NUR250 S1 2018 Assessment 1: Patient Assessment and Care Planning
VerifiedAdded on 2021/04/21
|18
|3584
|27
Homework Assignment
AI Summary
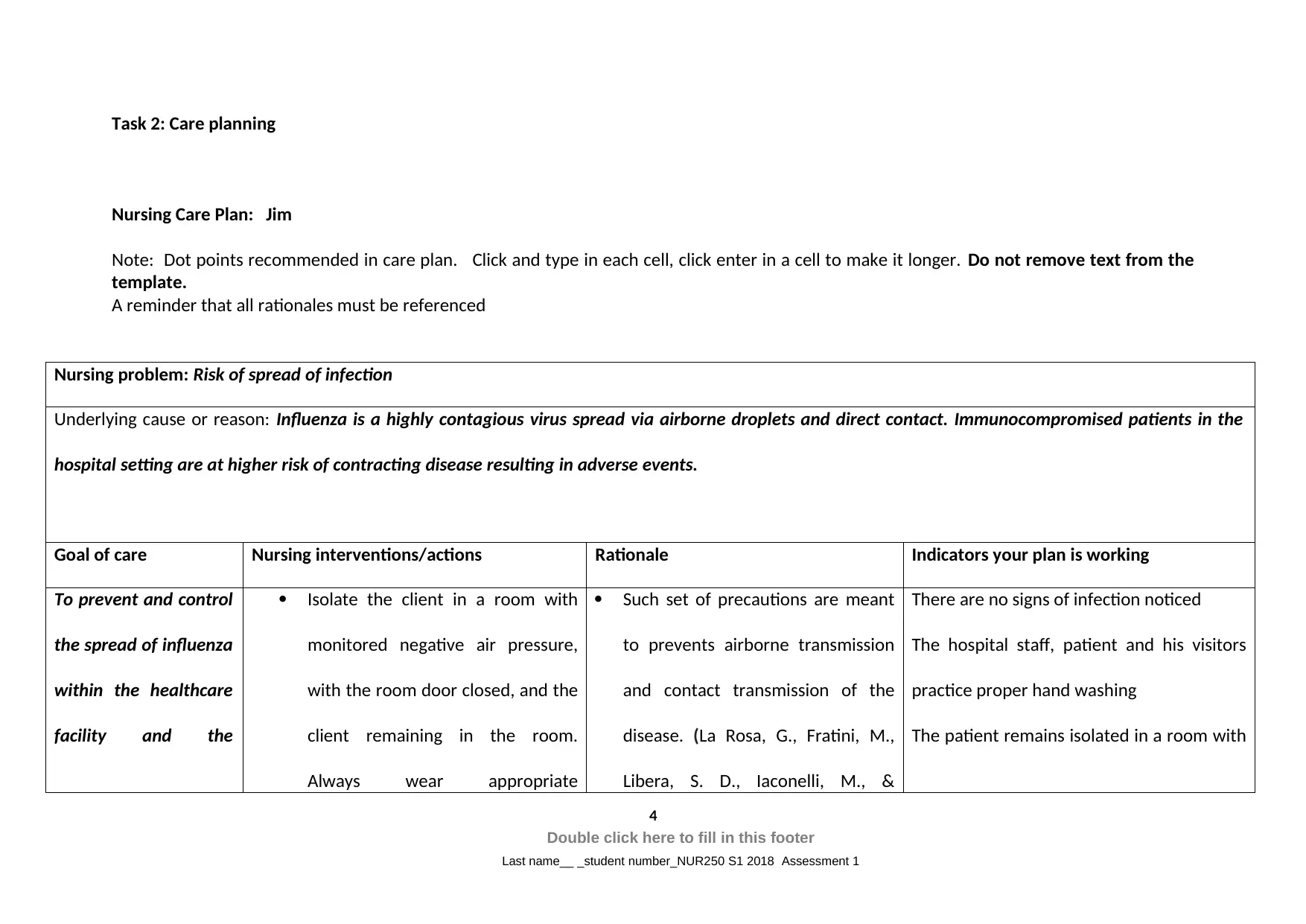
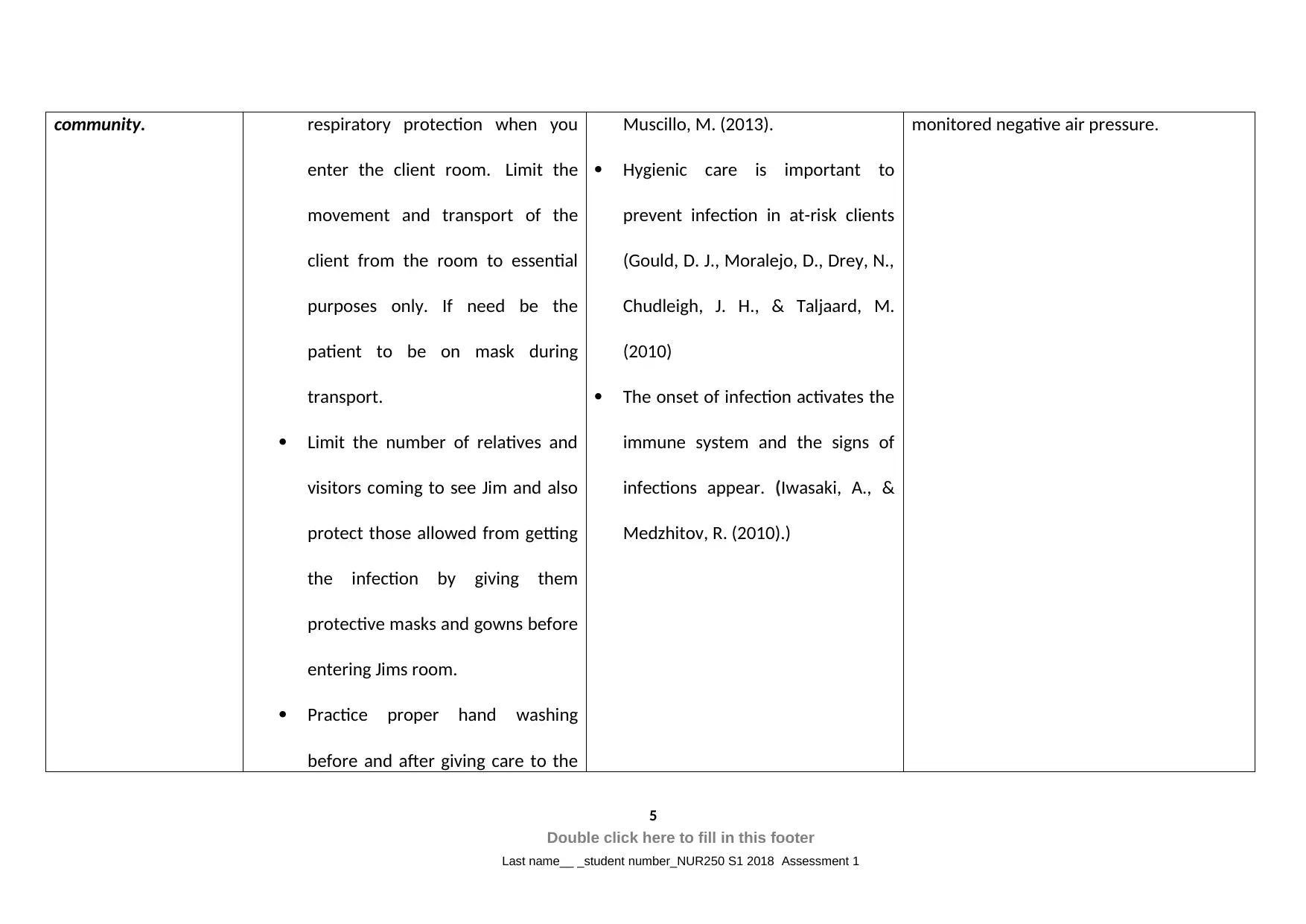
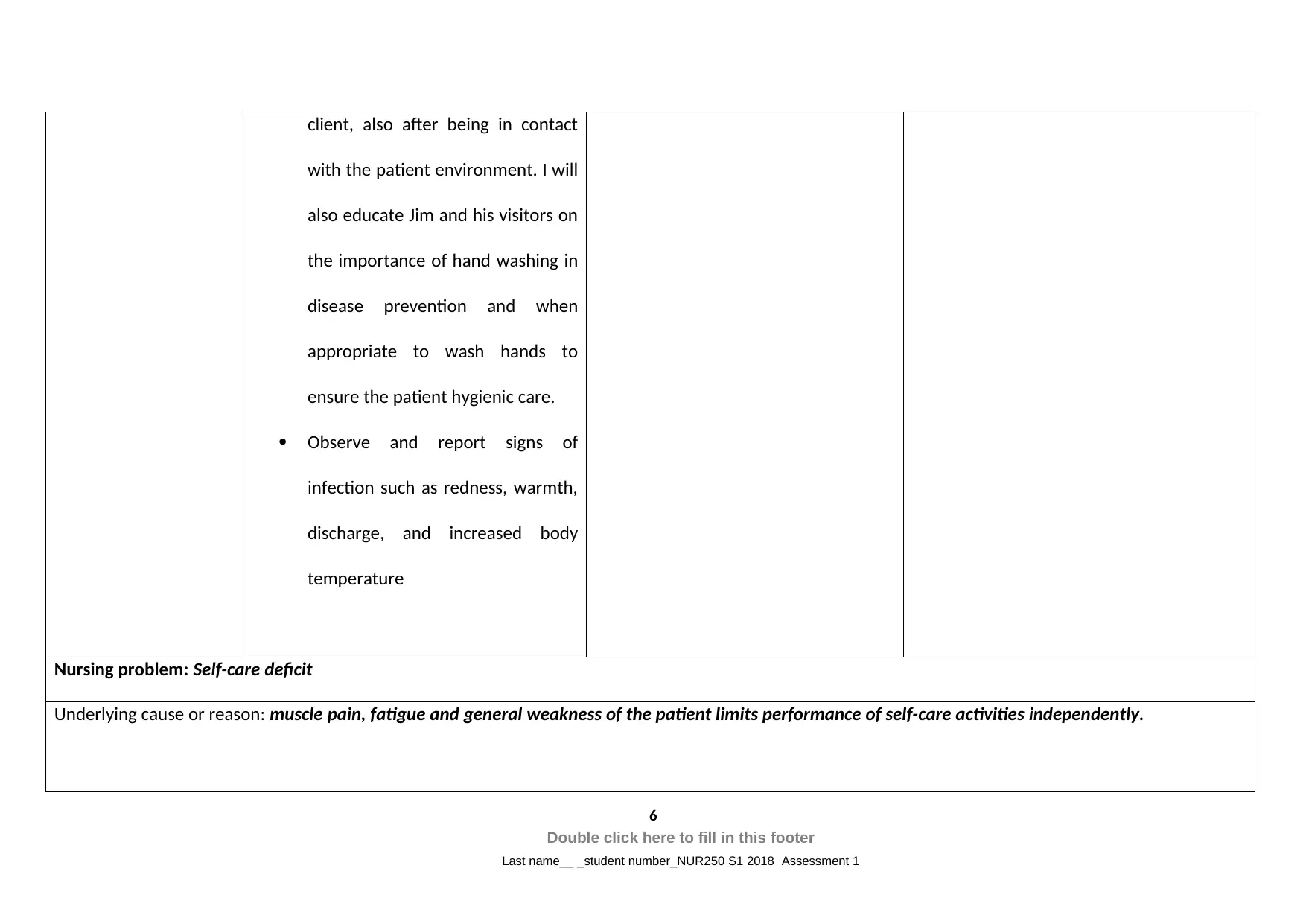
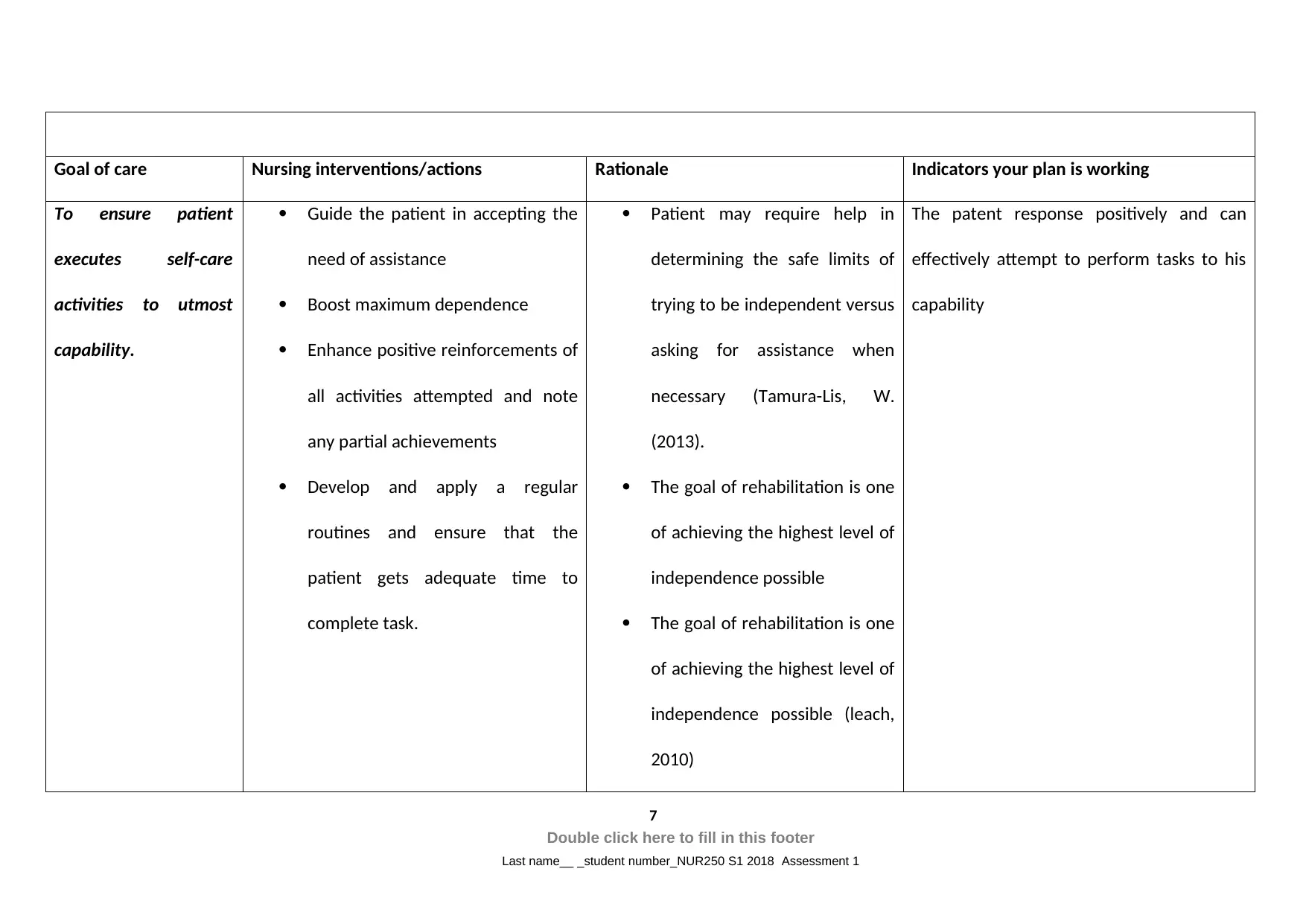
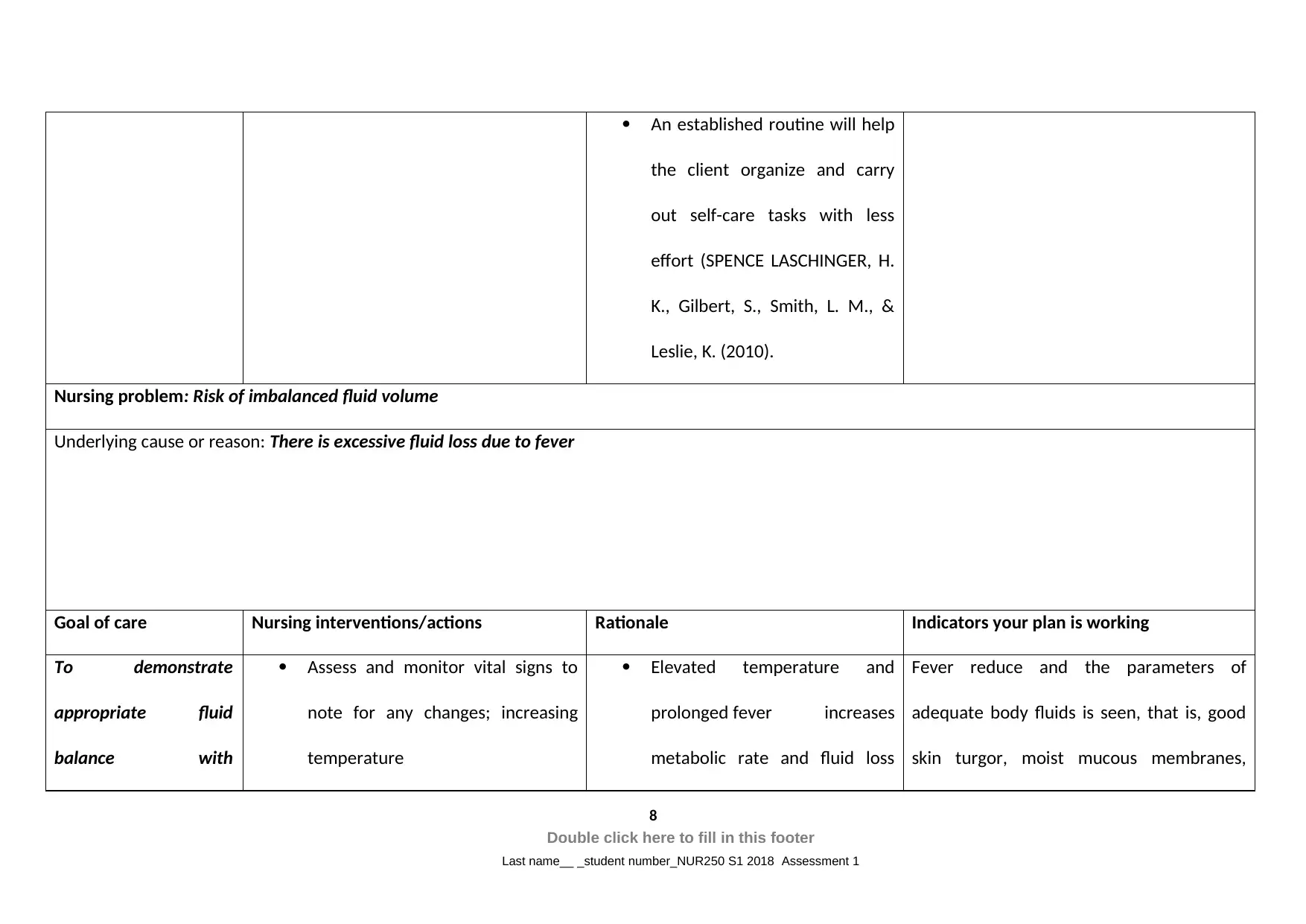
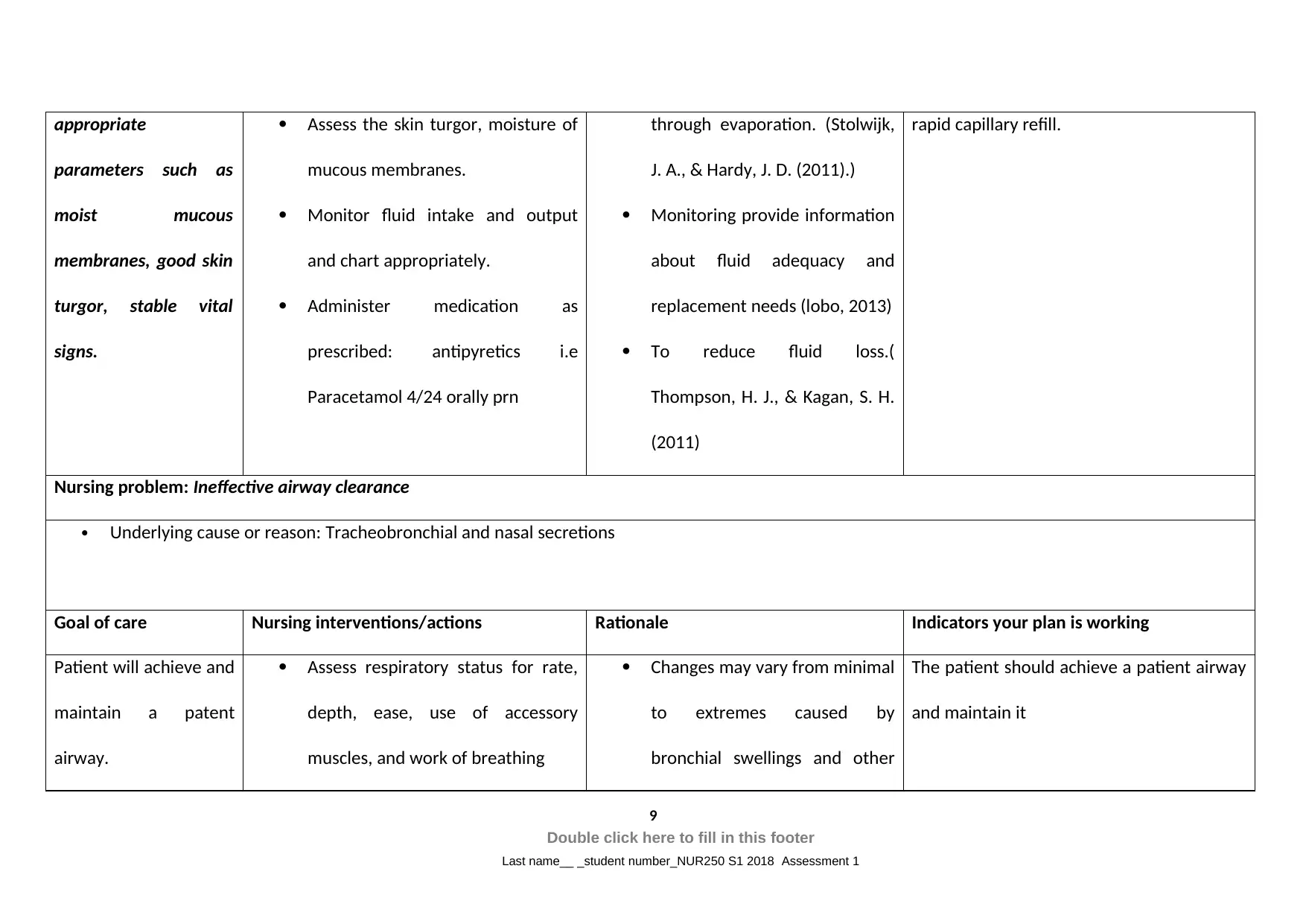
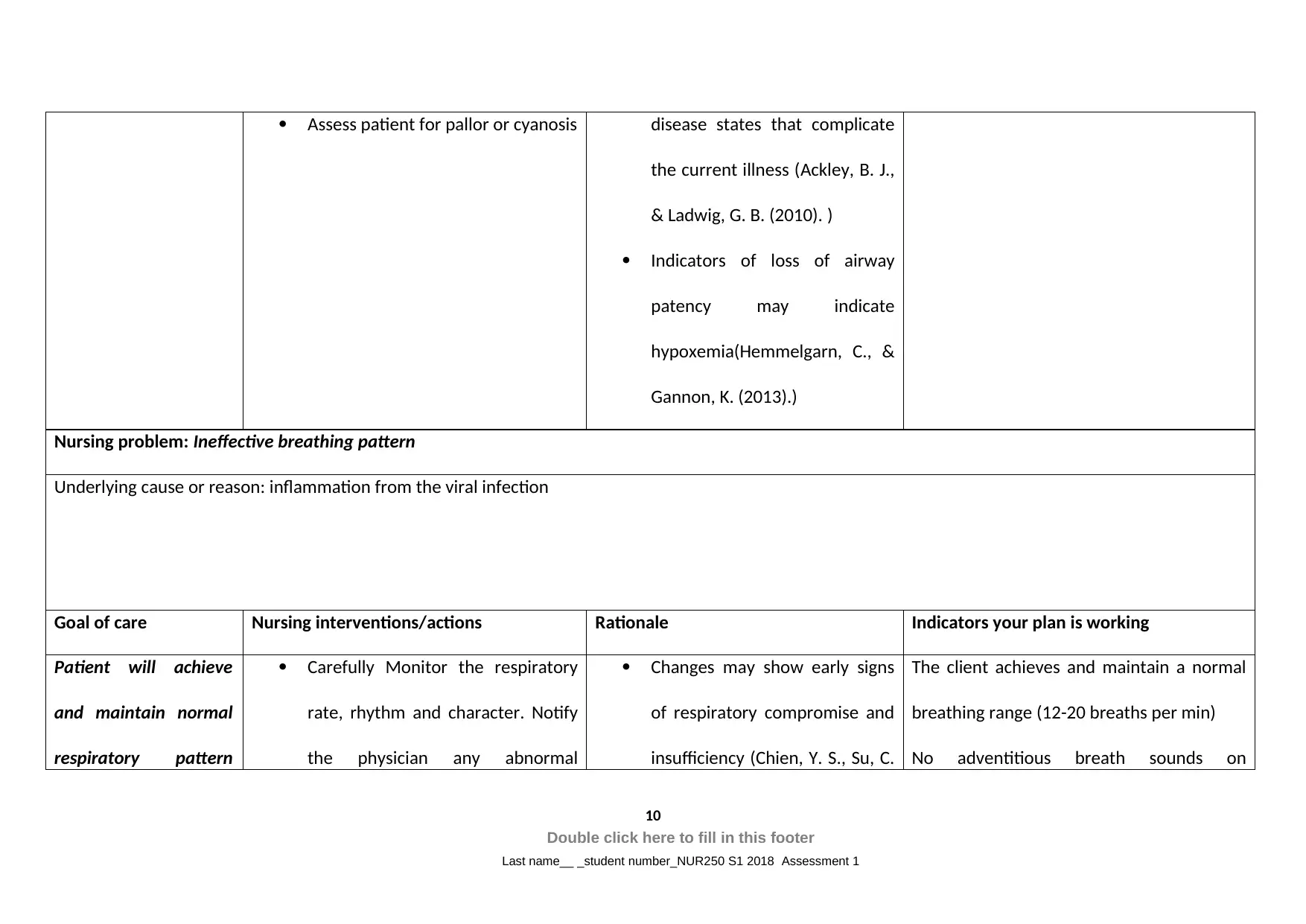
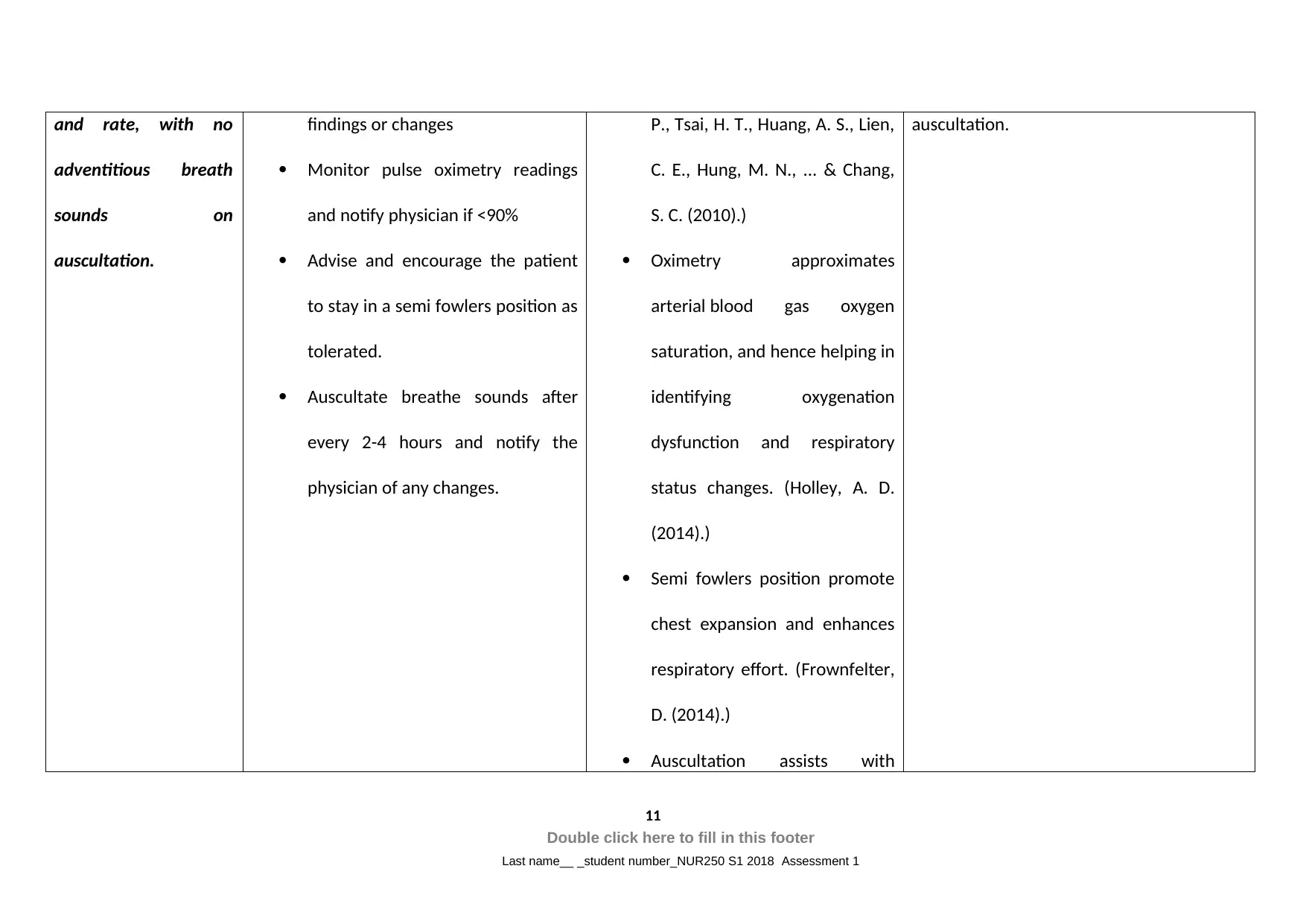
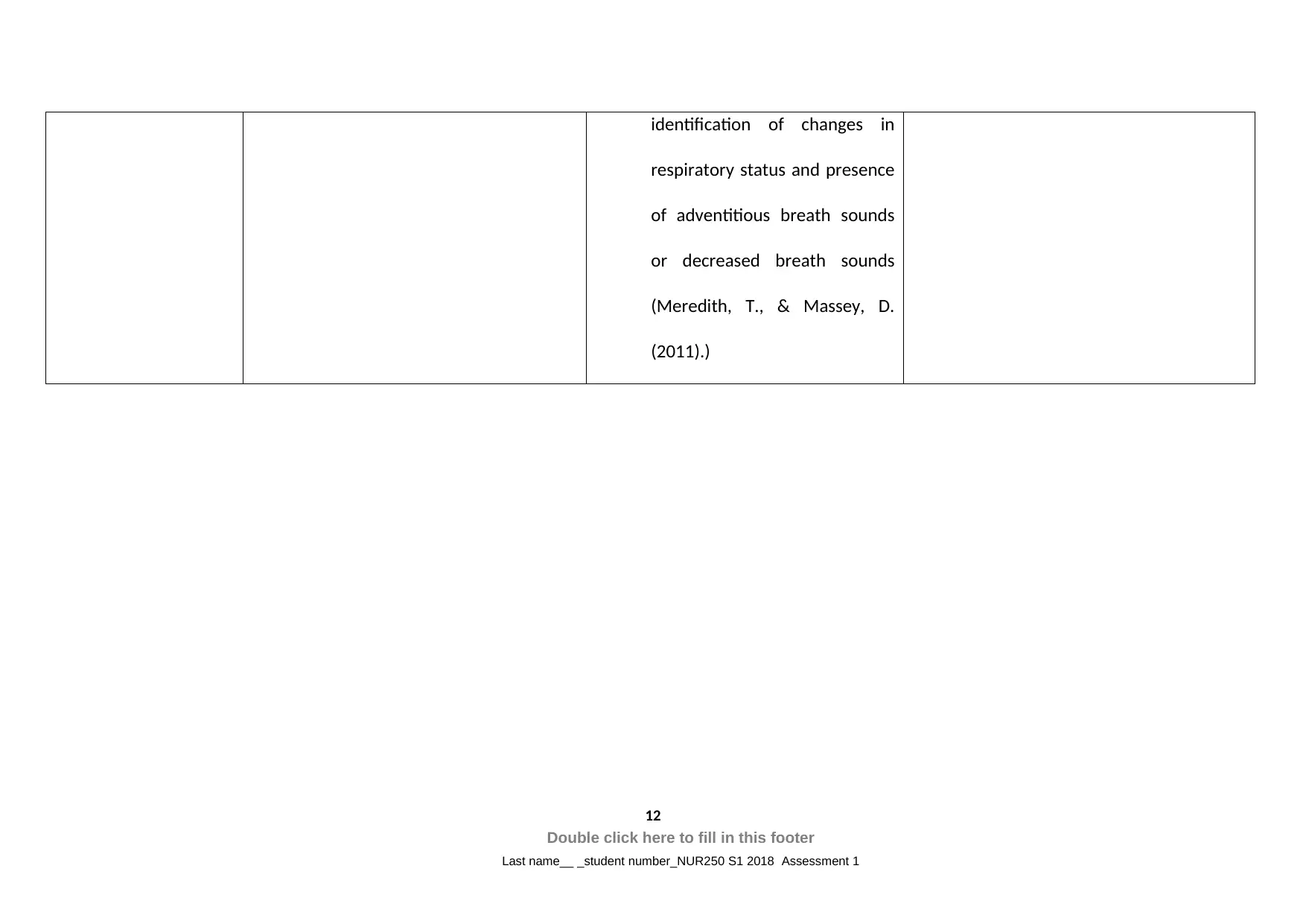
This assignment presents a comprehensive patient assessment and care plan for a patient, Jim, diagnosed with Influenza. The assessment focuses on identifying key nursing problems, including ineffective airway clearance, ineffective breathing pattern, hyperthermia, self-care deficit, risk of infection, and risk of imbalanced fluid volume. The care plan includes detailed nursing interventions, rationales, and expected outcomes for each identified problem, such as isolating the patient to prevent infection spread and encouraging self-care activities. The assignment also covers medication management, including the use of oseltamivir, paracetamol, and Fluvax IM, with considerations for dosage, side effects, and patient monitoring. Patient teaching is addressed, particularly focusing on the health implications of smoking and hypertension. The importance of patient education, including smoking cessation strategies, is emphasized to improve patient outcomes and prevent complications associated with influenza and related health issues. The assignment uses a problem-based approach, integrating evidence-based practices to ensure effective patient care.

1 out of 18
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.