Lifespan Nutrition Assessment: Case Study and Dietary Analysis
VerifiedAdded on 2023/04/22
|29
|7557
|165
Case Study
AI Summary
This assignment presents a detailed analysis of Lifespan Nutrition through case studies and personal dietary assessment. The first section examines the nutritional needs and health risks associated with overweight individuals planning for conception, including recommendations for folate and iron supplementation, and dietary and exercise guidelines. The second case study focuses on an adolescent, analyzing her dietary imbalances and providing a sample meal plan to address nutritional deficiencies. The assignment also includes a BMR calculation and a personal dietary analysis, evaluating the author's own food intake against recommended values and identifying deficiencies in protein, iron, calcium, and vitamins, along with suggestions for dietary modifications. The final sections delve into the impact of nutritional restriction before gestation and the factors influencing fetal growth, including discussions of IUGR and its effects on childhood development.

Running head : LIFESPAN NUTRITION
LIFESPAN NUTRITION
Name of the Student:
Name of the University:
Author note:
LIFESPAN NUTRITION
Name of the Student:
Name of the University:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1LIFESPAN NUTRITION
Case Study 2
Question 1: As observed from the given case study, the Body Mass Index (BMI) as well as the
waist circumference of both Jack and Jill are within the categories of ‘overweight’. In
accordance to the Department of Health of the Australian Government as well as ‘IVF Australia’
– a leading organization of fertility and reproductive health in Australia, the maintenance of a
BMI within the ‘normal’ range of 18.5 – 24.9, in adults aged 19 to 30 years, exerts optimal
health outcomes concerning an individual’s reproductive and sexual health as well as
possibilities of a healthy conception (Australian Government Department of Health, 2019). This
is due the fact that an abnormally high weight is associated with imbalances in hormones
responsible for ovulation resulting in disturbed menstrual and ovulation cycles (Kudesia, Talib &
Pollack, 2017). Even amidst a situation of successfully conception and pregnancy, an unhealthy
BMI poses increased susceptibilities to hypertension, preeclampsia, blood clotting, gestational
diabetes, still birth and babies with congenital and anthropometric measurements (Waring et al.,
2015). Likewise, excessive body weight in males can exert detrimental effects in the quality and
fertility of sperms, hence affecting conception (Kothari et al., 2019). Thus, considering the above
recommendations, Jack and Jill’s reproductive health as per their age and anthropometric
measurements is inappropriate and unhealthy for successful conception.
Question 2: While achievement of gradual reductions in weight resulting in healthy weight can
yield beneficial effects on a couple’s possibility to conceive, rapid losses in weight must be
address with precautions since it may result in complication during birth and as well as in the
offspring (Gorczyca et al., 2018).A rapid loss in weight can result in the birth of a child who is
preterm, is of low birth weight and stunted in growth and development (Price et al., 2018).
Case Study 2
Question 1: As observed from the given case study, the Body Mass Index (BMI) as well as the
waist circumference of both Jack and Jill are within the categories of ‘overweight’. In
accordance to the Department of Health of the Australian Government as well as ‘IVF Australia’
– a leading organization of fertility and reproductive health in Australia, the maintenance of a
BMI within the ‘normal’ range of 18.5 – 24.9, in adults aged 19 to 30 years, exerts optimal
health outcomes concerning an individual’s reproductive and sexual health as well as
possibilities of a healthy conception (Australian Government Department of Health, 2019). This
is due the fact that an abnormally high weight is associated with imbalances in hormones
responsible for ovulation resulting in disturbed menstrual and ovulation cycles (Kudesia, Talib &
Pollack, 2017). Even amidst a situation of successfully conception and pregnancy, an unhealthy
BMI poses increased susceptibilities to hypertension, preeclampsia, blood clotting, gestational
diabetes, still birth and babies with congenital and anthropometric measurements (Waring et al.,
2015). Likewise, excessive body weight in males can exert detrimental effects in the quality and
fertility of sperms, hence affecting conception (Kothari et al., 2019). Thus, considering the above
recommendations, Jack and Jill’s reproductive health as per their age and anthropometric
measurements is inappropriate and unhealthy for successful conception.
Question 2: While achievement of gradual reductions in weight resulting in healthy weight can
yield beneficial effects on a couple’s possibility to conceive, rapid losses in weight must be
address with precautions since it may result in complication during birth and as well as in the
offspring (Gorczyca et al., 2018).A rapid loss in weight can result in the birth of a child who is
preterm, is of low birth weight and stunted in growth and development (Price et al., 2018).
2LIFESPAN NUTRITION
Further, rapid weight loss prior to conception may result in low maternal weight and nutritional
deficiencies of key micronutrients such as iron and folate, which will not only enhance chances
of miscarriage, but may also result in delivery of a baby with deformities such as neural tube
defects (Schummers et al., 2015).
Question 3: In accordance to the Nutrient and Reference Values for Australia and New Zealand,
the Recommended Dietary Intake (RDI) and the Estimated Average Requirement (EAR) of
folate is 600 μg/day and 520 μg/day, while that of iron is 27 mg/day and 22-23 mg/day during
pregnancy (National Health and Medical Research Council. (2019). This will aid in the
achievement of a healthy conception, maintenance of healthy maternal as well as fetal blood
volumes, as well as the birth of a baby which is free from anemia, neural tube defects and
nutritional stunting (Moll & Davis, 2017). Hence, considering the difficulty of meeting these
nutritional needs through diet alone, Jill may be required to consume folate and iron nutritional
supplements as recommended by The Royal Australian and New Zealand College of
Obstetricians and Gynecologists at daily dosages of 60 mg (iron) and 0.4 mg (folate) for healthy
conception and delivery (The Royal Australian and New Zealand College of Obstetricians and
Gynaecologists, 2019). Likewise, as per the Australian Dietary Guidelines, Jack and Jill can
adhere to moderate levels of exercise daily for 30 minutes (as per less than 4.5 hours per day
times for sitting) and 45 to 60 minutes (as per sedentary lifestyle and contemporary fast food
consumption) for healthy loss. Similarly, as per the guidelines, Jack and Jill can also adhere to
Foundation Diets formulated by the Food Modeling system, which is high in whole grains, milk
products and lean meats and low in refined grains, starches and high fat products like red meats
and whole milk dairy foods, for weight loss and healthy conception (Australian Dietary
Guidelines, 2019).
Further, rapid weight loss prior to conception may result in low maternal weight and nutritional
deficiencies of key micronutrients such as iron and folate, which will not only enhance chances
of miscarriage, but may also result in delivery of a baby with deformities such as neural tube
defects (Schummers et al., 2015).
Question 3: In accordance to the Nutrient and Reference Values for Australia and New Zealand,
the Recommended Dietary Intake (RDI) and the Estimated Average Requirement (EAR) of
folate is 600 μg/day and 520 μg/day, while that of iron is 27 mg/day and 22-23 mg/day during
pregnancy (National Health and Medical Research Council. (2019). This will aid in the
achievement of a healthy conception, maintenance of healthy maternal as well as fetal blood
volumes, as well as the birth of a baby which is free from anemia, neural tube defects and
nutritional stunting (Moll & Davis, 2017). Hence, considering the difficulty of meeting these
nutritional needs through diet alone, Jill may be required to consume folate and iron nutritional
supplements as recommended by The Royal Australian and New Zealand College of
Obstetricians and Gynecologists at daily dosages of 60 mg (iron) and 0.4 mg (folate) for healthy
conception and delivery (The Royal Australian and New Zealand College of Obstetricians and
Gynaecologists, 2019). Likewise, as per the Australian Dietary Guidelines, Jack and Jill can
adhere to moderate levels of exercise daily for 30 minutes (as per less than 4.5 hours per day
times for sitting) and 45 to 60 minutes (as per sedentary lifestyle and contemporary fast food
consumption) for healthy loss. Similarly, as per the guidelines, Jack and Jill can also adhere to
Foundation Diets formulated by the Food Modeling system, which is high in whole grains, milk
products and lean meats and low in refined grains, starches and high fat products like red meats
and whole milk dairy foods, for weight loss and healthy conception (Australian Dietary
Guidelines, 2019).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3LIFESPAN NUTRITION
Case Study 5
Question 1: As per the given data, it can be calculated that Kara’s BMI is 26.6, which according
to the growth rate and BMI for age z scores outlined by the World Health Organization is in the
category of ‘overweight’ (World Health Organization, 2019).
Question 2: Upon evaluation of Kara’s diet, it can be observed that are daily food consumption
comprises of a large portion of processed foods such as breakfast cereals, biscuits, chips and nuts
as well as sugars, coupled with comparatively lower portions of vegetables and proteins. Hence,
this means that Kara’s current diet comprises of major nutritional imbalances in terms of high
amounts of refined and sugary carbohydrates due to processed food consumption and low
quantities of macronutrients such as proteins and unsaturated fats, due to inappropriate
consumption of lean meats, legumes and dairy products (Carrasco-Luna et al., 2018). Likewise,
due to inadequate consumption of vegetables and fruits, imbalances also exist in terms of
deficiencies in micronutrients such as vitamins, minerals and antioxidants (Joo, Ju & Chang,
2015). As per the Australian Guide to Healthy Eating, Kara’s diet must comprise of a balanced
proportion of core food groups such as whole grains, lean meats, dairy products, fruits,
vegetables, legumes and beans for the prevention of nutritional imbalances (Australian Dietary
Guidelines, 2019).
Question 3: As per the data reported by the Australian Bureau of Statistics – Australian Health
Survey (2011 – 2012) – Australians, especially adolescents within the age group of 14 to 18
years, derive a major proportion of their energy from ‘discretionary foods’ – which include
products of negligible nutritional value such as sugary sweetened beverages, breakfast cereals
and confectionary items such as fruit and nut bars which increases susceptibilities to deficiencies
in macronutrients like dietary fiber and excess consumption of saturated fats, sugars and the
Case Study 5
Question 1: As per the given data, it can be calculated that Kara’s BMI is 26.6, which according
to the growth rate and BMI for age z scores outlined by the World Health Organization is in the
category of ‘overweight’ (World Health Organization, 2019).
Question 2: Upon evaluation of Kara’s diet, it can be observed that are daily food consumption
comprises of a large portion of processed foods such as breakfast cereals, biscuits, chips and nuts
as well as sugars, coupled with comparatively lower portions of vegetables and proteins. Hence,
this means that Kara’s current diet comprises of major nutritional imbalances in terms of high
amounts of refined and sugary carbohydrates due to processed food consumption and low
quantities of macronutrients such as proteins and unsaturated fats, due to inappropriate
consumption of lean meats, legumes and dairy products (Carrasco-Luna et al., 2018). Likewise,
due to inadequate consumption of vegetables and fruits, imbalances also exist in terms of
deficiencies in micronutrients such as vitamins, minerals and antioxidants (Joo, Ju & Chang,
2015). As per the Australian Guide to Healthy Eating, Kara’s diet must comprise of a balanced
proportion of core food groups such as whole grains, lean meats, dairy products, fruits,
vegetables, legumes and beans for the prevention of nutritional imbalances (Australian Dietary
Guidelines, 2019).
Question 3: As per the data reported by the Australian Bureau of Statistics – Australian Health
Survey (2011 – 2012) – Australians, especially adolescents within the age group of 14 to 18
years, derive a major proportion of their energy from ‘discretionary foods’ – which include
products of negligible nutritional value such as sugary sweetened beverages, breakfast cereals
and confectionary items such as fruit and nut bars which increases susceptibilities to deficiencies
in macronutrients like dietary fiber and excess consumption of saturated fats, sugars and the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4LIFESPAN NUTRITION
resultant calories (Australian Bureau of Statistics (2019). Likewise, adolescence is a stage of
growth spurts associated with increased muscle development, blood volumes and bone mass
(Cox et al., 2017). Considering the observed Australian Health Survey’s reports of low fruit and
vegetable intake by adolescents, which is also observed in Kara, such imbalances can result in
increased risk of deficiencies in macronutrients such as proteins and micronutrients such as
calcium and iron (Lobstein et al., 2015). The risk of iron is greater in female adolescents like
Kara due to her regular menstrual cycles (Atkins et al., 2019).
Question 4: Diet plan for Kara (as designed by the Author)
Meal Menu
Breakfast Strawberry and blueberry oats porridge
prepared in low fat milk (1 bowl)
1 boiled egg
Mid-Morning Baked kale and sweet potato chips (1
small bowl)
200 ml of apple-cinnamon yogurt
smoothie
Lunch Chicken coleslaw whole grain
sandwich
200 ml low fat chocolate soy milk
Afternoon Tea 30 grams of trail mix (unsalted and
roasted almonds and walnuts)
2 flaxseed and soy crackers with cream
cheese or peanut butter or chickpea and
resultant calories (Australian Bureau of Statistics (2019). Likewise, adolescence is a stage of
growth spurts associated with increased muscle development, blood volumes and bone mass
(Cox et al., 2017). Considering the observed Australian Health Survey’s reports of low fruit and
vegetable intake by adolescents, which is also observed in Kara, such imbalances can result in
increased risk of deficiencies in macronutrients such as proteins and micronutrients such as
calcium and iron (Lobstein et al., 2015). The risk of iron is greater in female adolescents like
Kara due to her regular menstrual cycles (Atkins et al., 2019).
Question 4: Diet plan for Kara (as designed by the Author)
Meal Menu
Breakfast Strawberry and blueberry oats porridge
prepared in low fat milk (1 bowl)
1 boiled egg
Mid-Morning Baked kale and sweet potato chips (1
small bowl)
200 ml of apple-cinnamon yogurt
smoothie
Lunch Chicken coleslaw whole grain
sandwich
200 ml low fat chocolate soy milk
Afternoon Tea 30 grams of trail mix (unsalted and
roasted almonds and walnuts)
2 flaxseed and soy crackers with cream
cheese or peanut butter or chickpea and
5LIFESPAN NUTRITION
bean whole grain toast with hummus
200 ml lime and mint home-made
lemonade
Dinner Snack Chicken and spinach aglio olio pasta topped
with feta cheese
Snack 2 scoops of sugar free, non dairy banana ice cream
or dark 4 dark chocolate coated strawberries
Module 1
Question 3: BMR Calculation
Weight: 55 kg
Height: 160 cm
(For female, in the age group of 18 to 30 years) Basal Metabolic Rate as per the Schofield
equation = 62 * 55 + 2036 = 5446 kJ/day
Questions 1 and 2: Nutritional Analysis (See Appendix 1 and 2)
As per the Nutrient Reference Values for Australia and New Zealand, the recommended
water intake for adults ranges from 8 to 10 cups per day (2.1 – 2.6 liters per day) (National
Health and Medical Research Council, 2019). Upon evaluation of the personal fluid intake for
one day, it can be observed that I am meeting with the required water consumption throughout
the day. However, care has to be taken for not exceeding the given intake since it may result in
health complication such as hyponatremia, cramps, vomiting, nausea and fluctuations in blood
bean whole grain toast with hummus
200 ml lime and mint home-made
lemonade
Dinner Snack Chicken and spinach aglio olio pasta topped
with feta cheese
Snack 2 scoops of sugar free, non dairy banana ice cream
or dark 4 dark chocolate coated strawberries
Module 1
Question 3: BMR Calculation
Weight: 55 kg
Height: 160 cm
(For female, in the age group of 18 to 30 years) Basal Metabolic Rate as per the Schofield
equation = 62 * 55 + 2036 = 5446 kJ/day
Questions 1 and 2: Nutritional Analysis (See Appendix 1 and 2)
As per the Nutrient Reference Values for Australia and New Zealand, the recommended
water intake for adults ranges from 8 to 10 cups per day (2.1 – 2.6 liters per day) (National
Health and Medical Research Council, 2019). Upon evaluation of the personal fluid intake for
one day, it can be observed that I am meeting with the required water consumption throughout
the day. However, care has to be taken for not exceeding the given intake since it may result in
health complication such as hyponatremia, cramps, vomiting, nausea and fluctuations in blood
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6LIFESPAN NUTRITION
pressure (Stachenfield et al., 2018). Upon nutritionally analyzing my food intake by using Food
Choices and comparison with the Nutrient Reference Values, it can be observed that I am
achieving a negative energy balance of 140 kJ per day, which if left uncorrected, can lead to a
state of catabolism, muscle wastage, muscle loss, fatigue and detrimental immune system
(Moberg et al., 2017). However, my protein intake is 33% higher than the EAR which may lead
to acidosis and renal disorders in the future if left uncorrected (Wu, 2016). Further my diet is
also deficient in adequate quantities of iron and calcium. If left uncorrected, iron deficiencies can
lead to anemia, fatigue, numbness and tingling sensations in the hands and feet (Lopez et al.,
2016). Likewise, calcium deficiencies can lead to loss of bone strength and density and hence,
lead to osteoporosis and increased risk of fractures (Kumssa et al., 2015). Gross deficiencies
were also observed in Vitamin C which can result in losses in immune function and delayed
wound healing (Carr et al., 2017). Deficiencies have also been observed in Vitamin A which not
exerts deficits in visual prowess in the future but also increases levels of oxidative stress in
individuals due to its precursors (carotenoids) possessing antioxidant properties (Darlow et al.,
2016). Hence, to correct such deficiencies, I must modify my diet and incorporate increased
quantities of whole grains, green leafy and colorful fruits and vegetables along with
incorporation of low fat sources of dairy product, as per the Australian Dietary Guidelines
(Australian Dietary Guidelines, 2019).
Module 2
Question 1: Nutritional restriction during the ten weeks prior to gestation is likely to exert
detrimental impacts on the growth and development of the baby, despite being a stage of minor
nutritional requirements. This due to the fact that maternal nutrition at this stage is characterized
pressure (Stachenfield et al., 2018). Upon nutritionally analyzing my food intake by using Food
Choices and comparison with the Nutrient Reference Values, it can be observed that I am
achieving a negative energy balance of 140 kJ per day, which if left uncorrected, can lead to a
state of catabolism, muscle wastage, muscle loss, fatigue and detrimental immune system
(Moberg et al., 2017). However, my protein intake is 33% higher than the EAR which may lead
to acidosis and renal disorders in the future if left uncorrected (Wu, 2016). Further my diet is
also deficient in adequate quantities of iron and calcium. If left uncorrected, iron deficiencies can
lead to anemia, fatigue, numbness and tingling sensations in the hands and feet (Lopez et al.,
2016). Likewise, calcium deficiencies can lead to loss of bone strength and density and hence,
lead to osteoporosis and increased risk of fractures (Kumssa et al., 2015). Gross deficiencies
were also observed in Vitamin C which can result in losses in immune function and delayed
wound healing (Carr et al., 2017). Deficiencies have also been observed in Vitamin A which not
exerts deficits in visual prowess in the future but also increases levels of oxidative stress in
individuals due to its precursors (carotenoids) possessing antioxidant properties (Darlow et al.,
2016). Hence, to correct such deficiencies, I must modify my diet and incorporate increased
quantities of whole grains, green leafy and colorful fruits and vegetables along with
incorporation of low fat sources of dairy product, as per the Australian Dietary Guidelines
(Australian Dietary Guidelines, 2019).
Module 2
Question 1: Nutritional restriction during the ten weeks prior to gestation is likely to exert
detrimental impacts on the growth and development of the baby, despite being a stage of minor
nutritional requirements. This due to the fact that maternal nutrition at this stage is characterized
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7LIFESPAN NUTRITION
by its involvement in the development of the placenta. Restriction in nutrients at this stage results
in deficiencies of amino acids - key nutrients responsible for the development of the placental
tissues (Levine et al., 2015). Optimum development of the placenta is essential for the
distribution of nutrients from the mother to the baby and hence, nutritional deficiencies during
the early weeks prior to gestation results in inadequate placental development further leading to
intra-uterine growth restriction (IUGR) (Chassen et al., 2018). IUGR results in adverse effects on
the growth and development of the infant since it leads to restricted and inadequate growth of the
baby inside the womb, further resulting in low birth weight, difficulties during delivery and
reduced oxygen and immune status of the baby (Sharma, Shastri & Shamra, 2016).
Question 2: Maternal and placental factors are the underlying causative factors which determine
the growth of the fetus at greater rates in utero in comparison to other stages in the post natal
period. Some of the major maternal factors which pose as determinants include the body mass
index of the mother, along with her nutritional status, exposure to pollutants and adherence to
lifestyle habits such as smoking and alcohol consumption. This is due to the fact that maternal
nutrition, anthropometrics and lifestyle habits are key determinants of placental growth and
development, an essential component contributing extensively to fetal growth and development
(Cohen et al., 2016). For this reason, placental factors such as tissue size, circulation, protein
binding and nutrient transportation are key factors influencing fetal growth in utero, since these
determine the relaying of maternal nutrient factors to the fetal tissues for growth and
development. Hence, due to the interplay of maternal-fetal placental connections, maternal and
placental factors determine the rapid rate of infant growth in utero as compared to any other
stage (Sharma et al., 2016).
Question 3: Findings of IUGR infants on:
by its involvement in the development of the placenta. Restriction in nutrients at this stage results
in deficiencies of amino acids - key nutrients responsible for the development of the placental
tissues (Levine et al., 2015). Optimum development of the placenta is essential for the
distribution of nutrients from the mother to the baby and hence, nutritional deficiencies during
the early weeks prior to gestation results in inadequate placental development further leading to
intra-uterine growth restriction (IUGR) (Chassen et al., 2018). IUGR results in adverse effects on
the growth and development of the infant since it leads to restricted and inadequate growth of the
baby inside the womb, further resulting in low birth weight, difficulties during delivery and
reduced oxygen and immune status of the baby (Sharma, Shastri & Shamra, 2016).
Question 2: Maternal and placental factors are the underlying causative factors which determine
the growth of the fetus at greater rates in utero in comparison to other stages in the post natal
period. Some of the major maternal factors which pose as determinants include the body mass
index of the mother, along with her nutritional status, exposure to pollutants and adherence to
lifestyle habits such as smoking and alcohol consumption. This is due to the fact that maternal
nutrition, anthropometrics and lifestyle habits are key determinants of placental growth and
development, an essential component contributing extensively to fetal growth and development
(Cohen et al., 2016). For this reason, placental factors such as tissue size, circulation, protein
binding and nutrient transportation are key factors influencing fetal growth in utero, since these
determine the relaying of maternal nutrient factors to the fetal tissues for growth and
development. Hence, due to the interplay of maternal-fetal placental connections, maternal and
placental factors determine the rapid rate of infant growth in utero as compared to any other
stage (Sharma et al., 2016).
Question 3: Findings of IUGR infants on:
8LIFESPAN NUTRITION
a) Weight and height during childhood: IUGR infants have been observed to born small
for gestational age, with effects on childhood resulting in being 7 cm shorted and 4 kg
lighter during childhood, at 4 years of age. However, conflicting results are presented in
current literature with studies indicating IUGR babies acquiring normal weight and
height by 2 years of age (Galan, 2015).
b) Risk factors for disease in later life: IUGR infants have been associated with greater
susceptibilities towards disorders such as chronic lung disease, necrotizing enterocolitis,
hypoxia and brain injury, low Apgar score, nephropathy due to decreased glomerular
filtration rate, cerebral palsy, behavioral disorder and cognitive deficits such as poor
memory, intelligence quotient and language comprehension (Murray et al., 2015).
a) Weight and height during childhood: IUGR infants have been observed to born small
for gestational age, with effects on childhood resulting in being 7 cm shorted and 4 kg
lighter during childhood, at 4 years of age. However, conflicting results are presented in
current literature with studies indicating IUGR babies acquiring normal weight and
height by 2 years of age (Galan, 2015).
b) Risk factors for disease in later life: IUGR infants have been associated with greater
susceptibilities towards disorders such as chronic lung disease, necrotizing enterocolitis,
hypoxia and brain injury, low Apgar score, nephropathy due to decreased glomerular
filtration rate, cerebral palsy, behavioral disorder and cognitive deficits such as poor
memory, intelligence quotient and language comprehension (Murray et al., 2015).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9LIFESPAN NUTRITION
Module 3
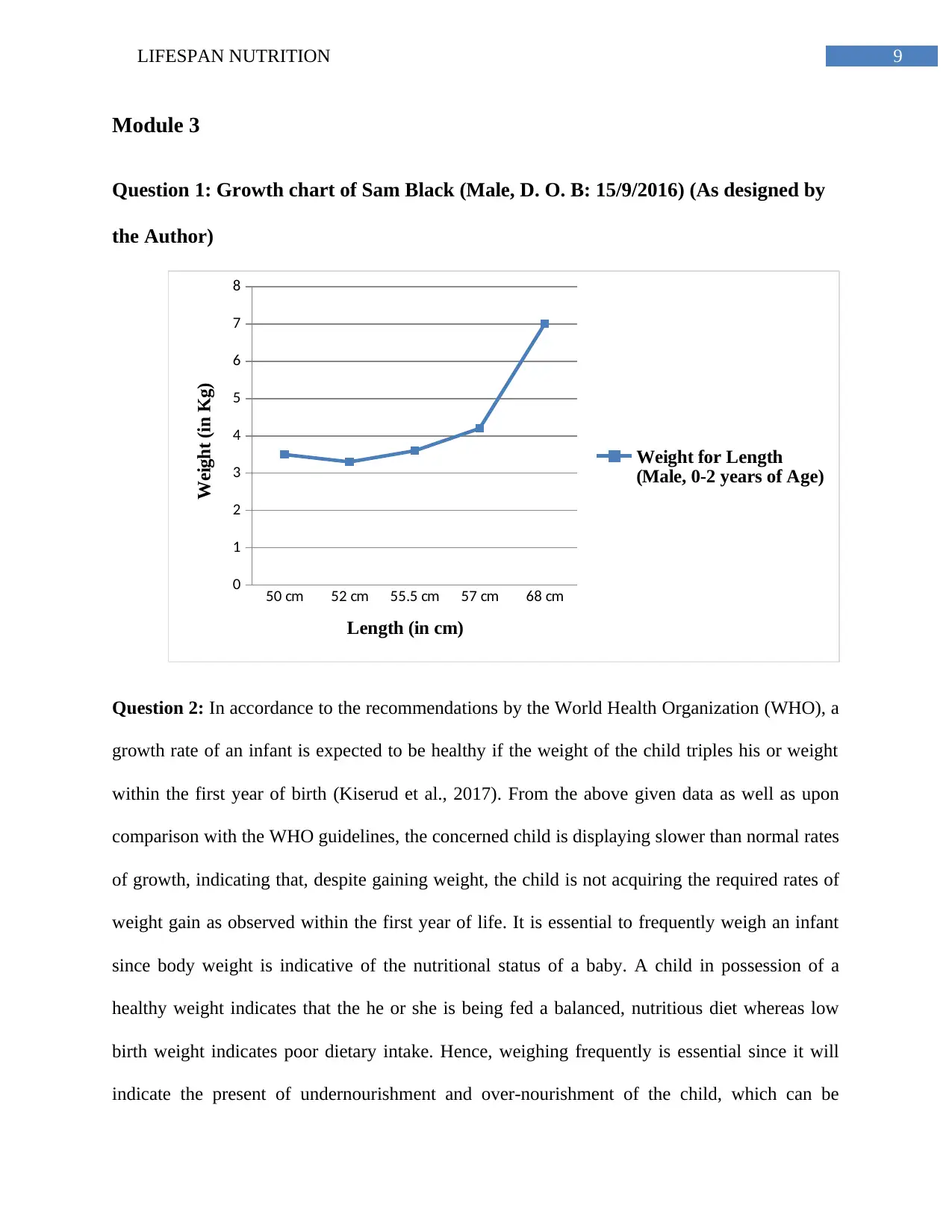
Question 1: Growth chart of Sam Black (Male, D. O. B: 15/9/2016) (As designed by
the Author)
50 cm 52 cm 55.5 cm 57 cm 68 cm
0
1
2
3
4
5
6
7
8
Weight for Length
(Male, 0-2 years of Age)
Length (in cm)
Weight (in Kg)
Question 2: In accordance to the recommendations by the World Health Organization (WHO), a
growth rate of an infant is expected to be healthy if the weight of the child triples his or weight
within the first year of birth (Kiserud et al., 2017). From the above given data as well as upon
comparison with the WHO guidelines, the concerned child is displaying slower than normal rates
of growth, indicating that, despite gaining weight, the child is not acquiring the required rates of
weight gain as observed within the first year of life. It is essential to frequently weigh an infant
since body weight is indicative of the nutritional status of a baby. A child in possession of a
healthy weight indicates that the he or she is being fed a balanced, nutritious diet whereas low
birth weight indicates poor dietary intake. Hence, weighing frequently is essential since it will
indicate the present of undernourishment and over-nourishment of the child, which can be
Module 3
Question 1: Growth chart of Sam Black (Male, D. O. B: 15/9/2016) (As designed by
the Author)
50 cm 52 cm 55.5 cm 57 cm 68 cm
0
1
2
3
4
5
6
7
8
Weight for Length
(Male, 0-2 years of Age)
Length (in cm)
Weight (in Kg)
Question 2: In accordance to the recommendations by the World Health Organization (WHO), a
growth rate of an infant is expected to be healthy if the weight of the child triples his or weight
within the first year of birth (Kiserud et al., 2017). From the above given data as well as upon
comparison with the WHO guidelines, the concerned child is displaying slower than normal rates
of growth, indicating that, despite gaining weight, the child is not acquiring the required rates of
weight gain as observed within the first year of life. It is essential to frequently weigh an infant
since body weight is indicative of the nutritional status of a baby. A child in possession of a
healthy weight indicates that the he or she is being fed a balanced, nutritious diet whereas low
birth weight indicates poor dietary intake. Hence, weighing frequently is essential since it will
indicate the present of undernourishment and over-nourishment of the child, which can be
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10LIFESPAN NUTRITION
modified accordingly in the future to ensure healthy growth and development (Kiserud et al.,
2018).
Question 3: Distinctions concerning nutritional recommendations are made between infants
receiving breast milk and formula milk, due to the nutritional completeness in breast milk.
Despite modern day formulas being nutritionally adequate, they are still devoid of the essential
antibodies and the ability to change in composition as per the changing needs of the infant.
Hence, a distinction is made between formula fed and breast fed babies where parents of the
former are firstly educated on the importance of breast milk (Clark et al., 2017). Likewise, breast
milk is one of the most natural and sterile source of nutrition for infants and is nutritionally
complete in all required nutrients. Hence, parents feeding formulas to infants are provided with
distinctive recommendations where they are asked to prepare the formula using correct
procedures and in sterile conditions to prevent contamination and over or under nutrition (Pierro
et al., 2016).
References
Atkins, L. A., McNaughton, S. A., Spence, A. C., & Szymlek-Gay, E. A. (2019). Adequacy of
iron intakes and socio-demographic factors associated with iron intakes of Australian pre-
schoolers. European journal of nutrition, 1-10.
Australian Bureau of Statistics (2019). Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12. [online] Ausstats.abs.gov.au. Available at:
http://www.ausstats.abs.gov.au/Ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf [Accessed 26 Feb. 2019].
modified accordingly in the future to ensure healthy growth and development (Kiserud et al.,
2018).
Question 3: Distinctions concerning nutritional recommendations are made between infants
receiving breast milk and formula milk, due to the nutritional completeness in breast milk.
Despite modern day formulas being nutritionally adequate, they are still devoid of the essential
antibodies and the ability to change in composition as per the changing needs of the infant.
Hence, a distinction is made between formula fed and breast fed babies where parents of the
former are firstly educated on the importance of breast milk (Clark et al., 2017). Likewise, breast
milk is one of the most natural and sterile source of nutrition for infants and is nutritionally
complete in all required nutrients. Hence, parents feeding formulas to infants are provided with
distinctive recommendations where they are asked to prepare the formula using correct
procedures and in sterile conditions to prevent contamination and over or under nutrition (Pierro
et al., 2016).
References
Atkins, L. A., McNaughton, S. A., Spence, A. C., & Szymlek-Gay, E. A. (2019). Adequacy of
iron intakes and socio-demographic factors associated with iron intakes of Australian pre-
schoolers. European journal of nutrition, 1-10.
Australian Bureau of Statistics (2019). Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12. [online] Ausstats.abs.gov.au. Available at:
http://www.ausstats.abs.gov.au/Ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf [Accessed 26 Feb. 2019].
11LIFESPAN NUTRITION
Australian Dietary Guidelines. (2019). Eat for Health. Retrieved from
https://www.eatforhealth.gov.au/sites/default/files/files/the_guidelines/
n55_australian_dietary_guidelines.pdf.
Australian Government Department of Health. (2019). Weight and body mass index | Australian
Government Department of Health. Retrieved from
https://beta.health.gov.au/resources/pregnancy-care-guidelines/part-d-clinical-
assessments/weight-and-body-mass-index.
Carr, A. C., Rosengrave, P. C., Bayer, S., Chambers, S., Mehrtens, J., & Shaw, G. M. (2017).
Hypovitaminosis C and vitamin C deficiency in critically ill patients despite
recommended enteral and parenteral intakes. Critical Care, 21(1), 300.
Carrasco-Luna, J., Gombert, M., Carrasco-García, Á., & Codoñer-Franch, P. (2018). Adolescent
Feeding: Nutritional Risk Factors. Journal of Child Science, 8(01), e99-e105.
Chassen, S. S., Ferchaud-Roucher, V., Gupta, M. B., Jansson, T., & Powell, T. L. (2018).
Alterations in placental long chain polyunsaturated fatty acid metabolism in human
intrauterine growth restriction. Clinical Science, 132(5), 595-607.
Clark, K. M., Li, M., Zhu, B., Liang, F., Shao, J., Zhang, Y., ... & Lozoff, B. (2017).
Breastfeeding, mixed, or formula feeding at 9 months of age and the prevalence of iron
deficiency and iron deficiency anemia in two cohorts of infants in China. The Journal of
pediatrics, 181, 56-61.
Cohen, E., Wong, F. Y., Horne, R. S., & Yiallourou, S. R. (2016). Intrauterine growth restriction:
impact on cardiovascular development and function throughout infancy. Pediatric
research, 79(6), 821.
Australian Dietary Guidelines. (2019). Eat for Health. Retrieved from
https://www.eatforhealth.gov.au/sites/default/files/files/the_guidelines/
n55_australian_dietary_guidelines.pdf.
Australian Government Department of Health. (2019). Weight and body mass index | Australian
Government Department of Health. Retrieved from
https://beta.health.gov.au/resources/pregnancy-care-guidelines/part-d-clinical-
assessments/weight-and-body-mass-index.
Carr, A. C., Rosengrave, P. C., Bayer, S., Chambers, S., Mehrtens, J., & Shaw, G. M. (2017).
Hypovitaminosis C and vitamin C deficiency in critically ill patients despite
recommended enteral and parenteral intakes. Critical Care, 21(1), 300.
Carrasco-Luna, J., Gombert, M., Carrasco-García, Á., & Codoñer-Franch, P. (2018). Adolescent
Feeding: Nutritional Risk Factors. Journal of Child Science, 8(01), e99-e105.
Chassen, S. S., Ferchaud-Roucher, V., Gupta, M. B., Jansson, T., & Powell, T. L. (2018).
Alterations in placental long chain polyunsaturated fatty acid metabolism in human
intrauterine growth restriction. Clinical Science, 132(5), 595-607.
Clark, K. M., Li, M., Zhu, B., Liang, F., Shao, J., Zhang, Y., ... & Lozoff, B. (2017).
Breastfeeding, mixed, or formula feeding at 9 months of age and the prevalence of iron
deficiency and iron deficiency anemia in two cohorts of infants in China. The Journal of
pediatrics, 181, 56-61.
Cohen, E., Wong, F. Y., Horne, R. S., & Yiallourou, S. R. (2016). Intrauterine growth restriction:
impact on cardiovascular development and function throughout infancy. Pediatric
research, 79(6), 821.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 29

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.