of Sub Centres, PHCs and CHCs
equivalent in urban areas. (Curson, J.,et al 2015) The estimated availability of roughly 19
lakh CHWs by 2022.
Increase HRH density to achieve WHO norms of at least 23 health workers (doctors, nurses,
and midwives) per 10,000 population .This will be facilitated by increasing financial aids to
strengthen the infra-structure for SC, PHC & CHCs and creating a new medical college at
each district. (Williams, J.,et al 2016)
To fulfill these recommendations Simultaneously progress towards making available at least
one ANM school in all districts with over 5 lakh population and Strengthen Lady Health
Visitor (LHV) training centres to ensure adequately trained CHW and ANM supervisor.
(Thakur, J. 2019).
ENVIRONMENTAL SCANNING -
The most reliable and common approach to strategic healthforce planning is an external
environmental scanning or analysis to identify the possibilities and threats facing the
organization, and internal scan to analyse the organization’s risk and upcoming opputunities.
(Koo, D., et al.,2016)
EXTERNAl SCANNING- Involves core environmental trends like little population growth in
a region since last 5 decades and this trend is likely to continue .Population in the region is
aging the younger population is leaving the region .Service sector employment especially in
health care .Government funding in health care needs
INTERNAL SCAN – SWOT analysis
Strength- Excellent health care facility and staff with strong qualifications Energetic and
innovative administration .Affordable and accessible quality programs
Weekness- Funding ,Communication,Teamwork
Oppurtunities-Population aging or decreasing ,State funding, More competition
Threats – like Population aging and decreasing, No state funding , Increasing competition
SHORTFALL IN CURRENT HEALTH MANPOWER
As on 31st March, 2015, there are 153655 Sub Centres, 25308 PHCs & 5396 Community
health centers functioning in the country. Total number of Sub Centres, PHCs and CHCs
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Health work force planning 7
have increased in between 2014-15 but still not sufficient to meet the requirments of the
population. . ANMs in the subcenters and PHCs have also increasd from 133194 to 212185
from 2005 to 2015 which is a total of 59.3% increase in their percentage. Out of 25308
PHCs, 799 are having more than 4 doctors , 770 consisting of 3 doctors, and 2041 are
without doctors, 6436 PHCs are having lady doctor. Total 10237 PHCs are having AYUSH
facility, bihar having maximum ayush facility 1384 . Total number of doctors (allopathic) at
the primary cemters increased from 220308 to 27421 in the period from 2005 to 2015.
(Pittman, P.,et al., 2016).A reduction in the number of surgeons did occurred around 76.7 %
and even of 80.2% specialists at the community health centers (Tiwari, R., et al.,2018)
REASONS FOR SHORTFALL IN HEALTH WORKFORCE-
Reduction in the technical education and no updation of the health manpower , mismatch
human resource distribution, reduction in training facilities, lack of job satisfaction are major
causes.
Report of the environmental scans and its analysis by methods and outcomes.
Primary care workforce and hospitals, educational institutes were involves and their exsisting
public healthcare data sets were taken . Method administered was Interview, conversational
and assessment during workforce planning quantifiable measures were used according to the
needs of primary healthcare services in rural and underprivileged communities
More than 500 targeted individuals and organizations from India Group of workers developed
workgroup developed for the better understanding of the challenges , oppurtunities and
ongoing initiatives of the workforce . Electronic survey was done . Survey did reached to a
larger audience. Variety of challenges like financial challenges, healthcare system
implementation, etc were addressed.
have increased in between 2014-15 but still not sufficient to meet the requirments of the
population. . ANMs in the subcenters and PHCs have also increasd from 133194 to 212185
from 2005 to 2015 which is a total of 59.3% increase in their percentage. Out of 25308
PHCs, 799 are having more than 4 doctors , 770 consisting of 3 doctors, and 2041 are
without doctors, 6436 PHCs are having lady doctor. Total 10237 PHCs are having AYUSH
facility, bihar having maximum ayush facility 1384 . Total number of doctors (allopathic) at
the primary cemters increased from 220308 to 27421 in the period from 2005 to 2015.
(Pittman, P.,et al., 2016).A reduction in the number of surgeons did occurred around 76.7 %
and even of 80.2% specialists at the community health centers (Tiwari, R., et al.,2018)
REASONS FOR SHORTFALL IN HEALTH WORKFORCE-
Reduction in the technical education and no updation of the health manpower , mismatch
human resource distribution, reduction in training facilities, lack of job satisfaction are major
causes.
Report of the environmental scans and its analysis by methods and outcomes.
Primary care workforce and hospitals, educational institutes were involves and their exsisting
public healthcare data sets were taken . Method administered was Interview, conversational
and assessment during workforce planning quantifiable measures were used according to the
needs of primary healthcare services in rural and underprivileged communities
More than 500 targeted individuals and organizations from India Group of workers developed
workgroup developed for the better understanding of the challenges , oppurtunities and
ongoing initiatives of the workforce . Electronic survey was done . Survey did reached to a
larger audience. Variety of challenges like financial challenges, healthcare system
implementation, etc were addressed.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Health work force planning 8
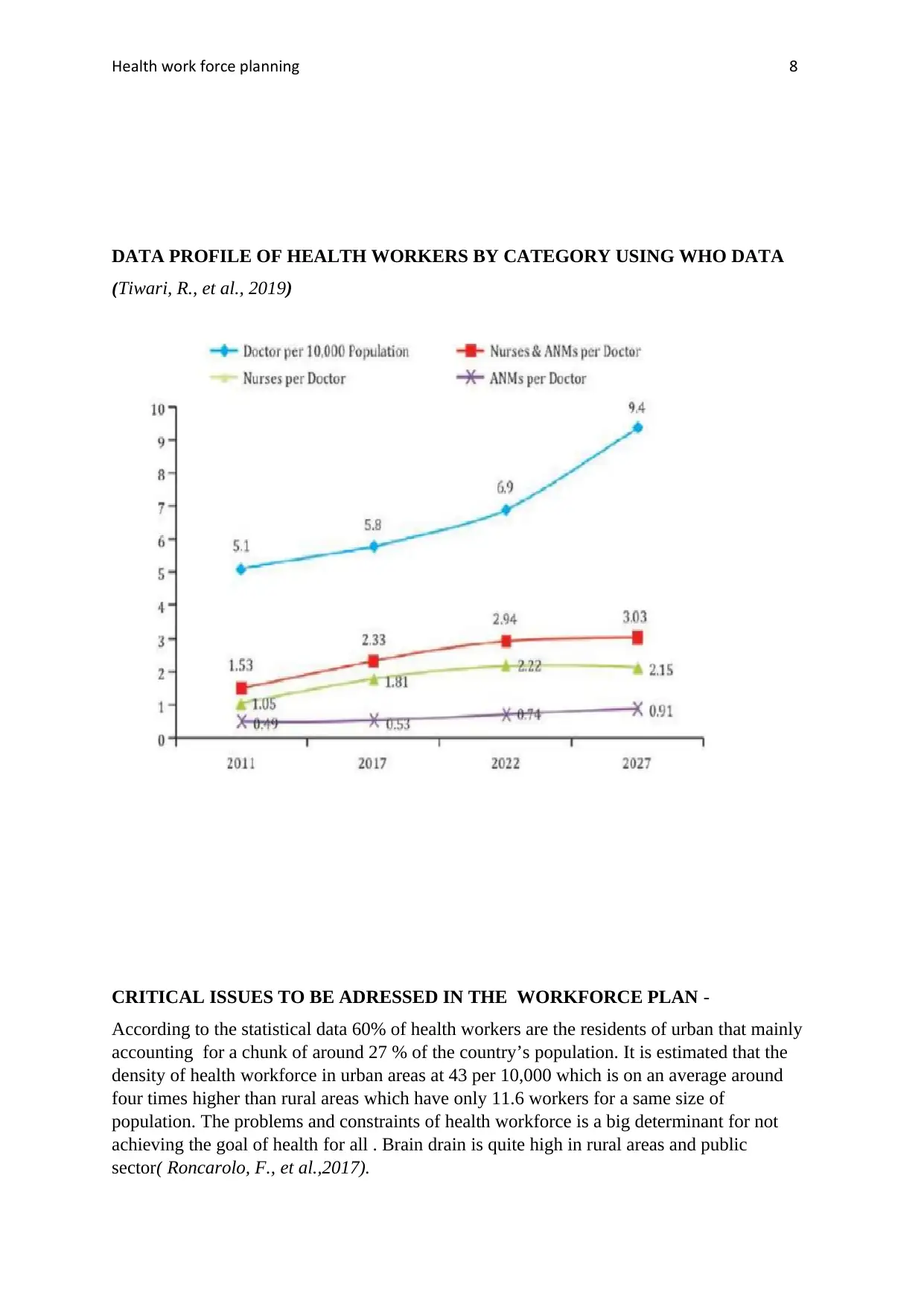
DATA PROFILE OF HEALTH WORKERS BY CATEGORY USING WHO DATA
(Tiwari, R., et al., 2019)
CRITICAL ISSUES TO BE ADRESSED IN THE WORKFORCE PLAN -
According to the statistical data 60% of health workers are the residents of urban that mainly
accounting for a chunk of around 27 % of the country’s population. It is estimated that the
density of health workforce in urban areas at 43 per 10,000 which is on an average around
four times higher than rural areas which have only 11.6 workers for a same size of
population. The problems and constraints of health workforce is a big determinant for not
achieving the goal of health for all . Brain drain is quite high in rural areas and public
sector( Roncarolo, F., et al.,2017).
DATA PROFILE OF HEALTH WORKERS BY CATEGORY USING WHO DATA
(Tiwari, R., et al., 2019)
CRITICAL ISSUES TO BE ADRESSED IN THE WORKFORCE PLAN -
According to the statistical data 60% of health workers are the residents of urban that mainly
accounting for a chunk of around 27 % of the country’s population. It is estimated that the
density of health workforce in urban areas at 43 per 10,000 which is on an average around
four times higher than rural areas which have only 11.6 workers for a same size of
population. The problems and constraints of health workforce is a big determinant for not
achieving the goal of health for all . Brain drain is quite high in rural areas and public
sector( Roncarolo, F., et al.,2017).
Health work force planning 9
10 RECOMMENDATIONS DEVELOPED IN WHO 2016 REPORT WORKING FOR
HEALTH AND GROWTH -
1. Creation of new job opportunities.
2. Ensure gender and women’s rights.
3. High quality education , training and skills.
4. Proper health service delivery and organisation.
5. Advanced technology .
6. Humanitarian setting and crises.
7. Financial and fiscal space.
8. Partnership and cooperation.
9. International migration.
10. Proper data information and accountability.
STRATEGIES TO IMPLEMENT IN THE HEALTH WORKFORCE PLAN
ACCORDING TO THE ABOVE RECOMMENDATIONS –
1. Investments in development of health sector jobs, mainly for women having the
desired skill with the right skills in the designated areas by developing labour market
policies to meet the demands for a sustainable health workforce.
2. Mainly by maximizing the economic participation of women by fostering their
empowerment through equality in education, government policies and norms.
3. High quality education so that all health workers are fully trained and can potentially
deal with the various health needs of the population. Strategy to implement exhaustive
education models for the health care workforce is required.
10 RECOMMENDATIONS DEVELOPED IN WHO 2016 REPORT WORKING FOR
HEALTH AND GROWTH -
1. Creation of new job opportunities.
2. Ensure gender and women’s rights.
3. High quality education , training and skills.
4. Proper health service delivery and organisation.
5. Advanced technology .
6. Humanitarian setting and crises.
7. Financial and fiscal space.
8. Partnership and cooperation.
9. International migration.
10. Proper data information and accountability.
STRATEGIES TO IMPLEMENT IN THE HEALTH WORKFORCE PLAN
ACCORDING TO THE ABOVE RECOMMENDATIONS –
1. Investments in development of health sector jobs, mainly for women having the
desired skill with the right skills in the designated areas by developing labour market
policies to meet the demands for a sustainable health workforce.
2. Mainly by maximizing the economic participation of women by fostering their
empowerment through equality in education, government policies and norms.
3. High quality education so that all health workers are fully trained and can potentially
deal with the various health needs of the population. Strategy to implement exhaustive
education models for the health care workforce is required.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Health work force planning 10
4. Reform service models concentrated on hospital care and focus instead on prevention
and on the efficient provision of high-quality, affordable, integrated, community-
based, people-centred primary and ambulatory care, paying special attention to
underserved areas or underprivileged areas . These can be done by organising such
clinical speciality centres and hospitals and public policies and regulatory bodies must
protect the interests of the public.
5. Rapidly changing technology is changing the fate of health services . Measures should
be taken to impart technologically enhanced health services which are person -centric
and cost effective also. Mainly digital technologies play an important role in
improving the health needs of the community.
6. Strategies must be implemented which should be regarding investment in the
International Health Regulations policies , and public health emergencies.
7. Strategies referring to raising funds both nationally and internationally .Investment
should be done in infrastructure , development of appropriate working environment
for the workforce ,Health financing can be secured by continuing growth in the public
revenue and good public policies which are capable of attracting foreign investors.
8. Strategy to promote collaboration at national and international levels; engage civil
society, unions and other health workers’ organizations and the private sector
9. Strategy to increase the benefits for health worker migration, and safeguard migrants’
rights. The smooth mobility of the health workforce provides various benefits to self
and destination nation.
10. Good data architecture depends on the active engagement of health workers,
employers and training institutions. OECD and WHO have a key role to play in
establishing of these regulatory bodies.
4. Reform service models concentrated on hospital care and focus instead on prevention
and on the efficient provision of high-quality, affordable, integrated, community-
based, people-centred primary and ambulatory care, paying special attention to
underserved areas or underprivileged areas . These can be done by organising such
clinical speciality centres and hospitals and public policies and regulatory bodies must
protect the interests of the public.
5. Rapidly changing technology is changing the fate of health services . Measures should
be taken to impart technologically enhanced health services which are person -centric
and cost effective also. Mainly digital technologies play an important role in
improving the health needs of the community.
6. Strategies must be implemented which should be regarding investment in the
International Health Regulations policies , and public health emergencies.
7. Strategies referring to raising funds both nationally and internationally .Investment
should be done in infrastructure , development of appropriate working environment
for the workforce ,Health financing can be secured by continuing growth in the public
revenue and good public policies which are capable of attracting foreign investors.
8. Strategy to promote collaboration at national and international levels; engage civil
society, unions and other health workers’ organizations and the private sector
9. Strategy to increase the benefits for health worker migration, and safeguard migrants’
rights. The smooth mobility of the health workforce provides various benefits to self
and destination nation.
10. Good data architecture depends on the active engagement of health workers,
employers and training institutions. OECD and WHO have a key role to play in
establishing of these regulatory bodies.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Health work force planning 11
There are large discrepancies in health workforce distribution and inequalities in health
worker provisions. This misdistribution adversely effects health outcomes in India. (Pozo-
Martin, F., et al. 2017)
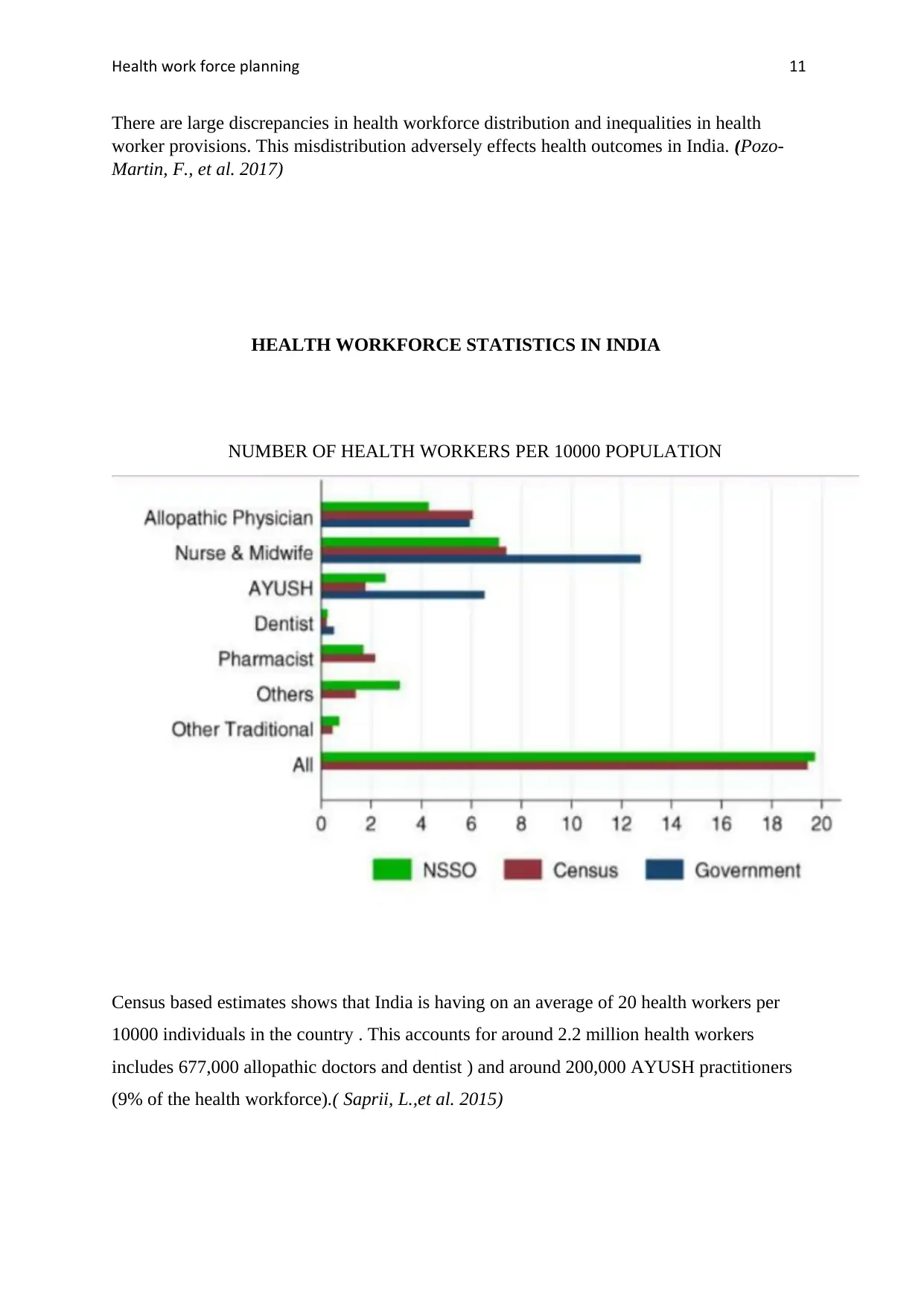
HEALTH WORKFORCE STATISTICS IN INDIA
NUMBER OF HEALTH WORKERS PER 10000 POPULATION
Census based estimates shows that India is having on an average of 20 health workers per
10000 individuals in the country . This accounts for around 2.2 million health workers
includes 677,000 allopathic doctors and dentist ) and around 200,000 AYUSH practitioners
(9% of the health workforce).( Saprii, L.,et al. 2015)
There are large discrepancies in health workforce distribution and inequalities in health
worker provisions. This misdistribution adversely effects health outcomes in India. (Pozo-
Martin, F., et al. 2017)
HEALTH WORKFORCE STATISTICS IN INDIA
NUMBER OF HEALTH WORKERS PER 10000 POPULATION
Census based estimates shows that India is having on an average of 20 health workers per
10000 individuals in the country . This accounts for around 2.2 million health workers
includes 677,000 allopathic doctors and dentist ) and around 200,000 AYUSH practitioners
(9% of the health workforce).( Saprii, L.,et al. 2015)
Health work force planning 12
CADRES OF HEALTHWORKERS IN INDIA-
Allopathic Doctors -Having an undergraduate degree i.e. MBBS which is bachelor of
medicine and bachelor of surgery alone or along with a speciality degree or diploma in a
speciality field.
Practioners of Ayurveda , Homeopathy , Unani , Sidha- Thes are called Ayush doctors holds
a degree or equivalent in one of the above desiciplines.
Nurses- Their qualification includes a three and a half year diploma in genral nursing and
midwifery (GNM) or a four year bacheolers degree (Bsc.) followed by two to three year post
graduate degree registered with nursing council of India.
Auxillary nurses and midwives- Have a two year diploma in the field of auxiliary nursing a
midwifery.
Community health workers-This group consists of individuals who have gone atleast 10 years
of formal education . They have underwent 23 days training to perform this function and
these includes health assistants and health educators.
Accredited Social health activist (ASHAs)-These health workers having a formal education
of atleast 8 years falling between the age group 25-45 years are the residents of the same
village in which they are serving and are they work under the NRHM (National Rural Health
Mission)
Each and every step is important in order to improve health outcomes for rural and
underprivileged population (Chokshi, M.,et al., 2016)
Primary health care, secondary and tertiary and specialist care hospitals each contribute to an
array of health care services (Lisam, S.,et al., 2015 )
Health workers have a variety of roles in health care systems. Right primary health care
approaches are important as there is a the high burden of chronic disease in underprivileged
nations (Parker, R.,et al. 2018)
There are no official, reliable measure to estimate the health workforce due to different
cadres, councils, systems of medicines and governing bodies. The sources of information are
mostly census, NSSO and professional bodies like MCI.
CADRES OF HEALTHWORKERS IN INDIA-
Allopathic Doctors -Having an undergraduate degree i.e. MBBS which is bachelor of
medicine and bachelor of surgery alone or along with a speciality degree or diploma in a
speciality field.
Practioners of Ayurveda , Homeopathy , Unani , Sidha- Thes are called Ayush doctors holds
a degree or equivalent in one of the above desiciplines.
Nurses- Their qualification includes a three and a half year diploma in genral nursing and
midwifery (GNM) or a four year bacheolers degree (Bsc.) followed by two to three year post
graduate degree registered with nursing council of India.
Auxillary nurses and midwives- Have a two year diploma in the field of auxiliary nursing a
midwifery.
Community health workers-This group consists of individuals who have gone atleast 10 years
of formal education . They have underwent 23 days training to perform this function and
these includes health assistants and health educators.
Accredited Social health activist (ASHAs)-These health workers having a formal education
of atleast 8 years falling between the age group 25-45 years are the residents of the same
village in which they are serving and are they work under the NRHM (National Rural Health
Mission)
Each and every step is important in order to improve health outcomes for rural and
underprivileged population (Chokshi, M.,et al., 2016)
Primary health care, secondary and tertiary and specialist care hospitals each contribute to an
array of health care services (Lisam, S.,et al., 2015 )
Health workers have a variety of roles in health care systems. Right primary health care
approaches are important as there is a the high burden of chronic disease in underprivileged
nations (Parker, R.,et al. 2018)
There are no official, reliable measure to estimate the health workforce due to different
cadres, councils, systems of medicines and governing bodies. The sources of information are
mostly census, NSSO and professional bodies like MCI.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.