Health Workforce Planning Report: India's Five-Year Strategic Plan
VerifiedAdded on 2023/01/19
|13
|3556
|54
Report
AI Summary
This report provides a detailed analysis of health workforce planning in India, focusing on challenges and proposing solutions. It begins with an executive summary and an environmental scan, evaluating the composition, density, and disparities within the workforce. The report delves into the data profile of the health workforce, highlighting issues such as the average population served by doctors, rural-urban disparities, and the presence of unqualified medical practitioners. The objectives for a five-year plan, based on WHO recommendations, are outlined, covering job creation, gender equality, education, technology, collaboration, and international migration. The report concludes with a discussion of the key findings and recommendations for improving India's health workforce, aiming to address critical shortages and enhance the quality of healthcare services. The report is based on the assignment brief provided, which required the development of a five-year national health workforce plan for a low and lower-middle income country, specifically focusing on the identification of critical issues and the formulation of strategies to address them.

Health Work Force Planning
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Executive Summary
Various versions of opinions exist when it comes to deciding what constitutes the health
workforce of a country, majorly depending on the situation the county is in at that point of
time and the way its entirety is monitored and looked after.
Human resources when it comes to health workforce includeevery employee or person who
holds single or multiple jobs at one or more than one location and receives payment in order
to provide voluntary services that maintain the health of the country.Proper workforce
planning can help churn out desired impacts when the aim is to build a healthy system. It will
work towards its duty which includes spreading information about human resources at the
same time helping build evidence in order to support a plan that presents forth a demand for
the required health workers due to their shortage. A proper workforce plan will help enlighten
a country like India, about what changes need to be made in order to have the desired impact
of the quality of services rendered.
Proper analysis of many factors (that seem to prove to be problems or other grieve issues
when it comes to a country) about the health workforce can enlighten and bring about results
which attempt to solve such problems with specific passive-aggressive measures. Every
source used to obtain such information will have its strength and weakness' but will still make
available comprehensive data for future decision making and policy implementation. This can
be done by first conducting an environment scan and later studying the data profiles of the
country. Coming up with contemporary solutions to directly attack the problems at hand
would be the next step, as stated in the following report.
Various versions of opinions exist when it comes to deciding what constitutes the health
workforce of a country, majorly depending on the situation the county is in at that point of
time and the way its entirety is monitored and looked after.
Human resources when it comes to health workforce includeevery employee or person who
holds single or multiple jobs at one or more than one location and receives payment in order
to provide voluntary services that maintain the health of the country.Proper workforce
planning can help churn out desired impacts when the aim is to build a healthy system. It will
work towards its duty which includes spreading information about human resources at the
same time helping build evidence in order to support a plan that presents forth a demand for
the required health workers due to their shortage. A proper workforce plan will help enlighten
a country like India, about what changes need to be made in order to have the desired impact
of the quality of services rendered.
Proper analysis of many factors (that seem to prove to be problems or other grieve issues
when it comes to a country) about the health workforce can enlighten and bring about results
which attempt to solve such problems with specific passive-aggressive measures. Every
source used to obtain such information will have its strength and weakness' but will still make
available comprehensive data for future decision making and policy implementation. This can
be done by first conducting an environment scan and later studying the data profiles of the
country. Coming up with contemporary solutions to directly attack the problems at hand
would be the next step, as stated in the following report.
Table of Contents
1.0 Introduction:.......................................................................................................................4
2.0 Environment Scan:.............................................................................................................5
2.1 Composition:..................................................................................................................5
2.2 Density:..........................................................................................................................5
2.3 Urban Rural disparities:.................................................................................................5
2.4 Male Female ratios:........................................................................................................5
2.5 Speed in the growth of doctors:.....................................................................................5
2.6 Education criteria’s:.......................................................................................................5
2.7 Important findings of the environment scan..................................................................6
3.0 Data Profile of the Health workforce in India....................................................................6
3.1 Average population served by an allopathic doctor in each govt..................................6
3.2Rural India is facing most of the brunt.................................................................................8
3.3 Fake Claims....................................................................................................................8
4.0 Objectives for the Five Year plan according to the ten recommendations of the WHO.. .8
4.1 Creation of jobs:.............................................................................................................8
4.2 Equal Gender and Women Rights:.................................................................................9
4.3 Education, skills and training:........................................................................................9
4.4 Technology:...................................................................................................................9
4.5 Collaborations and Co-operations:...............................................................................10
4.6 Crises and humanitarian settings:................................................................................10
4.7 International Migration:...............................................................................................10
5.0 Conclusion:......................................................................................................................10
6.0 Reference:........................................................................................................................12
1.0 Introduction:.......................................................................................................................4
2.0 Environment Scan:.............................................................................................................5
2.1 Composition:..................................................................................................................5
2.2 Density:..........................................................................................................................5
2.3 Urban Rural disparities:.................................................................................................5
2.4 Male Female ratios:........................................................................................................5
2.5 Speed in the growth of doctors:.....................................................................................5
2.6 Education criteria’s:.......................................................................................................5
2.7 Important findings of the environment scan..................................................................6
3.0 Data Profile of the Health workforce in India....................................................................6
3.1 Average population served by an allopathic doctor in each govt..................................6
3.2Rural India is facing most of the brunt.................................................................................8
3.3 Fake Claims....................................................................................................................8
4.0 Objectives for the Five Year plan according to the ten recommendations of the WHO.. .8
4.1 Creation of jobs:.............................................................................................................8
4.2 Equal Gender and Women Rights:.................................................................................9
4.3 Education, skills and training:........................................................................................9
4.4 Technology:...................................................................................................................9
4.5 Collaborations and Co-operations:...............................................................................10
4.6 Crises and humanitarian settings:................................................................................10
4.7 International Migration:...............................................................................................10
5.0 Conclusion:......................................................................................................................10
6.0 Reference:........................................................................................................................12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Introduction:
The potential and the capability of a country in order to meet its own health goals and
objectives mainly and specifically depend on the deployment of people who are responsible
for carrying out and delivering health services, along with motivation, skills and good
knowledge about the same. (Lopes, et al. 2015)
Most of the countries like India, however, lack the necessary human resources to provide
essential health services which are required in order to maintain healthy conditions in a
county. The reasons behind this are poor skills, imbalances in the demographics of the
countries, the constant migration and movement of various health workers in and around the
countries. Such problems need to be attended in order to come with a proper plan to face
these challenges.
The accurate description of Health workforce refers to all the people exclusively involved in
actions, and have their primary intent as the enhancement of health. These human resources
are made up of clinical staff, usually consisting of pharmacists, physicians, nurses as well as
dentists. Along with the main staff, even the management and support staff play a huge role,
they usually include the people that are necessary for the smooth functioning of the health
systems. These include ambulance drivers, accountants, managers amongst many. (World
Health Organization. 2016.)
The rationale behind selecting India as the country to be studied upon was the fact that India
is one of those countries who did not attempt to monitor the resourceseven up till the year
2011 effectively. As comprehensive data of these human resources were not easily available
at any one place, it is understood that when monitoring and studying the resources were
eventually started; it became a must to ensure the reliability of information from various
sources inorder to provide proper analysis. This increased the validity of the health workforce
statistics provided as they were and have been studied under a microscope to put forth only
reliable information. India, like most of the other countries, carries out its Health workforce
survey along with its population survey since 2011.De Bruecker et al. (2015)
On the other hand, when it comes to Health workforce planning, it is essential to have a
reliable system. In case if there exists any kind of a significant lag in it, it can affect the data
and the utility of the information in the process of any kind of decision making. (Pozo-
Martin, et al. 2017)
The potential and the capability of a country in order to meet its own health goals and
objectives mainly and specifically depend on the deployment of people who are responsible
for carrying out and delivering health services, along with motivation, skills and good
knowledge about the same. (Lopes, et al. 2015)
Most of the countries like India, however, lack the necessary human resources to provide
essential health services which are required in order to maintain healthy conditions in a
county. The reasons behind this are poor skills, imbalances in the demographics of the
countries, the constant migration and movement of various health workers in and around the
countries. Such problems need to be attended in order to come with a proper plan to face
these challenges.
The accurate description of Health workforce refers to all the people exclusively involved in
actions, and have their primary intent as the enhancement of health. These human resources
are made up of clinical staff, usually consisting of pharmacists, physicians, nurses as well as
dentists. Along with the main staff, even the management and support staff play a huge role,
they usually include the people that are necessary for the smooth functioning of the health
systems. These include ambulance drivers, accountants, managers amongst many. (World
Health Organization. 2016.)
The rationale behind selecting India as the country to be studied upon was the fact that India
is one of those countries who did not attempt to monitor the resourceseven up till the year
2011 effectively. As comprehensive data of these human resources were not easily available
at any one place, it is understood that when monitoring and studying the resources were
eventually started; it became a must to ensure the reliability of information from various
sources inorder to provide proper analysis. This increased the validity of the health workforce
statistics provided as they were and have been studied under a microscope to put forth only
reliable information. India, like most of the other countries, carries out its Health workforce
survey along with its population survey since 2011.De Bruecker et al. (2015)
On the other hand, when it comes to Health workforce planning, it is essential to have a
reliable system. In case if there exists any kind of a significant lag in it, it can affect the data
and the utility of the information in the process of any kind of decision making. (Pozo-
Martin, et al. 2017)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Environment Scan:
Environment scan is a way to make systems which helps organisations and countries to easily
identify the threats early as well as opportunities that may be of due importance in workforce
planning. It is basically a process by which one can determine various factors and the range
of which can lead to influence an organization's workforce in the future. (Addicottet al. 2015)
Environmental Scan and National profile of India
Composition: It is believed that of the out of a population of 133.92 crores in India, roughly
around 39% were doctors, approximately 30% were midwives and nurses, 1.2% marginally
covered the dentist. Out of all the doctors, around 70% were allopathic, whereas
approximately 22% were ayurvedic, Unani and homeopathic. (Rao, et al. 2016)
Density: The nation’s density when it comes to doctors was around 79l per lakh of the
population, and that of nurses and dentists were 61 and 2.4, respectively.
Urban-Rural disparities:Almost out of all the rural workers, around 30% were found to be
in rural areas and 70% in the urban.
Male Female ratios: Around 38% of the health workers were female, and the ratio of all
health workers is 1.6, out of which of doctors is 5.1, midwives and nurses in 0.2. (Fan, et al.
2016)
Speed in the growth of doctors:In India, there are approximately 462 medical colleges that
are responsible for almost around 56000+ doctors every year. On the same lines, about 3,123
institutions are preparing nurses around the country every year. Even though the numbers
seem high, they still fall low when the country's over increasing population of almost 26
Million every year is taken into account. The number of medical staff in comparison to such a
large number will thus logically present a shortage.
Education criteria’s:One of the other main problems that India faces is the shortfall of
trained professionals, due to the long 5year period taken to attain an MBBS degree, which
also slows down the entire process. The situation is different in China because most of the
doctors there hold only 3-year medical diplomas, and most of the needs are met through the
means of paramedics. (Joumard, et al. 2015)
Important findings of the environment scan
On average, a government doctor almost attends to around 11,082 people in India, which,
according to WHO is about 10 times more than the actual number. The easily noticeable
shortage in the existence of government doctors is not a grieve issue in India, where about
Environment scan is a way to make systems which helps organisations and countries to easily
identify the threats early as well as opportunities that may be of due importance in workforce
planning. It is basically a process by which one can determine various factors and the range
of which can lead to influence an organization's workforce in the future. (Addicottet al. 2015)
Environmental Scan and National profile of India
Composition: It is believed that of the out of a population of 133.92 crores in India, roughly
around 39% were doctors, approximately 30% were midwives and nurses, 1.2% marginally
covered the dentist. Out of all the doctors, around 70% were allopathic, whereas
approximately 22% were ayurvedic, Unani and homeopathic. (Rao, et al. 2016)
Density: The nation’s density when it comes to doctors was around 79l per lakh of the
population, and that of nurses and dentists were 61 and 2.4, respectively.
Urban-Rural disparities:Almost out of all the rural workers, around 30% were found to be
in rural areas and 70% in the urban.
Male Female ratios: Around 38% of the health workers were female, and the ratio of all
health workers is 1.6, out of which of doctors is 5.1, midwives and nurses in 0.2. (Fan, et al.
2016)
Speed in the growth of doctors:In India, there are approximately 462 medical colleges that
are responsible for almost around 56000+ doctors every year. On the same lines, about 3,123
institutions are preparing nurses around the country every year. Even though the numbers
seem high, they still fall low when the country's over increasing population of almost 26
Million every year is taken into account. The number of medical staff in comparison to such a
large number will thus logically present a shortage.
Education criteria’s:One of the other main problems that India faces is the shortfall of
trained professionals, due to the long 5year period taken to attain an MBBS degree, which
also slows down the entire process. The situation is different in China because most of the
doctors there hold only 3-year medical diplomas, and most of the needs are met through the
means of paramedics. (Joumard, et al. 2015)
Important findings of the environment scan
On average, a government doctor almost attends to around 11,082 people in India, which,
according to WHO is about 10 times more than the actual number. The easily noticeable
shortage in the existence of government doctors is not a grieve issue in India, where about
almost 70% of the expenses related to health care are met by expenditures that are considered
to be out of pocket. (Squires, et al. 2017)India is majorly battling a crisis, and that is the
evident shortage of government doctors and the inadequate infrastructure. The last nine years,
almost 72 thousand infants in Madhya Pradesh could not be saved due to the shortage of
medical staff, especially doctors.
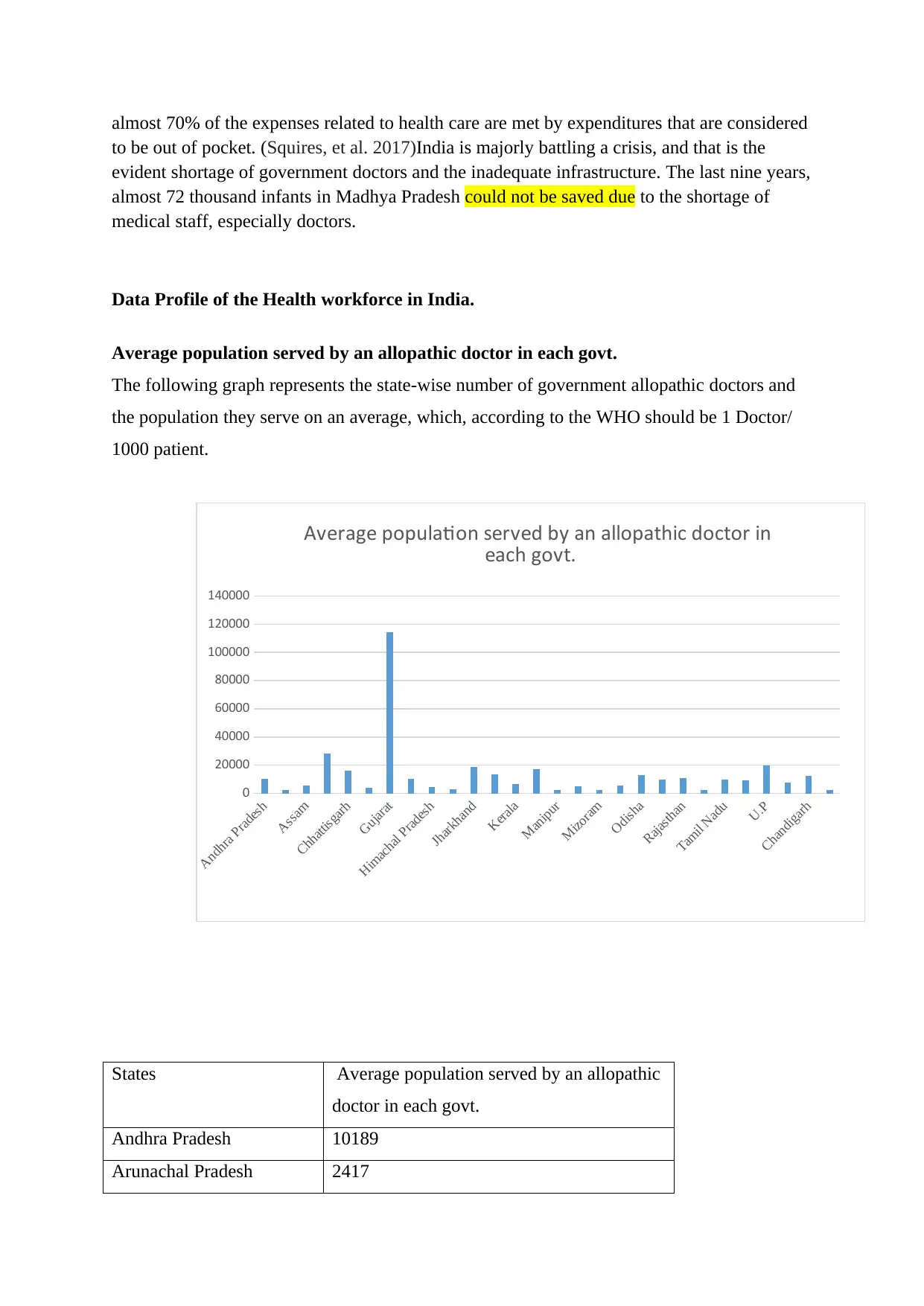
Data Profile of the Health workforce in India.
Average population served by an allopathic doctor in each govt.
The following graph represents the state-wise number of government allopathic doctors and
the population they serve on an average, which, according to the WHO should be 1 Doctor/
1000 patient.
Andhra Pradesh
Assam
Chhattisgarh
Gujarat
Himachal Pradesh
Jharkhand
Kerala
Manipur
Mizoram
Odisha
Rajasthan
Tamil Nadu
U.P
Chandigarh
0
20000
40000
60000
80000
100000
120000
140000
Average population served by an allopathic doctor in
each govt.
States Average population served by an allopathic
doctor in each govt.
Andhra Pradesh 10189
Arunachal Pradesh 2417
to be out of pocket. (Squires, et al. 2017)India is majorly battling a crisis, and that is the
evident shortage of government doctors and the inadequate infrastructure. The last nine years,
almost 72 thousand infants in Madhya Pradesh could not be saved due to the shortage of
medical staff, especially doctors.
Data Profile of the Health workforce in India.
Average population served by an allopathic doctor in each govt.
The following graph represents the state-wise number of government allopathic doctors and
the population they serve on an average, which, according to the WHO should be 1 Doctor/
1000 patient.
Andhra Pradesh
Assam
Chhattisgarh
Gujarat
Himachal Pradesh
Jharkhand
Kerala
Manipur
Mizoram
Odisha
Rajasthan
Tamil Nadu
U.P
Chandigarh
0
20000
40000
60000
80000
100000
120000
140000
Average population served by an allopathic doctor in
each govt.
States Average population served by an allopathic
doctor in each govt.
Andhra Pradesh 10189
Arunachal Pradesh 2417
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
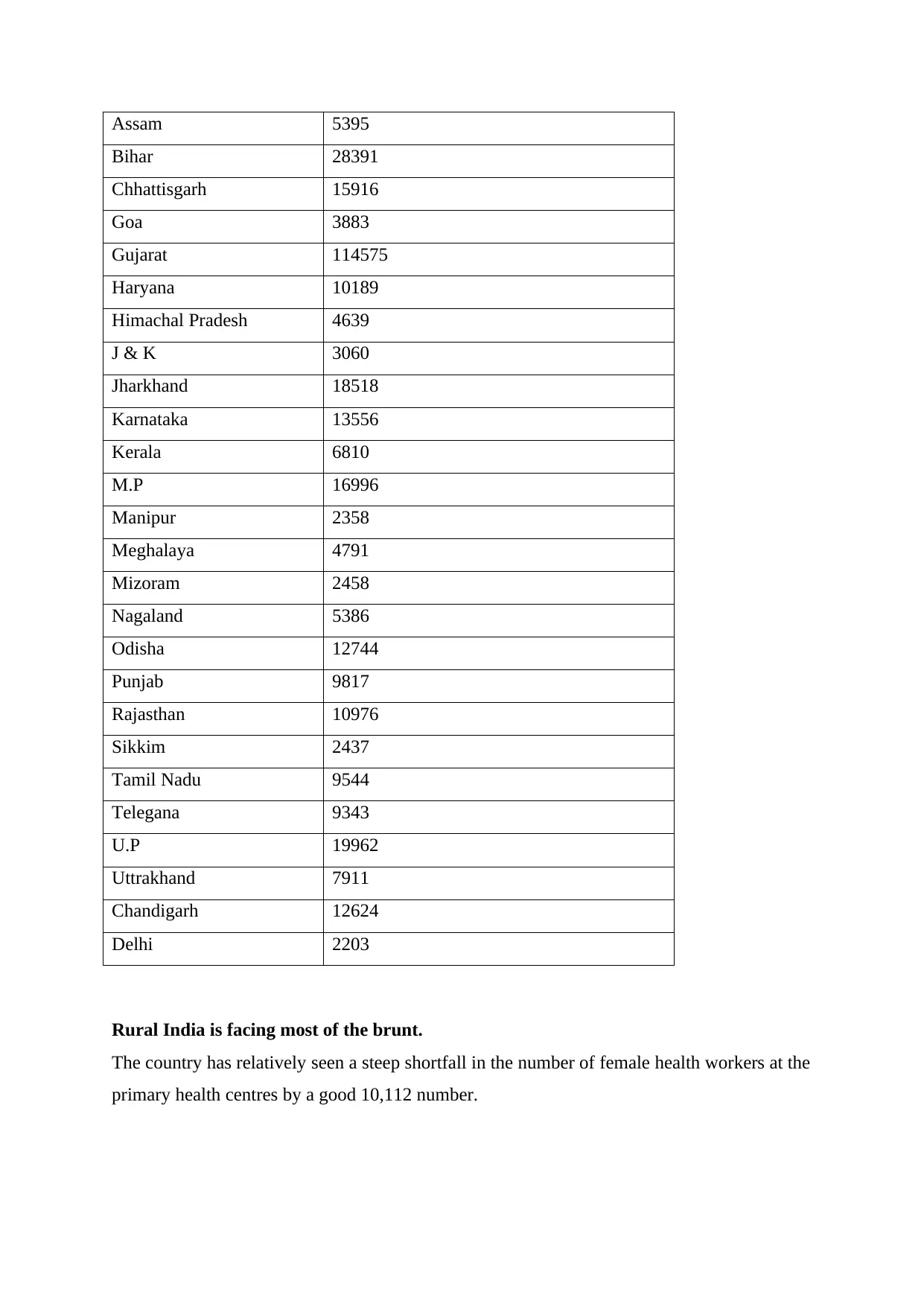
Assam 5395
Bihar 28391
Chhattisgarh 15916
Goa 3883
Gujarat 114575
Haryana 10189
Himachal Pradesh 4639
J & K 3060
Jharkhand 18518
Karnataka 13556
Kerala 6810
M.P 16996
Manipur 2358
Meghalaya 4791
Mizoram 2458
Nagaland 5386
Odisha 12744
Punjab 9817
Rajasthan 10976
Sikkim 2437
Tamil Nadu 9544
Telegana 9343
U.P 19962
Uttrakhand 7911
Chandigarh 12624
Delhi 2203
Rural India is facing most of the brunt.
The country has relatively seen a steep shortfall in the number of female health workers at the
primary health centres by a good 10,112 number.
Bihar 28391
Chhattisgarh 15916
Goa 3883
Gujarat 114575
Haryana 10189
Himachal Pradesh 4639
J & K 3060
Jharkhand 18518
Karnataka 13556
Kerala 6810
M.P 16996
Manipur 2358
Meghalaya 4791
Mizoram 2458
Nagaland 5386
Odisha 12744
Punjab 9817
Rajasthan 10976
Sikkim 2437
Tamil Nadu 9544
Telegana 9343
U.P 19962
Uttrakhand 7911
Chandigarh 12624
Delhi 2203
Rural India is facing most of the brunt.
The country has relatively seen a steep shortfall in the number of female health workers at the
primary health centres by a good 10,112 number.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
In rural areas, especially at the sub-centres, there is a shortfall of almost 11,713 female health
assistants and 15,592 male ones along with almost 6,100 female health workers and nurses
and midwives. (Buchan, et al. 2015)
It may not even come off as a shock that most of the primary health centres across India are
in urgent need and want of around 3000 doctors. There are also circumstances where almost
2000 centres are operating without being under the proper guidance of a doctor. (Hou, et al.
2015).
The state of the community centres is even worse as there is an evident shortfall as well as a
need for around 5000 surgeons.
Fake Claims
One of the other main and grieve problems that India is facing is the fact that there exist
many individuals who claim to be doctors and state it on their occupations but have been
found not to hold any requisite professional qualifications to stand by it. Almost one-third of
the people that call themselves are doctors have not been educated beyond the secondary
school. The absence of medical qualification while still conducting medical practice is a
crime, but is on the rise in India, especially in the rural areas. Considering the overall
population of registered doctors, only 19% of them have proper medical degrees and are
capable enough to tend the areas with the lowest amenities in India, which ironically
constitutes most of the population of the country.
Objectives for the Five Year plan according to the 10 recommendations of the WHO.
Creation of jobs:
Investing an amount in order to increase the number of decent jobs at the same time creation
of new jobs in the sectors related to health particularly in the rural areas of India, and even for
women and youth who have the right skills is a must. This commission will implement the
proper distribution of the right number of forces to the required places at the right time. This
will, in turn, foster and increase demand of the urban youth migrating to the rural areas in
search of better career opportunities.
Equal Gender and Women Rights:
assistants and 15,592 male ones along with almost 6,100 female health workers and nurses
and midwives. (Buchan, et al. 2015)
It may not even come off as a shock that most of the primary health centres across India are
in urgent need and want of around 3000 doctors. There are also circumstances where almost
2000 centres are operating without being under the proper guidance of a doctor. (Hou, et al.
2015).
The state of the community centres is even worse as there is an evident shortfall as well as a
need for around 5000 surgeons.
Fake Claims
One of the other main and grieve problems that India is facing is the fact that there exist
many individuals who claim to be doctors and state it on their occupations but have been
found not to hold any requisite professional qualifications to stand by it. Almost one-third of
the people that call themselves are doctors have not been educated beyond the secondary
school. The absence of medical qualification while still conducting medical practice is a
crime, but is on the rise in India, especially in the rural areas. Considering the overall
population of registered doctors, only 19% of them have proper medical degrees and are
capable enough to tend the areas with the lowest amenities in India, which ironically
constitutes most of the population of the country.
Objectives for the Five Year plan according to the 10 recommendations of the WHO.
Creation of jobs:
Investing an amount in order to increase the number of decent jobs at the same time creation
of new jobs in the sectors related to health particularly in the rural areas of India, and even for
women and youth who have the right skills is a must. This commission will implement the
proper distribution of the right number of forces to the required places at the right time. This
will, in turn, foster and increase demand of the urban youth migrating to the rural areas in
search of better career opportunities.
Equal Gender and Women Rights:
In today’s world there is a high increase in the number of female employees in comparison
to the numbers before, maximizing their economic participation and addressing as well as
taking care of gender biases at the same time tackling gender concern process will help in
growing the number of women that participate.
Education, skills and training:
When it comes to processes related to health, we trust only educated, skilled and trained
doctors. Many of the people in India do not have this option of choice due to the low level of
educated and highly trained skilled individuals. Making sure that any kind of education that is
provided is only of high quality will only help in churning out high-quality professionals.
Constantly keeping a check on the staff as well as the quality of their teachings when it
comes to college and degree staffs is the most important thing. Learning the right technique is
more important than learning just about any technique. It can be done by prioritizing
investments in the education models. The human race of the entire country depends on the
calibre of the health workforce that is responsible for their care.
Technology:
One of the most critical needs in today's world may it be any field, is technology, investing in
the right technological devices will not only help advance the field but also reduce the
complicated overworking of some of the health workforce at the same time providing better
care to the patients. Along with making investments in the above, it is also essential to
Provide suitable technologically advanced devices in rural areas. Making them readily
available to the doctors there will help reduce the reluctance of the urban doctors from going
to the rural place and at the same time reduce the turmoil's faced by the people. Most of the
rural areas do not even have gadgets that are a need in today's world. Making sure that
necessary basic instruments are made available first before progressing to buy new
technologies is essential.
Collaborations and Co-operations:
It is not easy to achieve a health workforce that is for the purpose; it needs actions across all
known sectors that are directly involved in the health labour market. The intersectoral
processes need the engagement of the public as well as the private sectors, along with them
even the trade unions and health work associations with other NGO’s and regulatory bodies.
Thus, having proper plans to carry out such collaborations and helping align them with
to the numbers before, maximizing their economic participation and addressing as well as
taking care of gender biases at the same time tackling gender concern process will help in
growing the number of women that participate.
Education, skills and training:
When it comes to processes related to health, we trust only educated, skilled and trained
doctors. Many of the people in India do not have this option of choice due to the low level of
educated and highly trained skilled individuals. Making sure that any kind of education that is
provided is only of high quality will only help in churning out high-quality professionals.
Constantly keeping a check on the staff as well as the quality of their teachings when it
comes to college and degree staffs is the most important thing. Learning the right technique is
more important than learning just about any technique. It can be done by prioritizing
investments in the education models. The human race of the entire country depends on the
calibre of the health workforce that is responsible for their care.
Technology:
One of the most critical needs in today's world may it be any field, is technology, investing in
the right technological devices will not only help advance the field but also reduce the
complicated overworking of some of the health workforce at the same time providing better
care to the patients. Along with making investments in the above, it is also essential to
Provide suitable technologically advanced devices in rural areas. Making them readily
available to the doctors there will help reduce the reluctance of the urban doctors from going
to the rural place and at the same time reduce the turmoil's faced by the people. Most of the
rural areas do not even have gadgets that are a need in today's world. Making sure that
necessary basic instruments are made available first before progressing to buy new
technologies is essential.
Collaborations and Co-operations:
It is not easy to achieve a health workforce that is for the purpose; it needs actions across all
known sectors that are directly involved in the health labour market. The intersectoral
processes need the engagement of the public as well as the private sectors, along with them
even the trade unions and health work associations with other NGO’s and regulatory bodies.
Thus, having proper plans to carry out such collaborations and helping align them with
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
international cooperation to promote investments in the health workforce are essential.
(Mason, et al. 2015).
Crises and humanitarian settings:
India should try to build and increase the capacity of its health force and systems to find out
and respond to public health emergencies and other risks. Identifying crises and the county's
existing shortcomings and instil specific protection and security facilities to provide essential
health and other social care services to citizens is necessary. Ensuring investment in
international health capacities to include and develop skills of national and international
health workers when it comes to dealing with public health emergencies. (Thistlethwaite, et
al. 2019)
International Migration:
The demand for work health professionals in middle-income countries like India is likely to
continue and drive health worker migrations for the future years to come. If the commission
recognizes that the mobility of health workers brings with it a considerable amount of
benefits to the source as well the as the destination nations. It also helps the health workers
themselves as it includes the transformation of information and helps the health workers in
developing countries to grab more information on treatments and procedures. The only side
effect when it comes to migration through that is a transfer of capital as well as the problems
that arise in the migrant's rights. Outside India can be solved by a broader agreement on the
international workforce migration and try their best to take into consideration provisions that
are required to make this concept mutually beneficial for both the parties. It will optimize the
use of skills and thus increase the benefits of the same. (Walton-Roberts, et al. 2017).
Conclusion:
If India as a country has to achieve the basic need of 1:1000 ratio of a doctor to a patient and
fall in terms of the recommendations of the WHO, there is an actual need of almost 2.07
million doctors more by approximately 2030. With sparing 1.3% of the GDP by the
government for public healthcare instead of the average that is accepted globally which is of
6%, it only comes to the conclusion that there will be a shortage of government doctors
making the general public spend more on health and medical expenses and that too in a
private health care centre. A country like India that does not have the necessary services and
is in dire need of a good plan which will help it understand the challenges that would come
(Mason, et al. 2015).
Crises and humanitarian settings:
India should try to build and increase the capacity of its health force and systems to find out
and respond to public health emergencies and other risks. Identifying crises and the county's
existing shortcomings and instil specific protection and security facilities to provide essential
health and other social care services to citizens is necessary. Ensuring investment in
international health capacities to include and develop skills of national and international
health workers when it comes to dealing with public health emergencies. (Thistlethwaite, et
al. 2019)
International Migration:
The demand for work health professionals in middle-income countries like India is likely to
continue and drive health worker migrations for the future years to come. If the commission
recognizes that the mobility of health workers brings with it a considerable amount of
benefits to the source as well the as the destination nations. It also helps the health workers
themselves as it includes the transformation of information and helps the health workers in
developing countries to grab more information on treatments and procedures. The only side
effect when it comes to migration through that is a transfer of capital as well as the problems
that arise in the migrant's rights. Outside India can be solved by a broader agreement on the
international workforce migration and try their best to take into consideration provisions that
are required to make this concept mutually beneficial for both the parties. It will optimize the
use of skills and thus increase the benefits of the same. (Walton-Roberts, et al. 2017).
Conclusion:
If India as a country has to achieve the basic need of 1:1000 ratio of a doctor to a patient and
fall in terms of the recommendations of the WHO, there is an actual need of almost 2.07
million doctors more by approximately 2030. With sparing 1.3% of the GDP by the
government for public healthcare instead of the average that is accepted globally which is of
6%, it only comes to the conclusion that there will be a shortage of government doctors
making the general public spend more on health and medical expenses and that too in a
private health care centre. A country like India that does not have the necessary services and
is in dire need of a good plan which will help it understand the challenges that would come
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

up in the following years due to the growing population. Emphasizing a workforce planning
strategy will not only help India but also the people of the Country.
strategy will not only help India but also the people of the Country.
Reference:
Addicott, R., Maguire, D., Honeyman, M., &Jabbal, J. (2015). Workforce planning in the
NHS. King's Fund.
Buchan, J., Twigg, D., Dussault, G., Duffield, C., & Stone, P. W. (2015). Policies to
sustain the nursing workforce: an international perspective. International nursing
review, 62(2), 162-170.
De Bruecker, P., Van den Bergh, J., Beliën, J., &Demeulemeester, E. (2015). Workforce
planning incorporating skills: State of the art. European Journal of Operational
Research, 243(1), 1-16.
Fan, V., & Anand, S., (2016). The health workforce in India.
Hou, J., &Ke, Y. (2015). Addressing the shortage of health professionals in rural China:
issues and progress: Comment on" Have human health resources become more equal
between rural and urban areas after the new reform?". International journal of health
policy and management, 4(5), 327.
Joumard, I., & Kumar, A. (2015). Improving health outcomes and health care in India.
Lopes, M. A., Almeida, Á. S. & Almada-Lobo, B. (2015). Handling healthcare
workforce planning with care: where do we stand?. Human resources for
health, 13(1), 38.
Mason, T., Sutton, M., Whittaker, W., & Birch, S. (2015). Exploring the limitations of
age-based models for health care planning. Social Science & Medicine, 132, 11-19.
Pozo-Martin, F., Nove, A., Lopes, S. C., Campbell, J., Buchan, J., Dussault, G., ...
&Siyam, A., (2017). Health workforce metrics pre-and post-2015: a stimulus to
public policy and planning. Human resources for health, 15(1), 14.
Rao, K. D., Shahrawat, R., & Bhatnagar, A. (2016). Composition and distribution of the
health workforce in India: estimates based on data from the National Sample
Survey. WHO South-East Asia journal of public health, 5(2), 133.
Squires, A., Jylhä, V., Jun, J., Ensio, A., &Kinnunen, J. (2017). A scoping review of
nursing workforce planning and forecasting research. Journal of nursing
management, 25(8), 587-596.
Thistlethwaite, J. E., Dunston, R., & Yassine, T. (2019). The times are changing:
workforce planning, new health-care models and the need for interprofessional
education in Australia. Journal of interprofessional care, 1-8.
Addicott, R., Maguire, D., Honeyman, M., &Jabbal, J. (2015). Workforce planning in the
NHS. King's Fund.
Buchan, J., Twigg, D., Dussault, G., Duffield, C., & Stone, P. W. (2015). Policies to
sustain the nursing workforce: an international perspective. International nursing
review, 62(2), 162-170.
De Bruecker, P., Van den Bergh, J., Beliën, J., &Demeulemeester, E. (2015). Workforce
planning incorporating skills: State of the art. European Journal of Operational
Research, 243(1), 1-16.
Fan, V., & Anand, S., (2016). The health workforce in India.
Hou, J., &Ke, Y. (2015). Addressing the shortage of health professionals in rural China:
issues and progress: Comment on" Have human health resources become more equal
between rural and urban areas after the new reform?". International journal of health
policy and management, 4(5), 327.
Joumard, I., & Kumar, A. (2015). Improving health outcomes and health care in India.
Lopes, M. A., Almeida, Á. S. & Almada-Lobo, B. (2015). Handling healthcare
workforce planning with care: where do we stand?. Human resources for
health, 13(1), 38.
Mason, T., Sutton, M., Whittaker, W., & Birch, S. (2015). Exploring the limitations of
age-based models for health care planning. Social Science & Medicine, 132, 11-19.
Pozo-Martin, F., Nove, A., Lopes, S. C., Campbell, J., Buchan, J., Dussault, G., ...
&Siyam, A., (2017). Health workforce metrics pre-and post-2015: a stimulus to
public policy and planning. Human resources for health, 15(1), 14.
Rao, K. D., Shahrawat, R., & Bhatnagar, A. (2016). Composition and distribution of the
health workforce in India: estimates based on data from the National Sample
Survey. WHO South-East Asia journal of public health, 5(2), 133.
Squires, A., Jylhä, V., Jun, J., Ensio, A., &Kinnunen, J. (2017). A scoping review of
nursing workforce planning and forecasting research. Journal of nursing
management, 25(8), 587-596.
Thistlethwaite, J. E., Dunston, R., & Yassine, T. (2019). The times are changing:
workforce planning, new health-care models and the need for interprofessional
education in Australia. Journal of interprofessional care, 1-8.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.