Introduction to Epidemiology (401076) Assignment 1 Analysis
VerifiedAdded on 2020/02/24
|7
|1944
|261
Homework Assignment
AI Summary
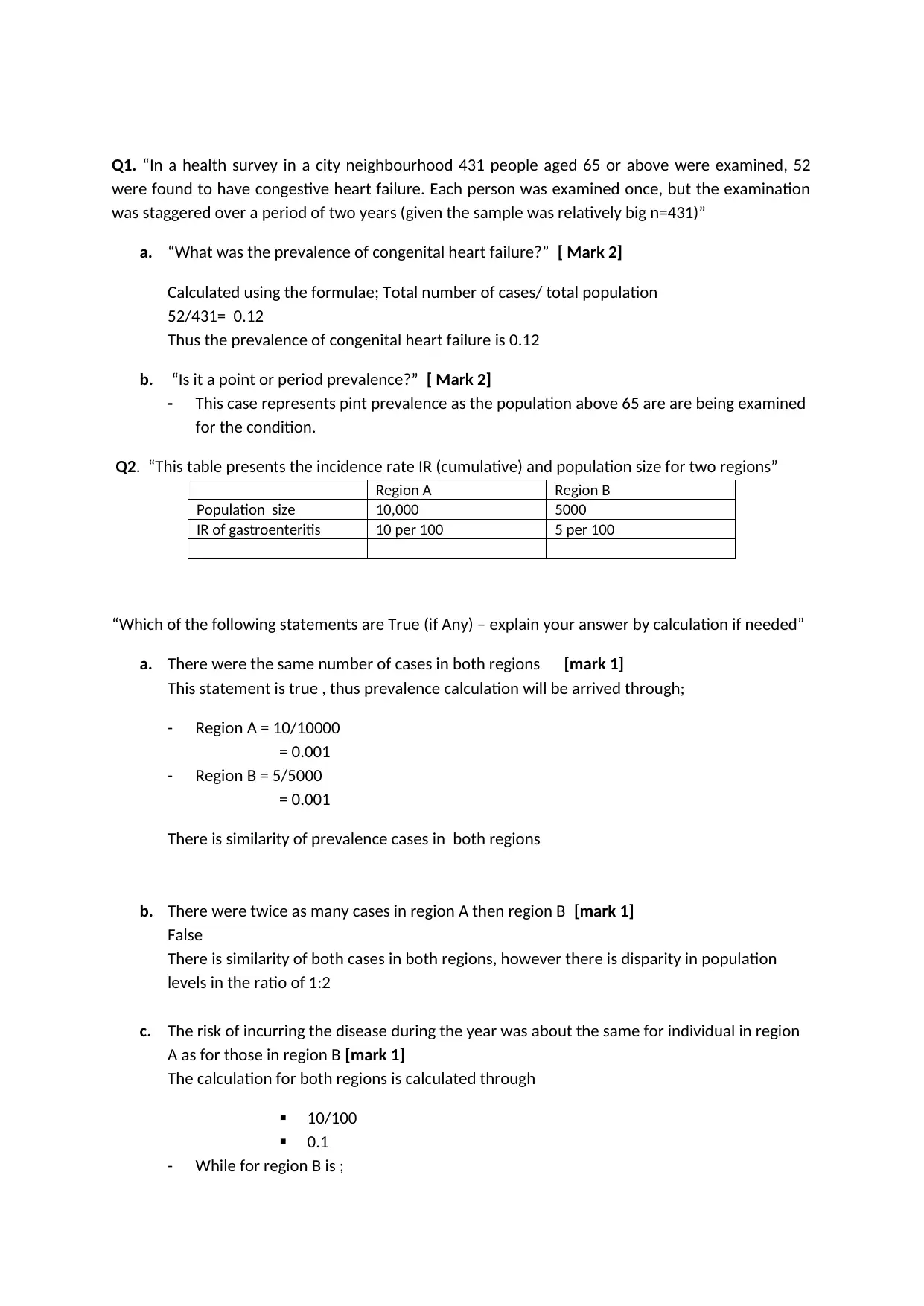
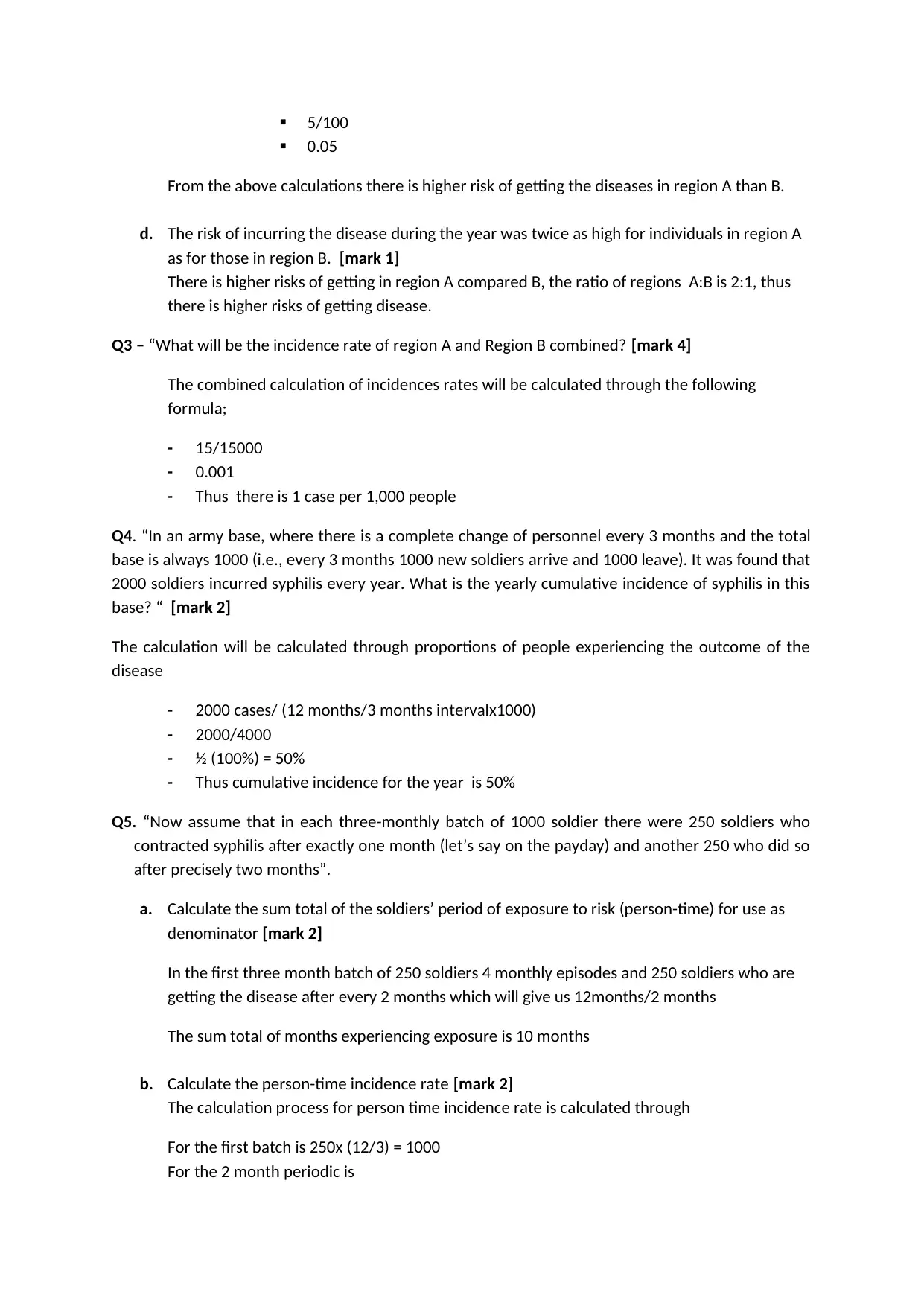
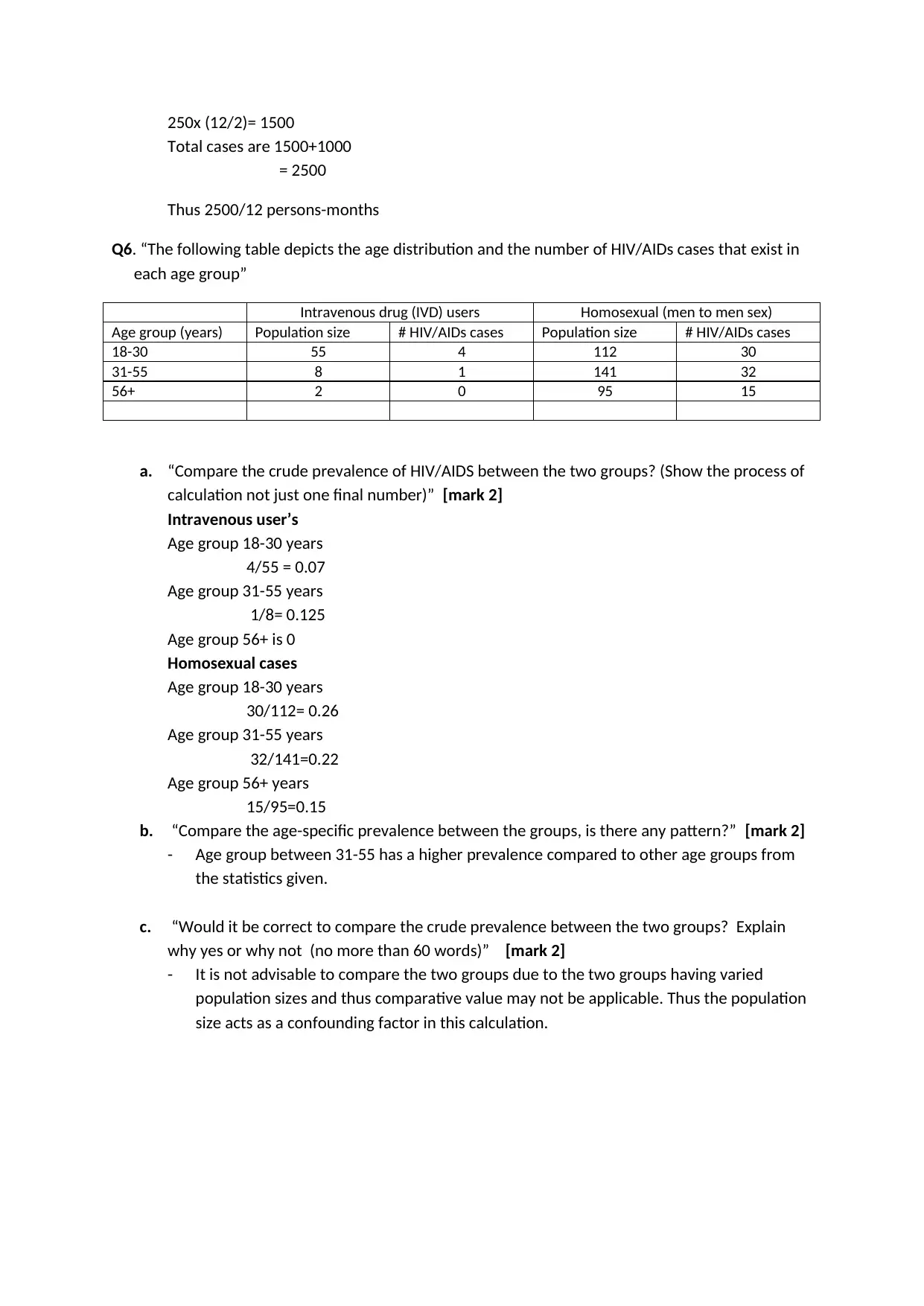
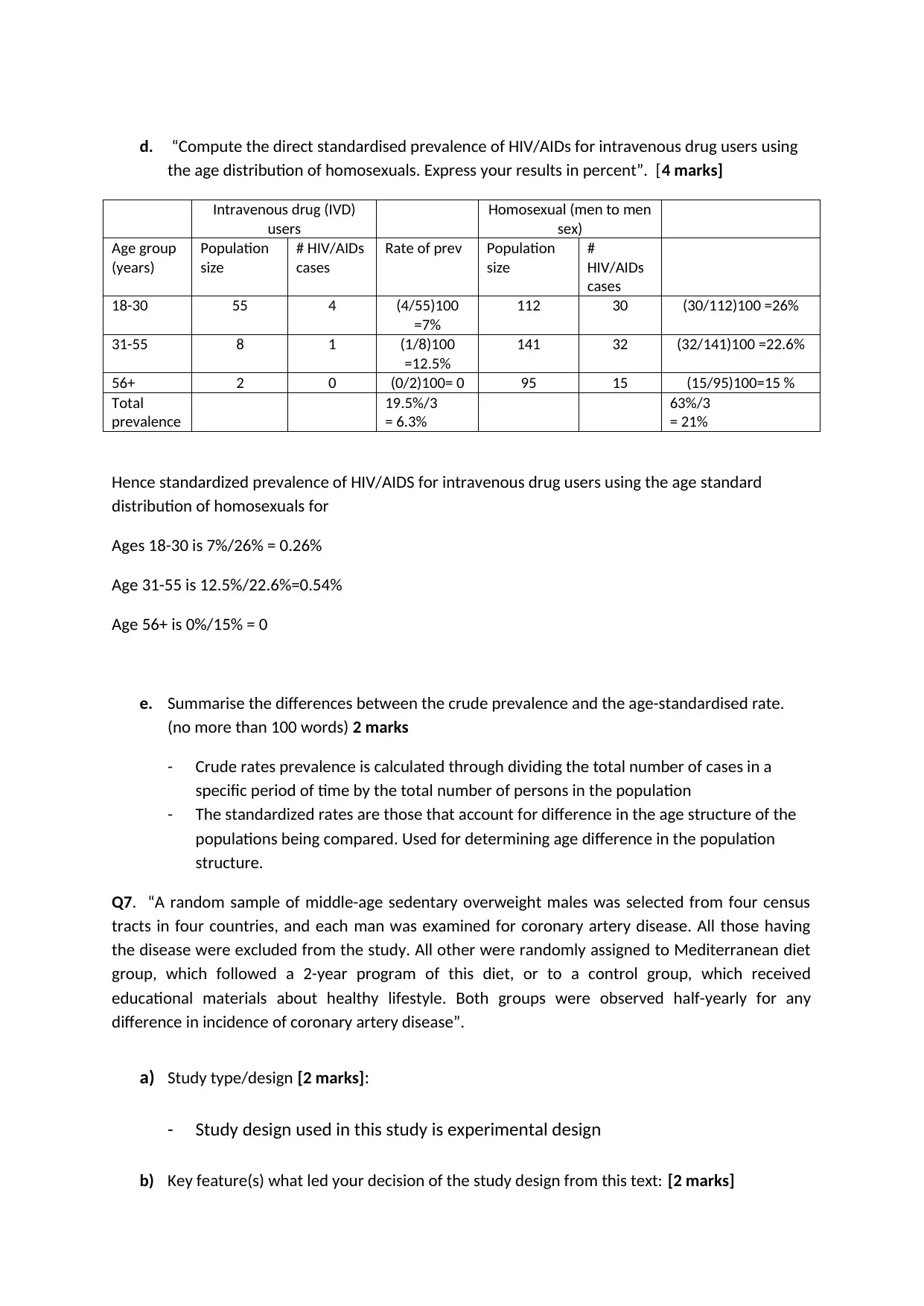
This document presents a complete solution to an Introduction to Epidemiology assignment from the University of Western Sydney. The assignment covers various epidemiological concepts, including calculating prevalence (both point and period), incidence rates (cumulative and person-time), and comparing prevalence between different groups. The solution includes detailed calculations for questions involving congenital heart failure, gastroenteritis, syphilis, and HIV/AIDS. Furthermore, the assignment explores different study designs, such as experimental and quasi-experimental designs, and requires analysis of research abstracts to identify research questions, exposures, outcomes, and study designs. The solution provides clear explanations and calculations for each question, demonstrating a strong understanding of epidemiological principles and their application in public health contexts.

1 out of 7
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.