Pharmacology Presentation: Ketamine Route of Administration
VerifiedAdded on 2023/06/08
|11
|2323
|203
Presentation
AI Summary
This presentation provides a detailed overview of ketamine's journey through the human body, starting with its classification as a Schedule 3 compound and NMDA receptor antagonist. It explores the drug's chemistry, prime and secondary effects, and half-life, as well as its legal and illicit accessibility. The presentation then traces ketamine's route of administration, detailing how it enters the circulatory system via oral, intravenous, or other routes, and how it is distributed throughout the body, including its passage through the blood-brain barrier. The mechanism of action at the site of action is explained, focusing on its role as an NMDA receptor antagonist. The presentation further explains the metabolism of ketamine in organs and tissues, primarily the liver, and its excretion through urine and faeces. The presentation concludes by referencing key sources, offering a comprehensive understanding of ketamine's pharmacokinetics. Desklib is a great resource for students looking for similar solved assignments.

Running Head: KETAMINE ROUTE OF ADMINISTRATION 1
Ketamine Route Of Administration
Author’s Name
Institution
Date
Ketamine Route Of Administration
Author’s Name
Institution
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
KETAMINE ROUTE OF ADMINISTRATION 2
Ketamine Drug Information
Drug Classification
Ketamine is classified as a Schedule 3 Compound that is used for starting as well as
maintaining an anaesthesia. The drug class is an NMDA receptor antagonist that is used as a
general anaesthesia (Tripathi, 2013). Ketamine is also classified as a dissociative which is the
class of hallucinogen. The drug is also classified as a sedative, analgesic and antidepressants
(Harold, 2015).
Chemistry
The chemical structure of Ketamine makes it be classified as an arylcyclohexylamine
derivative. The drug has a chiral compound. The pharmaceutical preparations of this medicine
are racemic but some preparations have differences in enantiomer proportions. The most active
enantiomer is ketamine (S-Ketamine) and the less active enantiomer is ketamine (R-Ketamine)
that is sold as an enantiopure drug used for clinical purposes (Harold, 2015).
The images below shows structural representation of ketamine (Katzung & Trevor, 2015).
Skeletal Formula of (R)-Ketamine
Ball-and-Stick Model of (R)-Ketamine
Ketamine Drug Information
Drug Classification
Ketamine is classified as a Schedule 3 Compound that is used for starting as well as
maintaining an anaesthesia. The drug class is an NMDA receptor antagonist that is used as a
general anaesthesia (Tripathi, 2013). Ketamine is also classified as a dissociative which is the
class of hallucinogen. The drug is also classified as a sedative, analgesic and antidepressants
(Harold, 2015).
Chemistry
The chemical structure of Ketamine makes it be classified as an arylcyclohexylamine
derivative. The drug has a chiral compound. The pharmaceutical preparations of this medicine
are racemic but some preparations have differences in enantiomer proportions. The most active
enantiomer is ketamine (S-Ketamine) and the less active enantiomer is ketamine (R-Ketamine)
that is sold as an enantiopure drug used for clinical purposes (Harold, 2015).
The images below shows structural representation of ketamine (Katzung & Trevor, 2015).
Skeletal Formula of (R)-Ketamine
Ball-and-Stick Model of (R)-Ketamine
KETAMINE ROUTE OF ADMINISTRATION 3
Skeletal Formula of (S)-Ketamine
Ball-and-Stick Model of (R)-Ketamine
Prime Effects
• Ketamine has a trance-like effect
• Pain relief (Bell, Eccleston & Kalso, 2012).
• Sedation effects
• Memory loss
• Gastrointestinal effects that include vomiting, increased salivation, decreased appetite and
nausea.
Skeletal Formula of (S)-Ketamine
Ball-and-Stick Model of (R)-Ketamine
Prime Effects
• Ketamine has a trance-like effect
• Pain relief (Bell, Eccleston & Kalso, 2012).
• Sedation effects
• Memory loss
• Gastrointestinal effects that include vomiting, increased salivation, decreased appetite and
nausea.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
KETAMINE ROUTE OF ADMINISTRATION 4
• Cardiovascular effects since it stimulates the sympathetic nervous system hence leading to
cardiovascular changes.
• Euphoria
• Anxiety (Harold, 2015).
Secondary Effects
• Agitation
• Vivid dreams
• Increased blood pressure
• Respiratory effects like the decrease in breathing, airway obstruction, spasms of the larynx
and increased bronchial secretions
• Confusion
• Hallucinations
• Muscle tremors
• Dependence (Morgan, Curran & Independent Scientific Committee on Drugs (ISCD), 2012).
• Dermatological effects such as reddening of the skin and rash
• Ocular effects- double vision, tunnel vision, involuntary movements of the eyes and rise in
intraocular pressure.
• Urinary incontinence (Harold, 2015).
Half-Life
• Cardiovascular effects since it stimulates the sympathetic nervous system hence leading to
cardiovascular changes.
• Euphoria
• Anxiety (Harold, 2015).
Secondary Effects
• Agitation
• Vivid dreams
• Increased blood pressure
• Respiratory effects like the decrease in breathing, airway obstruction, spasms of the larynx
and increased bronchial secretions
• Confusion
• Hallucinations
• Muscle tremors
• Dependence (Morgan, Curran & Independent Scientific Committee on Drugs (ISCD), 2012).
• Dermatological effects such as reddening of the skin and rash
• Ocular effects- double vision, tunnel vision, involuntary movements of the eyes and rise in
intraocular pressure.
• Urinary incontinence (Harold, 2015).
Half-Life
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
KETAMINE ROUTE OF ADMINISTRATION 5
The half-life of ketamine is between 2-3 hours and that of norketamine is about 12 hours.
Ketamine takes almost 4 hours in the body before half of the drug is removed from the body such
that the serum concentration is reduced due to metabolism and excretion (elimination).
Accessibility (Legal or Illicit)
Ketamine is legally marketed in most of the countries to be used for medical purposes.
However, in many countries due to the use of the drug as a drug of abuse, it is a controlled
substance (Rang, Ritter, Flower & Henderson, 2014). Therefore one to acquire ketamine in these
countries where the substance is controlled, one has had a prescription and is illegal to sell, use
or to possess the drug without a prescription. Ketamine is a substance that is availed for use,
however, it requires restriction of the production, supply, distribution, ownership and use so that
to decrease cases of ketamine abuse, misuse and also eradicate psychological or physical
dependence. For instance, in Canada ketamine has been classified as a Schedule 1 narcotic since
the year 2005. In Australia, ketamine is a schedule 8 controlled drug from October 2015 under
the Poisons Standard. The drug is a frequently abused recreational drug as it has dissociative
effects, tranquillizing as well as hallucinogenic effects hence there are many restrictions (Aan
Het Rot, Zarate Jr, Charney & Mathew, 2012).
Route of Administration
Ketamine is orally administered whereby 16% of the administered drug is absorbed. This
means that about 5 mg of the administered 30mg is orally absorbed. Other routes of Ketamine
administration include intravenous, subcutaneous, rectal, intranasal, epidural, sublingual and
intramuscular.
How The Drug Gets From The Point Of Entry Into The Circulatory System
The half-life of ketamine is between 2-3 hours and that of norketamine is about 12 hours.
Ketamine takes almost 4 hours in the body before half of the drug is removed from the body such
that the serum concentration is reduced due to metabolism and excretion (elimination).
Accessibility (Legal or Illicit)
Ketamine is legally marketed in most of the countries to be used for medical purposes.
However, in many countries due to the use of the drug as a drug of abuse, it is a controlled
substance (Rang, Ritter, Flower & Henderson, 2014). Therefore one to acquire ketamine in these
countries where the substance is controlled, one has had a prescription and is illegal to sell, use
or to possess the drug without a prescription. Ketamine is a substance that is availed for use,
however, it requires restriction of the production, supply, distribution, ownership and use so that
to decrease cases of ketamine abuse, misuse and also eradicate psychological or physical
dependence. For instance, in Canada ketamine has been classified as a Schedule 1 narcotic since
the year 2005. In Australia, ketamine is a schedule 8 controlled drug from October 2015 under
the Poisons Standard. The drug is a frequently abused recreational drug as it has dissociative
effects, tranquillizing as well as hallucinogenic effects hence there are many restrictions (Aan
Het Rot, Zarate Jr, Charney & Mathew, 2012).
Route of Administration
Ketamine is orally administered whereby 16% of the administered drug is absorbed. This
means that about 5 mg of the administered 30mg is orally absorbed. Other routes of Ketamine
administration include intravenous, subcutaneous, rectal, intranasal, epidural, sublingual and
intramuscular.
How The Drug Gets From The Point Of Entry Into The Circulatory System
KETAMINE ROUTE OF ADMINISTRATION 6
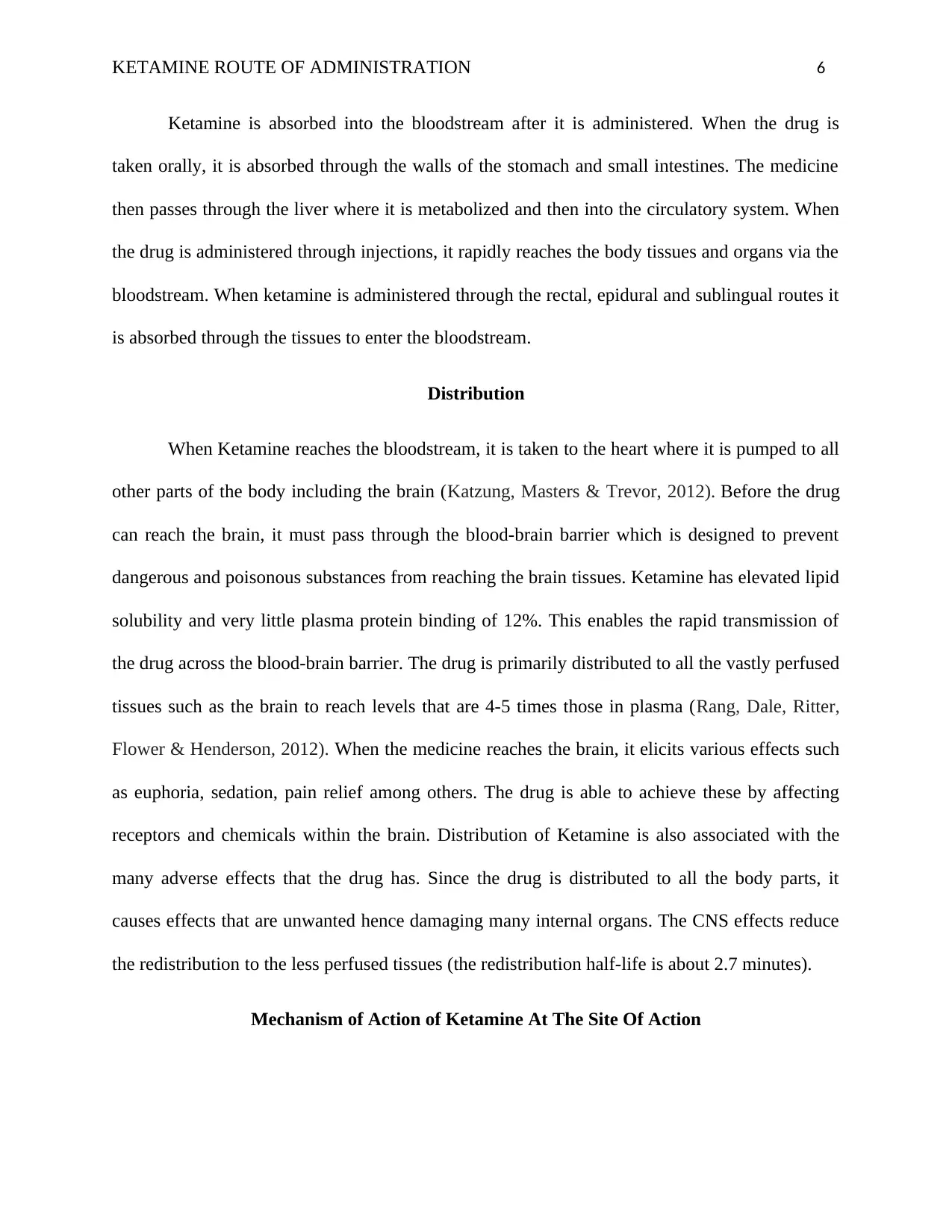
Ketamine is absorbed into the bloodstream after it is administered. When the drug is
taken orally, it is absorbed through the walls of the stomach and small intestines. The medicine
then passes through the liver where it is metabolized and then into the circulatory system. When
the drug is administered through injections, it rapidly reaches the body tissues and organs via the
bloodstream. When ketamine is administered through the rectal, epidural and sublingual routes it
is absorbed through the tissues to enter the bloodstream.
Distribution
When Ketamine reaches the bloodstream, it is taken to the heart where it is pumped to all
other parts of the body including the brain (Katzung, Masters & Trevor, 2012). Before the drug
can reach the brain, it must pass through the blood-brain barrier which is designed to prevent
dangerous and poisonous substances from reaching the brain tissues. Ketamine has elevated lipid
solubility and very little plasma protein binding of 12%. This enables the rapid transmission of
the drug across the blood-brain barrier. The drug is primarily distributed to all the vastly perfused
tissues such as the brain to reach levels that are 4-5 times those in plasma (Rang, Dale, Ritter,
Flower & Henderson, 2012). When the medicine reaches the brain, it elicits various effects such
as euphoria, sedation, pain relief among others. The drug is able to achieve these by affecting
receptors and chemicals within the brain. Distribution of Ketamine is also associated with the
many adverse effects that the drug has. Since the drug is distributed to all the body parts, it
causes effects that are unwanted hence damaging many internal organs. The CNS effects reduce
the redistribution to the less perfused tissues (the redistribution half-life is about 2.7 minutes).
Mechanism of Action of Ketamine At The Site Of Action
Ketamine is absorbed into the bloodstream after it is administered. When the drug is
taken orally, it is absorbed through the walls of the stomach and small intestines. The medicine
then passes through the liver where it is metabolized and then into the circulatory system. When
the drug is administered through injections, it rapidly reaches the body tissues and organs via the
bloodstream. When ketamine is administered through the rectal, epidural and sublingual routes it
is absorbed through the tissues to enter the bloodstream.
Distribution
When Ketamine reaches the bloodstream, it is taken to the heart where it is pumped to all
other parts of the body including the brain (Katzung, Masters & Trevor, 2012). Before the drug
can reach the brain, it must pass through the blood-brain barrier which is designed to prevent
dangerous and poisonous substances from reaching the brain tissues. Ketamine has elevated lipid
solubility and very little plasma protein binding of 12%. This enables the rapid transmission of
the drug across the blood-brain barrier. The drug is primarily distributed to all the vastly perfused
tissues such as the brain to reach levels that are 4-5 times those in plasma (Rang, Dale, Ritter,
Flower & Henderson, 2012). When the medicine reaches the brain, it elicits various effects such
as euphoria, sedation, pain relief among others. The drug is able to achieve these by affecting
receptors and chemicals within the brain. Distribution of Ketamine is also associated with the
many adverse effects that the drug has. Since the drug is distributed to all the body parts, it
causes effects that are unwanted hence damaging many internal organs. The CNS effects reduce
the redistribution to the less perfused tissues (the redistribution half-life is about 2.7 minutes).
Mechanism of Action of Ketamine At The Site Of Action
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
KETAMINE ROUTE OF ADMINISTRATION 7
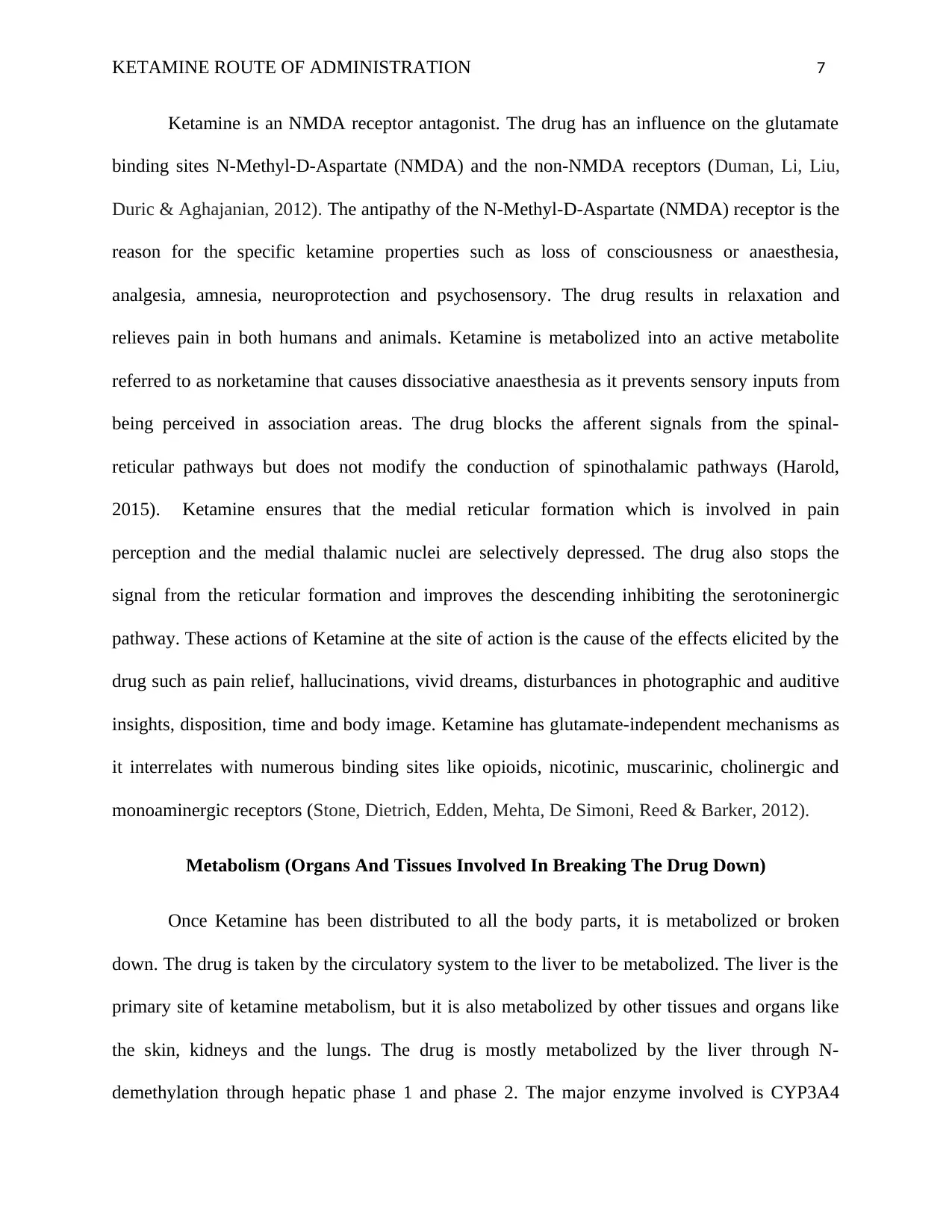
Ketamine is an NMDA receptor antagonist. The drug has an influence on the glutamate
binding sites N-Methyl-D-Aspartate (NMDA) and the non-NMDA receptors (Duman, Li, Liu,
Duric & Aghajanian, 2012). The antipathy of the N-Methyl-D-Aspartate (NMDA) receptor is the
reason for the specific ketamine properties such as loss of consciousness or anaesthesia,
analgesia, amnesia, neuroprotection and psychosensory. The drug results in relaxation and
relieves pain in both humans and animals. Ketamine is metabolized into an active metabolite
referred to as norketamine that causes dissociative anaesthesia as it prevents sensory inputs from
being perceived in association areas. The drug blocks the afferent signals from the spinal-
reticular pathways but does not modify the conduction of spinothalamic pathways (Harold,
2015). Ketamine ensures that the medial reticular formation which is involved in pain
perception and the medial thalamic nuclei are selectively depressed. The drug also stops the
signal from the reticular formation and improves the descending inhibiting the serotoninergic
pathway. These actions of Ketamine at the site of action is the cause of the effects elicited by the
drug such as pain relief, hallucinations, vivid dreams, disturbances in photographic and auditive
insights, disposition, time and body image. Ketamine has glutamate-independent mechanisms as
it interrelates with numerous binding sites like opioids, nicotinic, muscarinic, cholinergic and
monoaminergic receptors (Stone, Dietrich, Edden, Mehta, De Simoni, Reed & Barker, 2012).
Metabolism (Organs And Tissues Involved In Breaking The Drug Down)
Once Ketamine has been distributed to all the body parts, it is metabolized or broken
down. The drug is taken by the circulatory system to the liver to be metabolized. The liver is the
primary site of ketamine metabolism, but it is also metabolized by other tissues and organs like
the skin, kidneys and the lungs. The drug is mostly metabolized by the liver through N-
demethylation through hepatic phase 1 and phase 2. The major enzyme involved is CYP3A4
Ketamine is an NMDA receptor antagonist. The drug has an influence on the glutamate
binding sites N-Methyl-D-Aspartate (NMDA) and the non-NMDA receptors (Duman, Li, Liu,
Duric & Aghajanian, 2012). The antipathy of the N-Methyl-D-Aspartate (NMDA) receptor is the
reason for the specific ketamine properties such as loss of consciousness or anaesthesia,
analgesia, amnesia, neuroprotection and psychosensory. The drug results in relaxation and
relieves pain in both humans and animals. Ketamine is metabolized into an active metabolite
referred to as norketamine that causes dissociative anaesthesia as it prevents sensory inputs from
being perceived in association areas. The drug blocks the afferent signals from the spinal-
reticular pathways but does not modify the conduction of spinothalamic pathways (Harold,
2015). Ketamine ensures that the medial reticular formation which is involved in pain
perception and the medial thalamic nuclei are selectively depressed. The drug also stops the
signal from the reticular formation and improves the descending inhibiting the serotoninergic
pathway. These actions of Ketamine at the site of action is the cause of the effects elicited by the
drug such as pain relief, hallucinations, vivid dreams, disturbances in photographic and auditive
insights, disposition, time and body image. Ketamine has glutamate-independent mechanisms as
it interrelates with numerous binding sites like opioids, nicotinic, muscarinic, cholinergic and
monoaminergic receptors (Stone, Dietrich, Edden, Mehta, De Simoni, Reed & Barker, 2012).
Metabolism (Organs And Tissues Involved In Breaking The Drug Down)
Once Ketamine has been distributed to all the body parts, it is metabolized or broken
down. The drug is taken by the circulatory system to the liver to be metabolized. The liver is the
primary site of ketamine metabolism, but it is also metabolized by other tissues and organs like
the skin, kidneys and the lungs. The drug is mostly metabolized by the liver through N-
demethylation through hepatic phase 1 and phase 2. The major enzyme involved is CYP3A4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
KETAMINE ROUTE OF ADMINISTRATION 8
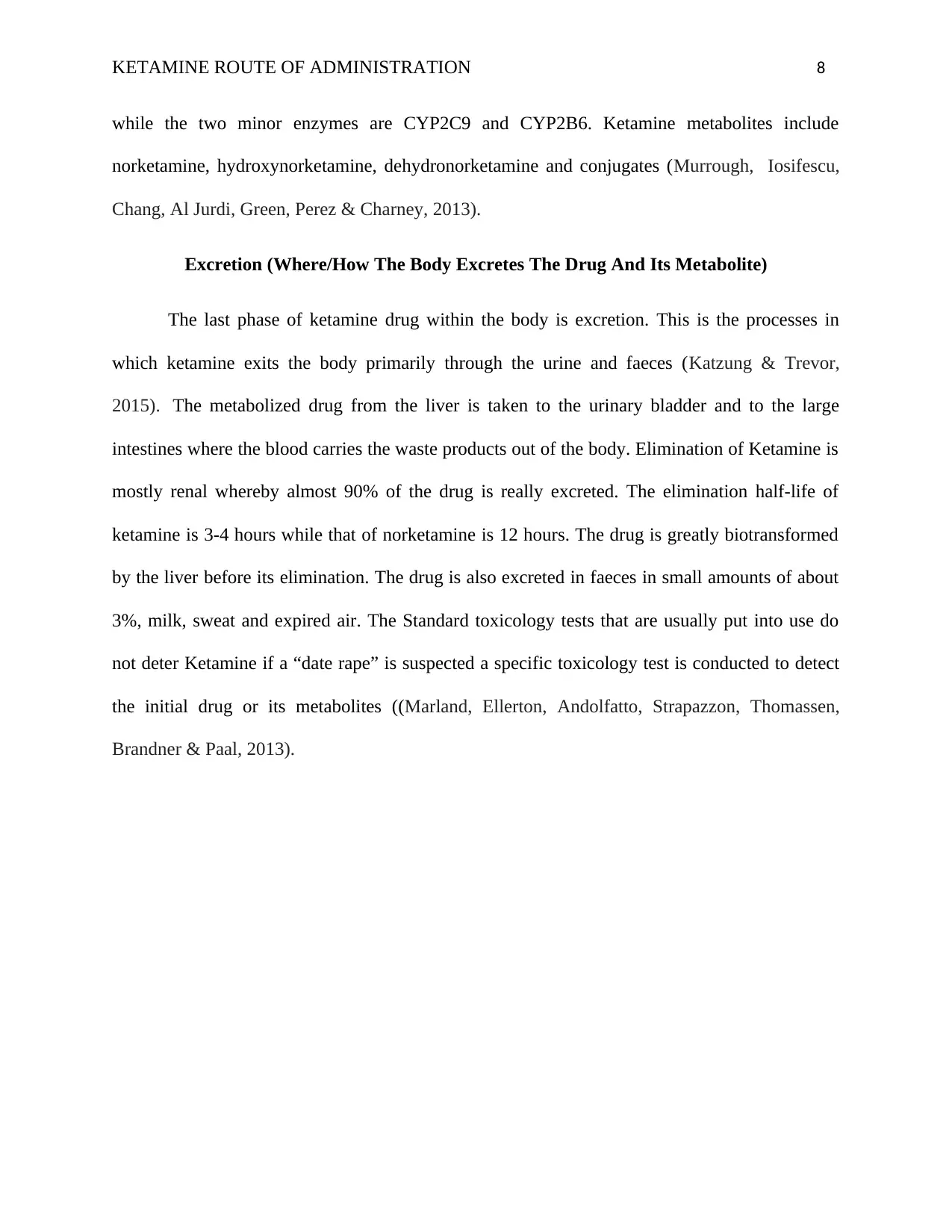
while the two minor enzymes are CYP2C9 and CYP2B6. Ketamine metabolites include
norketamine, hydroxynorketamine, dehydronorketamine and conjugates (Murrough, Iosifescu,
Chang, Al Jurdi, Green, Perez & Charney, 2013).
Excretion (Where/How The Body Excretes The Drug And Its Metabolite)
The last phase of ketamine drug within the body is excretion. This is the processes in
which ketamine exits the body primarily through the urine and faeces (Katzung & Trevor,
2015). The metabolized drug from the liver is taken to the urinary bladder and to the large
intestines where the blood carries the waste products out of the body. Elimination of Ketamine is
mostly renal whereby almost 90% of the drug is really excreted. The elimination half-life of
ketamine is 3-4 hours while that of norketamine is 12 hours. The drug is greatly biotransformed
by the liver before its elimination. The drug is also excreted in faeces in small amounts of about
3%, milk, sweat and expired air. The Standard toxicology tests that are usually put into use do
not deter Ketamine if a “date rape” is suspected a specific toxicology test is conducted to detect
the initial drug or its metabolites ((Marland, Ellerton, Andolfatto, Strapazzon, Thomassen,
Brandner & Paal, 2013).
while the two minor enzymes are CYP2C9 and CYP2B6. Ketamine metabolites include
norketamine, hydroxynorketamine, dehydronorketamine and conjugates (Murrough, Iosifescu,
Chang, Al Jurdi, Green, Perez & Charney, 2013).
Excretion (Where/How The Body Excretes The Drug And Its Metabolite)
The last phase of ketamine drug within the body is excretion. This is the processes in
which ketamine exits the body primarily through the urine and faeces (Katzung & Trevor,
2015). The metabolized drug from the liver is taken to the urinary bladder and to the large
intestines where the blood carries the waste products out of the body. Elimination of Ketamine is
mostly renal whereby almost 90% of the drug is really excreted. The elimination half-life of
ketamine is 3-4 hours while that of norketamine is 12 hours. The drug is greatly biotransformed
by the liver before its elimination. The drug is also excreted in faeces in small amounts of about
3%, milk, sweat and expired air. The Standard toxicology tests that are usually put into use do
not deter Ketamine if a “date rape” is suspected a specific toxicology test is conducted to detect
the initial drug or its metabolites ((Marland, Ellerton, Andolfatto, Strapazzon, Thomassen,
Brandner & Paal, 2013).
KETAMINE ROUTE OF ADMINISTRATION 9
References
Aan Het Rot, M., Zarate Jr, C. A., Charney, D. S., & Mathew, S. J. (2012). Ketamine for
depression: where do we go from here?. Biological psychiatry, 72(7), 537-547.
Becker, D. E., & Reed, K. L. (2012). Local anesthetics: review of pharmacological
considerations. Anesthesia progress, 59(2), 90-102.
Bell, R. F., Eccleston, C., & Kalso, E. A. (2012). Ketamine as an adjuvant to opioids for cancer
pain. The Cochrane database of systematic reviews, 11, CD003351-CD003351.
Duman, R. S., Li, N., Liu, R. J., Duric, V., & Aghajanian, G. (2012). Signaling pathways
underlying the rapid antidepressant actions of ketamine. Neuropharmacology, 62(1), 35-
41.
Harold E.D, (2015). Concepts of Chemical Dependency 9th Edition pp. 66-77
Katzung, B. G., & Trevor, A. J. (Eds.). (2015). Basic & clinical pharmacology (pp. 753-756).
New York, NY: McGraw-Hill.
Katzung, B. G., Masters, S. B., & Trevor, A. J. (2012). Basic and Clinical Pharmacology
(LANGE Basic Science). McGraw-Hill Education.
Marland, S., Ellerton, J., Andolfatto, G., Strapazzon, G., Thomassen, O., Brandner, B., ... & Paal,
P. (2013). Ketamine: use in anesthesia. CNS neuroscience & therapeutics, 19(6), 381-
389.
Morgan, C. J., Curran, H. V., & Independent Scientific Committee on Drugs (ISCD). (2012).
Ketamine use: a review. Addiction, 107(1), 27-38.
References
Aan Het Rot, M., Zarate Jr, C. A., Charney, D. S., & Mathew, S. J. (2012). Ketamine for
depression: where do we go from here?. Biological psychiatry, 72(7), 537-547.
Becker, D. E., & Reed, K. L. (2012). Local anesthetics: review of pharmacological
considerations. Anesthesia progress, 59(2), 90-102.
Bell, R. F., Eccleston, C., & Kalso, E. A. (2012). Ketamine as an adjuvant to opioids for cancer
pain. The Cochrane database of systematic reviews, 11, CD003351-CD003351.
Duman, R. S., Li, N., Liu, R. J., Duric, V., & Aghajanian, G. (2012). Signaling pathways
underlying the rapid antidepressant actions of ketamine. Neuropharmacology, 62(1), 35-
41.
Harold E.D, (2015). Concepts of Chemical Dependency 9th Edition pp. 66-77
Katzung, B. G., & Trevor, A. J. (Eds.). (2015). Basic & clinical pharmacology (pp. 753-756).
New York, NY: McGraw-Hill.
Katzung, B. G., Masters, S. B., & Trevor, A. J. (2012). Basic and Clinical Pharmacology
(LANGE Basic Science). McGraw-Hill Education.
Marland, S., Ellerton, J., Andolfatto, G., Strapazzon, G., Thomassen, O., Brandner, B., ... & Paal,
P. (2013). Ketamine: use in anesthesia. CNS neuroscience & therapeutics, 19(6), 381-
389.
Morgan, C. J., Curran, H. V., & Independent Scientific Committee on Drugs (ISCD). (2012).
Ketamine use: a review. Addiction, 107(1), 27-38.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
KETAMINE ROUTE OF ADMINISTRATION 10
Murrough, J. W., Iosifescu, D. V., Chang, L. C., Al Jurdi, R. K., Green, C. E., Perez, A. M., ... &
Charney, D. S. (2013). Antidepressant efficacy of ketamine in treatment-resistant major
depression: a two-site randomized controlled trial. American Journal of
Psychiatry, 170(10), 1134-1142.
Rang, H. P., Dale, M. M., Ritter, J. M., Flower, R. J., & Henderson, G. (2012). Antidepressant
drugs. Rang and Dale's pharmacology. 7th ed. Edinburgh: Elsevier/Churchill
Livingstone, 564-83.
Rang, H. P., Ritter, J. M., Flower, R. J., & Henderson, G. (2014). Rang & Dale's Pharmacology
E-Book: with STUDENT CONSULT Online Access. Elsevier Health Sciences.
Stone, J. M., Dietrich, C., Edden, R., Mehta, M. A., De Simoni, S., Reed, L. J., ... & Barker, G. J.
(2012). Ketamine effects on brain GABA and glutamate levels with 1H-MRS:
relationship to ketamine-induced psychopathology. Molecular psychiatry, 17(7), 664.
Tripathi, K. D. (2013). Essentials of medical pharmacology. JP Medical Ltd.
Zanos, P., Moaddel, R., Morris, P. J., Georgiou, P., Fischell, J., Elmer, G. I., ... & Dossou, K. S.
(2016). NMDAR inhibition-independent antidepressant actions of ketamine
metabolites. Nature, 533(7604), 481.
Murrough, J. W., Iosifescu, D. V., Chang, L. C., Al Jurdi, R. K., Green, C. E., Perez, A. M., ... &
Charney, D. S. (2013). Antidepressant efficacy of ketamine in treatment-resistant major
depression: a two-site randomized controlled trial. American Journal of
Psychiatry, 170(10), 1134-1142.
Rang, H. P., Dale, M. M., Ritter, J. M., Flower, R. J., & Henderson, G. (2012). Antidepressant
drugs. Rang and Dale's pharmacology. 7th ed. Edinburgh: Elsevier/Churchill
Livingstone, 564-83.
Rang, H. P., Ritter, J. M., Flower, R. J., & Henderson, G. (2014). Rang & Dale's Pharmacology
E-Book: with STUDENT CONSULT Online Access. Elsevier Health Sciences.
Stone, J. M., Dietrich, C., Edden, R., Mehta, M. A., De Simoni, S., Reed, L. J., ... & Barker, G. J.
(2012). Ketamine effects on brain GABA and glutamate levels with 1H-MRS:
relationship to ketamine-induced psychopathology. Molecular psychiatry, 17(7), 664.
Tripathi, K. D. (2013). Essentials of medical pharmacology. JP Medical Ltd.
Zanos, P., Moaddel, R., Morris, P. J., Georgiou, P., Fischell, J., Elmer, G. I., ... & Dossou, K. S.
(2016). NMDAR inhibition-independent antidepressant actions of ketamine
metabolites. Nature, 533(7604), 481.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

KETAMINE ROUTE OF ADMINISTRATION 11
1 out of 11

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.