Case Study: Diagnosis, Treatment, and Nursing of Left Heart Failure
VerifiedAdded on 2020/03/04
|11
|2228
|62
Case Study
AI Summary
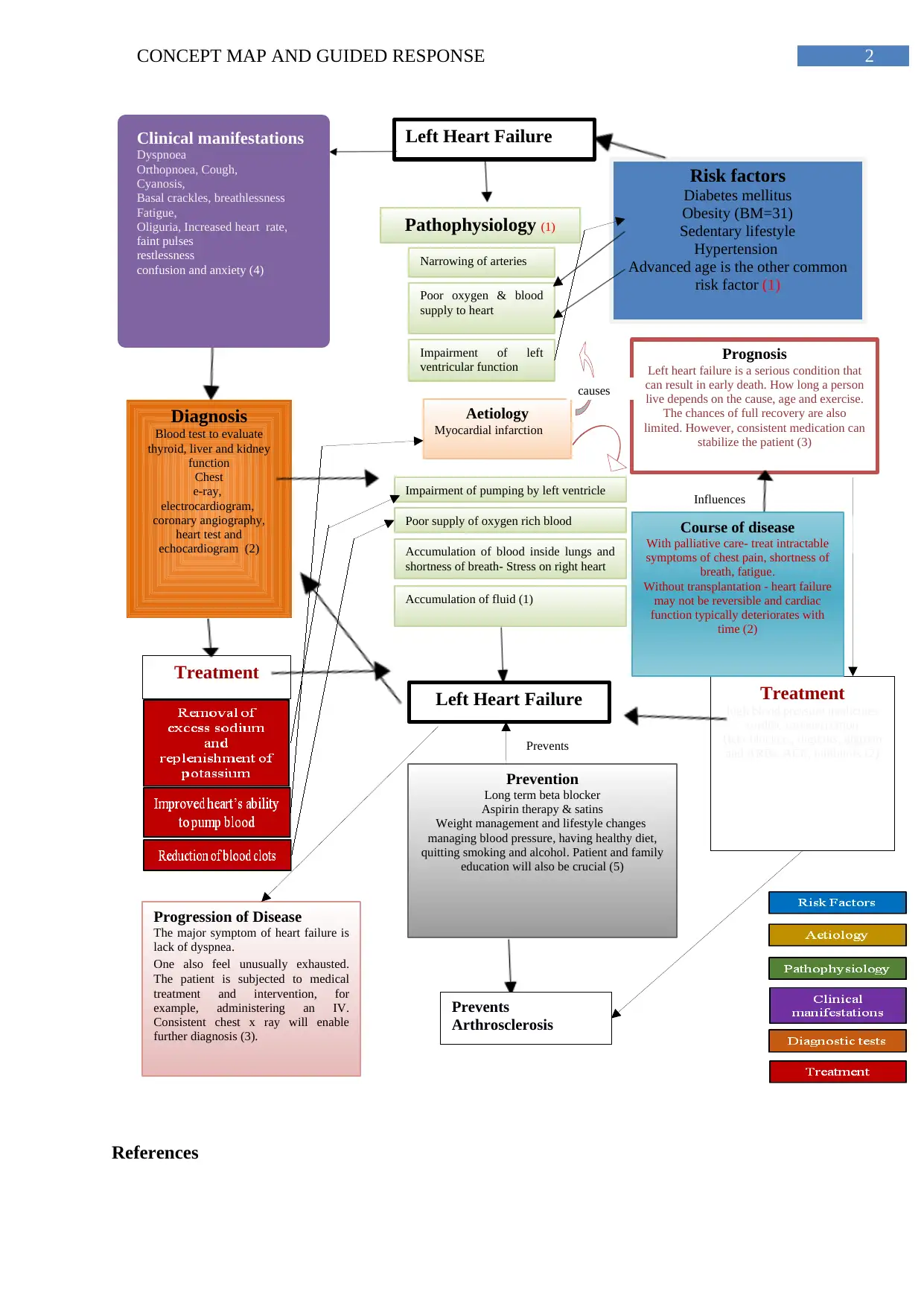
This assignment presents a comprehensive case study on chronic left-sided heart failure, focusing on a patient named Mrs. Brown. It begins with a concept map illustrating the risk factors, etiology, pathophysiology, clinical manifestations, diagnosis, treatment, and prognosis of the condition. The case study then delves into the patient's clinical presentation, including tachycardia, tachypnea, dyspnea, and decreased oxygen saturation, leading to a diagnosis of chronic left-sided heart failure with arterial fibrillation. The pathogenesis of the condition is discussed, emphasizing systolic and diastolic dysfunction. Furthermore, the assignment explores evidence-based nursing strategies for managing Mrs. Brown's condition, including oxygen therapy and medication administration, such as Digoxine. Finally, it examines the mechanism of action and nursing implications of IV furosemide and sublingual glyceryl trinitrate, commonly used medications in treating heart failure, providing valuable insights into patient care and pharmacological interventions.



1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.