Nursing Leadership and the Implementation of eMARs in Healthcare
VerifiedAdded on 2021/05/31
|22
|5484
|46
Report
AI Summary
This report examines nursing leadership in the context of medication management and the implementation of electronic medication administration records (eMARs). It begins with an introduction highlighting the significance of eMARs in reducing medication errors and improving patient safety. The discussion section delves into various leadership theories, including transformational and transactional leadership, and their suitability for driving change within healthcare settings. The report emphasizes the importance of leadership traits such as effective communication, fostering a team culture, and identifying champions during change implementation. A SWOT analysis is presented to evaluate the effects of the working environment on planned change with eMARs. The report also defines change management and its application in healthcare, highlighting the challenges and stresses associated with implementing new practices. Finally, the report provides a conclusion summarizing the key findings and insights discussed throughout the analysis.

0Running head: NURSING LEADERSHIP
Nursing Leadership
Name of the Student
Name of the University
Author Note
Nursing Leadership
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING LEADERSHIP
Table of Contents
Introduction................................................................................................................................2
Discussion..................................................................................................................................2
Leadership..............................................................................................................................2
Innovation in healthcare.........................................................................................................6
Change and change management...........................................................................................8
Use of evidence to support the change.................................................................................13
Conclusion................................................................................................................................14
References................................................................................................................................16
Appendix..................................................................................................................................20
SMART Goals......................................................................................................................20
Table of Contents
Introduction................................................................................................................................2
Discussion..................................................................................................................................2
Leadership..............................................................................................................................2
Innovation in healthcare.........................................................................................................6
Change and change management...........................................................................................8
Use of evidence to support the change.................................................................................13
Conclusion................................................................................................................................14
References................................................................................................................................16
Appendix..................................................................................................................................20
SMART Goals......................................................................................................................20
2NURSING LEADERSHIP
Introduction
According to Ashcroft et al (2015), medicines or drugs are the most commonly
employed clinical interventions under the healthcare settings. However, the use of drugs
towards the successful treatment of the patients is at times associated with sudden degree of
error. Berdot et al. (2012) argued that medication error can occur during, dispensing,
prescribing and administration of drug. The results of this medication error are fatal which
may lead to the development of chest aspiration, pneumonia or worse intracarnial
haemorrhage. In relation of medication management, Berdot et al. (2012) is of the opinion
that the drug error is the single most avoidable cause behind the subsequent patient’s harm. In
order to reduce the medication cost subsequent harm to patients electronic medication
administration records are gradually gaining importance (eMARs). According to Guo
Iribarren, Kapsandoy, Perri and Staggers (2011), eMARs can be used to support medication
management in order to decrease the rate of medication errors, while promoting patient safety
along with the improvement of the overall workflow efficiency.
Discussion
Leadership
According to Scully (2015), nursing is challenging yet dynamic profession which
demands engaging and inspiring leaders and role models. In present day ever changing yet
extremely demand healthcare environment, proper identification along with development of
appropriate nursing leadership is one of the biggest challenges experienced by the individuals
in the nursing profession. The overall concept of the nursing leadership is complex and has
multi-dimensional approach. Hutchinson and Jackson (2013) is of the opinion that effective
Introduction
According to Ashcroft et al (2015), medicines or drugs are the most commonly
employed clinical interventions under the healthcare settings. However, the use of drugs
towards the successful treatment of the patients is at times associated with sudden degree of
error. Berdot et al. (2012) argued that medication error can occur during, dispensing,
prescribing and administration of drug. The results of this medication error are fatal which
may lead to the development of chest aspiration, pneumonia or worse intracarnial
haemorrhage. In relation of medication management, Berdot et al. (2012) is of the opinion
that the drug error is the single most avoidable cause behind the subsequent patient’s harm. In
order to reduce the medication cost subsequent harm to patients electronic medication
administration records are gradually gaining importance (eMARs). According to Guo
Iribarren, Kapsandoy, Perri and Staggers (2011), eMARs can be used to support medication
management in order to decrease the rate of medication errors, while promoting patient safety
along with the improvement of the overall workflow efficiency.
Discussion
Leadership
According to Scully (2015), nursing is challenging yet dynamic profession which
demands engaging and inspiring leaders and role models. In present day ever changing yet
extremely demand healthcare environment, proper identification along with development of
appropriate nursing leadership is one of the biggest challenges experienced by the individuals
in the nursing profession. The overall concept of the nursing leadership is complex and has
multi-dimensional approach. Hutchinson and Jackson (2013) is of the opinion that effective
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING LEADERSHIP
nursing leadership is regarded as one of the essential factor towards achieving optimal patient
centred outcomes along with proper workplace enhancements. There are numerous nursing
leadership theories however, not all the nursing leadership theories align with all the
successful change implementation in the healthcare domains (Scully, 2015). According to
Grossman and Valiga (2016), transformational and transactional leadership are the two most
well-studied leadership theories in nursing professionals. Both the transformational and
transactional leadership theories span both the organisational and cultural boundaries and
have been critically validated and accessed in numerous studies.
Transformational leadership is akin to visionary and charismatic leadership. Leaders
who abide by the transformational leadership inspire, motivate their followers in manners that
extends beyond rewards and exchange. Transformational leadership executes expectionally
well under close supervisory relationships in comparison with more diverse relationships and
this closer supervision is more typical in order to implement certain administrative change
like the use of the eMARs in nursing health care settings. This integrated relationship may be
typical of a supervisee-supervisor relationship and is also captured under the notion of “first
level leaders” who are thought to be important due to their effective functional proximity
with their supervisees under a particular healthcare setting (Hutchinson & Jackson, 2013).
Hutchinson and Jackson (2013) argued that transformational leadership increases the overall
intrinsic motivation via expression of the importance along with the values of the leader’s
goals and thereby helping to implement the change. Transformational leadership will be best
suited in order to implement change in medication management via eMARs because
transformational leader has been described as an engaging leader who develops the followers
via creating a proper vision that generates meaning towards the change along with proper
motivation. Via stating a promising vision along with proper enthusiasm and accurate
confidence, transformative leaders are said to develop a firm sense of identification within the
nursing leadership is regarded as one of the essential factor towards achieving optimal patient
centred outcomes along with proper workplace enhancements. There are numerous nursing
leadership theories however, not all the nursing leadership theories align with all the
successful change implementation in the healthcare domains (Scully, 2015). According to
Grossman and Valiga (2016), transformational and transactional leadership are the two most
well-studied leadership theories in nursing professionals. Both the transformational and
transactional leadership theories span both the organisational and cultural boundaries and
have been critically validated and accessed in numerous studies.
Transformational leadership is akin to visionary and charismatic leadership. Leaders
who abide by the transformational leadership inspire, motivate their followers in manners that
extends beyond rewards and exchange. Transformational leadership executes expectionally
well under close supervisory relationships in comparison with more diverse relationships and
this closer supervision is more typical in order to implement certain administrative change
like the use of the eMARs in nursing health care settings. This integrated relationship may be
typical of a supervisee-supervisor relationship and is also captured under the notion of “first
level leaders” who are thought to be important due to their effective functional proximity
with their supervisees under a particular healthcare setting (Hutchinson & Jackson, 2013).
Hutchinson and Jackson (2013) argued that transformational leadership increases the overall
intrinsic motivation via expression of the importance along with the values of the leader’s
goals and thereby helping to implement the change. Transformational leadership will be best
suited in order to implement change in medication management via eMARs because
transformational leader has been described as an engaging leader who develops the followers
via creating a proper vision that generates meaning towards the change along with proper
motivation. Via stating a promising vision along with proper enthusiasm and accurate
confidence, transformative leaders are said to develop a firm sense of identification within the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING LEADERSHIP
organisation thereby persuading individuals to transcend their own self-interest. However,
transformational leadership model has certain form of limitation like dichromatic
interpretation of the leadership while keeping the focus upon the heroic or charismatic leaders
and providing minimal insight into the leader integrity (Hutchinson & Jackson, 2013).
Nevertheless, these limitations can be overcomed via the human-capital-enhancing resource
management style of transformational leaders. This particular style will motivate the
members of the team beyond their own expectations and thereby helping them to inherit and
successfully implement the change in the medication management under nursing care
(Hutchinson & Jackson, 2013).
In contrast to the transformational leadership, transactional leadership model is
based on “exchanges” between the follower and leader under which the follower is rewarded
for satisfying specific performance criteria or goals. Though transactional leadership is more
practical in nature as it give importance towards meeting specific targets or objectives, it has
certain level of limitations (Dumdum, Lowe & Avolio, 2013). Dumdum, Lowe and Avolio
(2013) is of the opinion that transactional leaders are said to achieve performance when
required via contingent rewards or via negative feedbacks. The focus of the transactional
leaders is to focus mainly upon the structures while clarifying the tasks along with providing
valid rewards only for extra efforts or satisfying the requirement of the team members only
when they meet or comply the expectations. This specific pattern of achieving performance
of the followers via contingent reward has been conceptualized as much lower order
leadership function. Thus the transactional leadership model might not be suitable for the
implementation of fresh new change in the nursing practise. Clarke (2013) is of the opinion
that while implementing any advanced technological change in the nursing practise like in the
case of eMARs, it is the duty of a nursing leader to acknowledge each and every initiative
taken by a nursing professional towards effective medication management through eMARs.
organisation thereby persuading individuals to transcend their own self-interest. However,
transformational leadership model has certain form of limitation like dichromatic
interpretation of the leadership while keeping the focus upon the heroic or charismatic leaders
and providing minimal insight into the leader integrity (Hutchinson & Jackson, 2013).
Nevertheless, these limitations can be overcomed via the human-capital-enhancing resource
management style of transformational leaders. This particular style will motivate the
members of the team beyond their own expectations and thereby helping them to inherit and
successfully implement the change in the medication management under nursing care
(Hutchinson & Jackson, 2013).
In contrast to the transformational leadership, transactional leadership model is
based on “exchanges” between the follower and leader under which the follower is rewarded
for satisfying specific performance criteria or goals. Though transactional leadership is more
practical in nature as it give importance towards meeting specific targets or objectives, it has
certain level of limitations (Dumdum, Lowe & Avolio, 2013). Dumdum, Lowe and Avolio
(2013) is of the opinion that transactional leaders are said to achieve performance when
required via contingent rewards or via negative feedbacks. The focus of the transactional
leaders is to focus mainly upon the structures while clarifying the tasks along with providing
valid rewards only for extra efforts or satisfying the requirement of the team members only
when they meet or comply the expectations. This specific pattern of achieving performance
of the followers via contingent reward has been conceptualized as much lower order
leadership function. Thus the transactional leadership model might not be suitable for the
implementation of fresh new change in the nursing practise. Clarke (2013) is of the opinion
that while implementing any advanced technological change in the nursing practise like in the
case of eMARs, it is the duty of a nursing leader to acknowledge each and every initiative
taken by a nursing professional towards effective medication management through eMARs.
5NURSING LEADERSHIP
Rewarding only added efforts will only create a disgust or unwillingness to implement the
change and thereby creating failure towards successful utilization of the eMARs in reducing
medication error and management (Clarke, 2013).
However, Frankel and PGCMS (2018) are of the opinion that a given nursing leader
may exhibit a varying percentage of both the leadership that is transformational or
transactional leadership. These two theories of leadership models or theories are not mutually
exclusive and few combinations of both might increase effective leadership and overall
change management outcomes.
In the concerned organisation (the main organisation of interest in this assignment),
leadership traits are also taken into special considerations apart from abiding by one specific
leadership model. According to Stanley and Stanley (2017), these specific leadership traits
are an important determining factor behind the clinical leadership in nursing professional.
Stanley and Stanley (2017) further argued that clinical leadership in nursing is a special
practise domain that employs interpersonal communication skills in order to support nurses to
procure high quality patient care. According to Gesme and Wiseman (2010), effective and
frequent communication is important during the change implementation at strategic,
operational and at individual level. When promoting a transformative change, Gesme and
Wiseman (2010) argued that effective communication is extremely important in order to
communication few basic question lying behind a particular change and this includes “who”,
“what”, “where”, “why” and “how”. Other level of clinical leadership after communication
that must be displayed in all level of nursing is fostering a team culture. Under this
leadership trait, a nursing leader with manage the change process via encouraging the
participation of the individuals involved in the change. This emphasizes the importance of the
team culture where everyone will be motivated enough to work towards the common goal
(change implementation). Moreover, an efficient nursing clinical leader must also provide
Rewarding only added efforts will only create a disgust or unwillingness to implement the
change and thereby creating failure towards successful utilization of the eMARs in reducing
medication error and management (Clarke, 2013).
However, Frankel and PGCMS (2018) are of the opinion that a given nursing leader
may exhibit a varying percentage of both the leadership that is transformational or
transactional leadership. These two theories of leadership models or theories are not mutually
exclusive and few combinations of both might increase effective leadership and overall
change management outcomes.
In the concerned organisation (the main organisation of interest in this assignment),
leadership traits are also taken into special considerations apart from abiding by one specific
leadership model. According to Stanley and Stanley (2017), these specific leadership traits
are an important determining factor behind the clinical leadership in nursing professional.
Stanley and Stanley (2017) further argued that clinical leadership in nursing is a special
practise domain that employs interpersonal communication skills in order to support nurses to
procure high quality patient care. According to Gesme and Wiseman (2010), effective and
frequent communication is important during the change implementation at strategic,
operational and at individual level. When promoting a transformative change, Gesme and
Wiseman (2010) argued that effective communication is extremely important in order to
communication few basic question lying behind a particular change and this includes “who”,
“what”, “where”, “why” and “how”. Other level of clinical leadership after communication
that must be displayed in all level of nursing is fostering a team culture. Under this
leadership trait, a nursing leader with manage the change process via encouraging the
participation of the individuals involved in the change. This emphasizes the importance of the
team culture where everyone will be motivated enough to work towards the common goal
(change implementation). Moreover, an efficient nursing clinical leader must also provide
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING LEADERSHIP
feedback along with positive reinforcement to the team members in order to motivate them
to work effectively towards the change. According to Gesme and Wiseman (2010),
individuals want to know how are they performing or whether their efforts are making any
difference towards the change. Thus providing periodic feedback to the team members will
help to document the entire process of progression along with the reinforcement of the new
behaviours. Another trait if a nursing leader that must be reflected in order to implement the
change is identification and empowerment of the champions. Gesme and Wiseman (2010)
argued that all changes demand visible champions who are devoted towards the goals and can
lead other members of the team. It is the role of a nursing leader to know the strength of his
or her team members. Here strength signifies to recognise the individuals with natural
leadership skills who will in turn convince the peers towards optimal implementation of the
change.
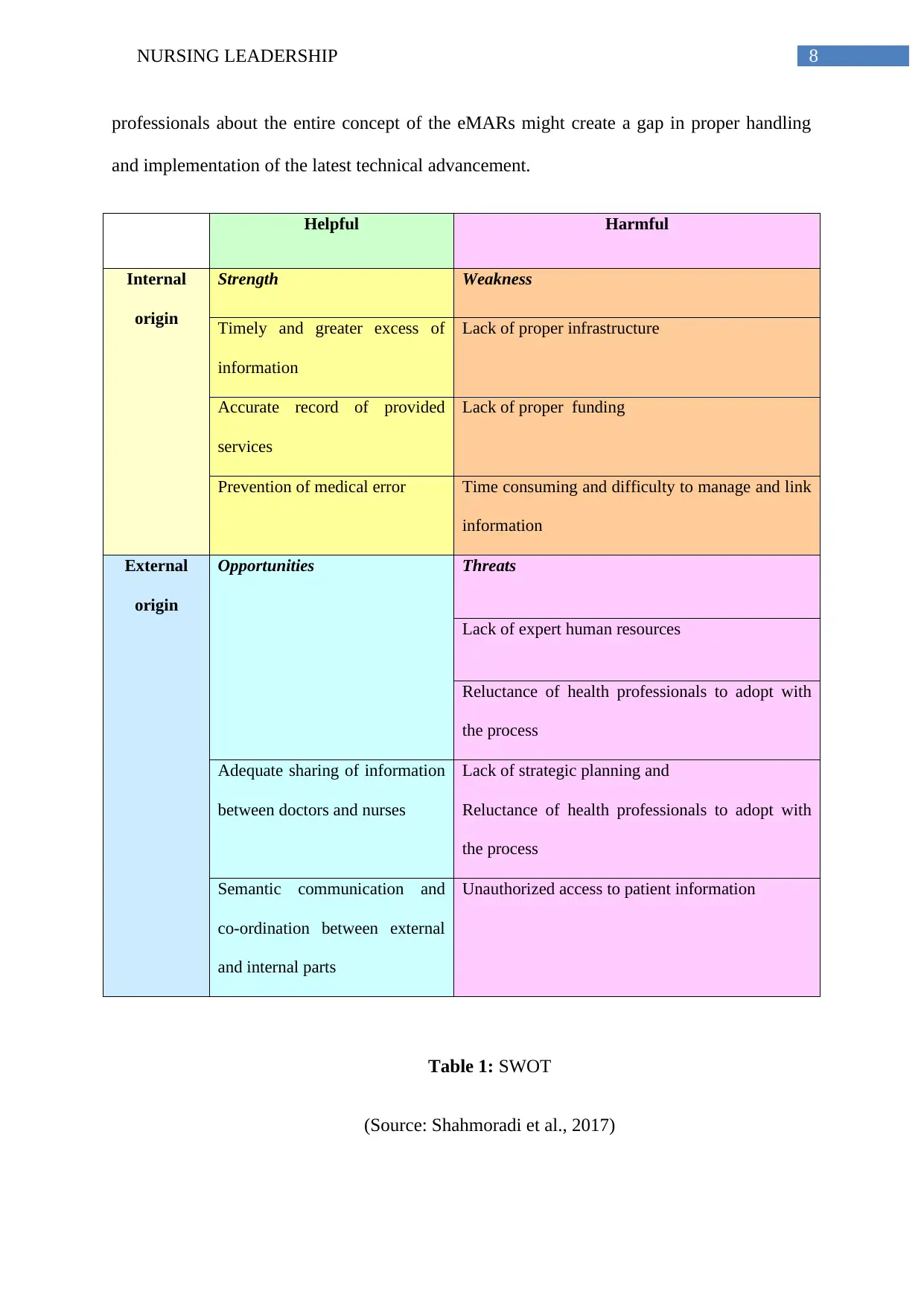
Innovation in healthcare
Effects of working environment on planned change via SWOT analysis
Strength:
The main strength of the eMAR is related to quick and timely access of the
medication related information for the patient by the nurses (Shahmoradi, Darrudi, Arji &
Nejad, 2017). According to Moreland, Gallagher, Bena, Morrison and Albert (2012), the use
of the eMARs enable the nursing professionals to access the medication related information
of the patients whenever and wherever required. This greater access to information will help
to improve patient care and at the same time the concerned nursing professionals will be able
to communicate with each other remotely.
Weakness:
feedback along with positive reinforcement to the team members in order to motivate them
to work effectively towards the change. According to Gesme and Wiseman (2010),
individuals want to know how are they performing or whether their efforts are making any
difference towards the change. Thus providing periodic feedback to the team members will
help to document the entire process of progression along with the reinforcement of the new
behaviours. Another trait if a nursing leader that must be reflected in order to implement the
change is identification and empowerment of the champions. Gesme and Wiseman (2010)
argued that all changes demand visible champions who are devoted towards the goals and can
lead other members of the team. It is the role of a nursing leader to know the strength of his
or her team members. Here strength signifies to recognise the individuals with natural
leadership skills who will in turn convince the peers towards optimal implementation of the
change.
Innovation in healthcare
Effects of working environment on planned change via SWOT analysis
Strength:
The main strength of the eMAR is related to quick and timely access of the
medication related information for the patient by the nurses (Shahmoradi, Darrudi, Arji &
Nejad, 2017). According to Moreland, Gallagher, Bena, Morrison and Albert (2012), the use
of the eMARs enable the nursing professionals to access the medication related information
of the patients whenever and wherever required. This greater access to information will help
to improve patient care and at the same time the concerned nursing professionals will be able
to communicate with each other remotely.
Weakness:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING LEADERSHIP
The main weakness of the implementation of the eMARs is mainly associated with
the lack of proper hardware and compatible infrastructures (Shahmoradi et al., 2017). The
amount of investment required to perchance and simultaneously install eMARs is the main
barrier towards the optimal adaptation of the eMARS. Apart from significant amount of
capital investment, another weakness of implementation of eMARs is high demand of the
information-technology workforce in order to link, store and handle the data encryption
(Staggers, Iribarren, Guo & Weir, 2015).
Opportunity:
The main opportunities behind the implementation of the eMARs under hospital
settings for proper medication management is proper sharing of the information between the
doctors and the nurses and thereby helping to increase the quality of care along with
decreasing the gap of information exchange between both the groups of health care
professionals (Moreland et al., 2012). Moreover it will ensure semantic co-ordination and
communication between the external and internal system along while maintaining integrity
(Shahmoradi et al., 2017).
Threats:
The main threats arising behind the optimal implementation of the eMARs under
hospital settings is the unwillingness of the healthcare professionals to spontaneously adopt
this electronic software. The reluctant is learning the technical specificities required for
handling eMARs may create a disturbance within the entire synchronization of the work-
process. Moreover, lack for proper stringent privacy regulation in the technicalities of the
eMARs have lead to unauthorised access of the patient’s medical information leading to
bridging of the ethical issue of privacy and confidentiality (Middleton et al., 2013).
According to Shahmoradi et al. (2017), the limited awareness among the healthcare
The main weakness of the implementation of the eMARs is mainly associated with
the lack of proper hardware and compatible infrastructures (Shahmoradi et al., 2017). The
amount of investment required to perchance and simultaneously install eMARs is the main
barrier towards the optimal adaptation of the eMARS. Apart from significant amount of
capital investment, another weakness of implementation of eMARs is high demand of the
information-technology workforce in order to link, store and handle the data encryption
(Staggers, Iribarren, Guo & Weir, 2015).
Opportunity:
The main opportunities behind the implementation of the eMARs under hospital
settings for proper medication management is proper sharing of the information between the
doctors and the nurses and thereby helping to increase the quality of care along with
decreasing the gap of information exchange between both the groups of health care
professionals (Moreland et al., 2012). Moreover it will ensure semantic co-ordination and
communication between the external and internal system along while maintaining integrity
(Shahmoradi et al., 2017).
Threats:
The main threats arising behind the optimal implementation of the eMARs under
hospital settings is the unwillingness of the healthcare professionals to spontaneously adopt
this electronic software. The reluctant is learning the technical specificities required for
handling eMARs may create a disturbance within the entire synchronization of the work-
process. Moreover, lack for proper stringent privacy regulation in the technicalities of the
eMARs have lead to unauthorised access of the patient’s medical information leading to
bridging of the ethical issue of privacy and confidentiality (Middleton et al., 2013).
According to Shahmoradi et al. (2017), the limited awareness among the healthcare
8NURSING LEADERSHIP
professionals about the entire concept of the eMARs might create a gap in proper handling
and implementation of the latest technical advancement.
Helpful Harmful
Internal
origin
Strength Weakness
Timely and greater excess of
information
Lack of proper infrastructure
Accurate record of provided
services
Lack of proper funding
Prevention of medical error Time consuming and difficulty to manage and link
information
External
origin
Opportunities Threats
Lack of expert human resources
Reluctance of health professionals to adopt with
the process
Adequate sharing of information
between doctors and nurses
Lack of strategic planning and
Reluctance of health professionals to adopt with
the process
Semantic communication and
co-ordination between external
and internal parts
Unauthorized access to patient information
Table 1: SWOT
(Source: Shahmoradi et al., 2017)
professionals about the entire concept of the eMARs might create a gap in proper handling
and implementation of the latest technical advancement.
Helpful Harmful
Internal
origin
Strength Weakness
Timely and greater excess of
information
Lack of proper infrastructure
Accurate record of provided
services
Lack of proper funding
Prevention of medical error Time consuming and difficulty to manage and link
information
External
origin
Opportunities Threats
Lack of expert human resources
Reluctance of health professionals to adopt with
the process
Adequate sharing of information
between doctors and nurses
Lack of strategic planning and
Reluctance of health professionals to adopt with
the process
Semantic communication and
co-ordination between external
and internal parts
Unauthorized access to patient information
Table 1: SWOT
(Source: Shahmoradi et al., 2017)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING LEADERSHIP
Change and change management
According to Al-Balushi et al. (2014), change management is defined as an
application of a set of tools, skills, processes and principles for effective management of
people side of change in order to obtain the needed outcomes of a change initiative or project.
Al-Balushi et al. (2014) is of the opinion that change in healthcare is progressing with a rapid
phase as the practises strive to implement new regulator and policy guidelines. Under this
environment of change the implementation of eMARs is extremely a path-breaking steps as
this change is taking place under some circumstances where healthcare providers are still
attending patients and at the same time trying to maintain a healthy work life-balance. For
obvious reasons these are stressful times for the healthcare providers and adapting to change
has become a part of their professional life. Fortunately, change management is well-
developed domain with prominent evidence and evidence and adequate learning practices on
how to successfully manage the overall change process. One of the leading notable tinkers in
managing organisational change and delivering applicable strategies for navigating change is
John Kotter (Hornstein, 2015). According to Kotter, change has both situational and
emotional components for proper optimal implementation of change Kotter has proposed a
multi-step change model. This model is arranged in three main phases in order to assist the
leaders to effectively manage the challenges that are inherent under any initiative of change
(Hornstein, 2015). Another change management model is Lewin’s change management
model. Lewin’s change management model is based in three stages of change management
and this includes unfreezing, change or transition and re-freezing (Shirey, 2013).
Change and change management
According to Al-Balushi et al. (2014), change management is defined as an
application of a set of tools, skills, processes and principles for effective management of
people side of change in order to obtain the needed outcomes of a change initiative or project.
Al-Balushi et al. (2014) is of the opinion that change in healthcare is progressing with a rapid
phase as the practises strive to implement new regulator and policy guidelines. Under this
environment of change the implementation of eMARs is extremely a path-breaking steps as
this change is taking place under some circumstances where healthcare providers are still
attending patients and at the same time trying to maintain a healthy work life-balance. For
obvious reasons these are stressful times for the healthcare providers and adapting to change
has become a part of their professional life. Fortunately, change management is well-
developed domain with prominent evidence and evidence and adequate learning practices on
how to successfully manage the overall change process. One of the leading notable tinkers in
managing organisational change and delivering applicable strategies for navigating change is
John Kotter (Hornstein, 2015). According to Kotter, change has both situational and
emotional components for proper optimal implementation of change Kotter has proposed a
multi-step change model. This model is arranged in three main phases in order to assist the
leaders to effectively manage the challenges that are inherent under any initiative of change
(Hornstein, 2015). Another change management model is Lewin’s change management
model. Lewin’s change management model is based in three stages of change management
and this includes unfreezing, change or transition and re-freezing (Shirey, 2013).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10NURSING LEADERSHIP
Lewin’s change management model
(Source: Shirey, 2013)
For the optimal implementation of the eMARs, Kotter’s change management model
will be extremely effective. The below mentioned diagram attempts to illustrates how
Kotter’s three-phase approach can be employed while planning a change from the present
way of executing business and caring for patients with a vision of future practise that
optimizes the application of technology to deliver high-quality, safe and effective patient care
services while adequately satisfying the regulatory requirements (Boonstra, Versluis & Vos,
2014).
UnfreezeDeterminationofwhatneedstobechangedCreatinganeedforchangeunderthestrongsupportfrommanagementUnderstandingandmanagingthedoubtsofconcersChangePropercommunicationEmpoweringactionsInvolvingtheconcernedpeopleintotheoverallprocessRefreezeAnchoringthechangingwithintheadministrativesysteoftheprganisationandworkcultureProvidingpropersupportfortrainingDevelopingwaystosustainthechanges
Lewin’s change management model
(Source: Shirey, 2013)
For the optimal implementation of the eMARs, Kotter’s change management model
will be extremely effective. The below mentioned diagram attempts to illustrates how
Kotter’s three-phase approach can be employed while planning a change from the present
way of executing business and caring for patients with a vision of future practise that
optimizes the application of technology to deliver high-quality, safe and effective patient care
services while adequately satisfying the regulatory requirements (Boonstra, Versluis & Vos,
2014).
UnfreezeDeterminationofwhatneedstobechangedCreatinganeedforchangeunderthestrongsupportfrommanagementUnderstandingandmanagingthedoubtsofconcersChangePropercommunicationEmpoweringactionsInvolvingtheconcernedpeopleintotheoverallprocessRefreezeAnchoringthechangingwithintheadministrativesysteoftheprganisationandworkcultureProvidingpropersupportfortrainingDevelopingwaystosustainthechanges
11NURSING LEADERSHIP
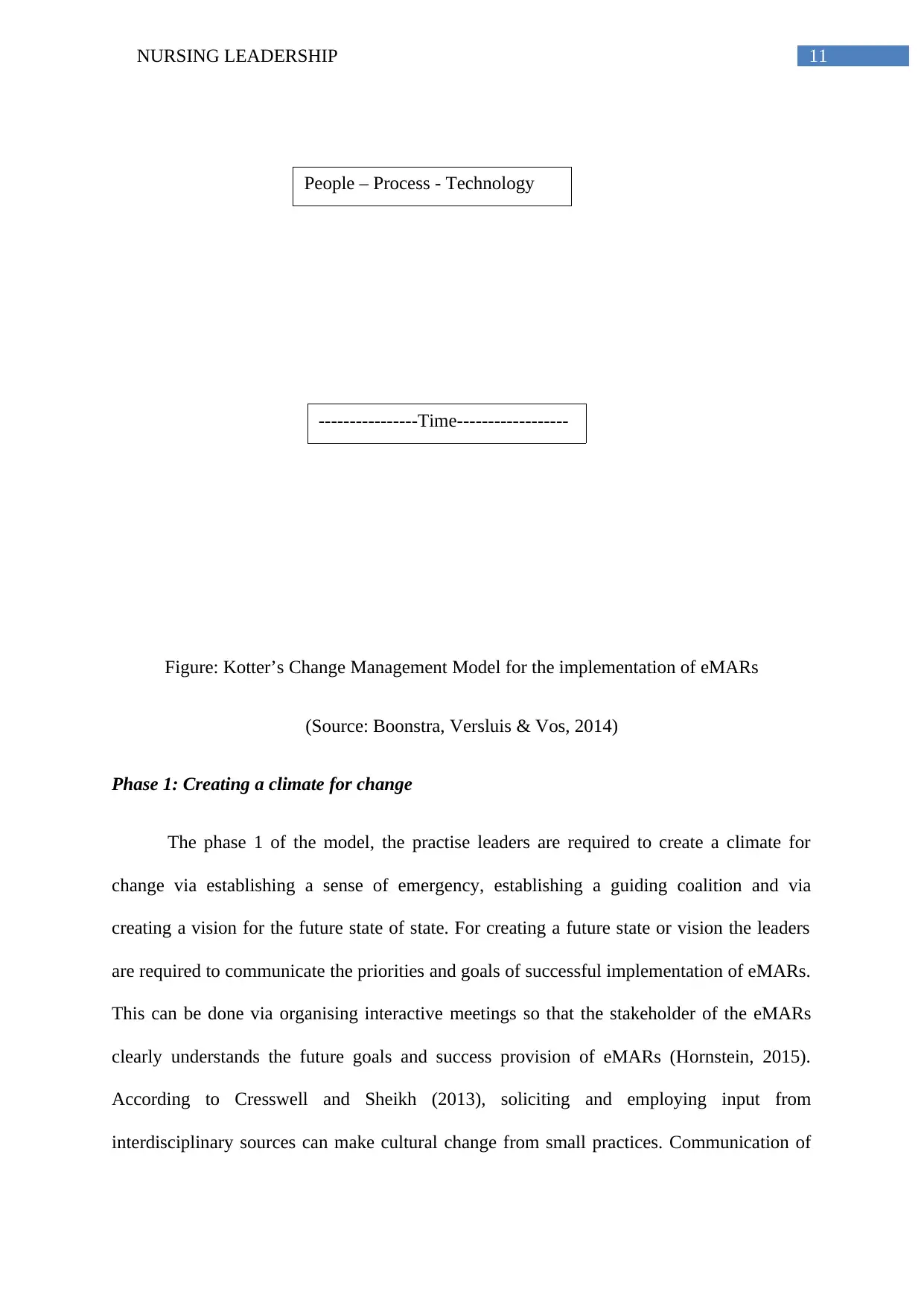
Figure: Kotter’s Change Management Model for the implementation of eMARs
(Source: Boonstra, Versluis & Vos, 2014)
Phase 1: Creating a climate for change
The phase 1 of the model, the practise leaders are required to create a climate for
change via establishing a sense of emergency, establishing a guiding coalition and via
creating a vision for the future state of state. For creating a future state or vision the leaders
are required to communicate the priorities and goals of successful implementation of eMARs.
This can be done via organising interactive meetings so that the stakeholder of the eMARs
clearly understands the future goals and success provision of eMARs (Hornstein, 2015).
According to Cresswell and Sheikh (2013), soliciting and employing input from
interdisciplinary sources can make cultural change from small practices. Communication of
CurrentstatePhase1CreatingaclimateforchangePhase2EnagagingandenablingtheorganisationforthechangePhase3ImplementingandsustainingchangesFuturestateSuccessfullimplementationofeMARs----------------Time------------------
People – Process - Technology
Figure: Kotter’s Change Management Model for the implementation of eMARs
(Source: Boonstra, Versluis & Vos, 2014)
Phase 1: Creating a climate for change
The phase 1 of the model, the practise leaders are required to create a climate for
change via establishing a sense of emergency, establishing a guiding coalition and via
creating a vision for the future state of state. For creating a future state or vision the leaders
are required to communicate the priorities and goals of successful implementation of eMARs.
This can be done via organising interactive meetings so that the stakeholder of the eMARs
clearly understands the future goals and success provision of eMARs (Hornstein, 2015).
According to Cresswell and Sheikh (2013), soliciting and employing input from
interdisciplinary sources can make cultural change from small practices. Communication of
CurrentstatePhase1CreatingaclimateforchangePhase2EnagagingandenablingtheorganisationforthechangePhase3ImplementingandsustainingchangesFuturestateSuccessfullimplementationofeMARs----------------Time------------------
People – Process - Technology
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 22
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.