Lifespan Nutrition Case Study: Assessing Dietary Adequacy in Aged Care
VerifiedAdded on 2022/10/13
|14
|3863
|13
Case Study
AI Summary
This assignment presents a comprehensive case study on lifespan nutrition within an aged care facility. The student analyzes the dietary adequacy of an elderly resident, Agnes, assessing her nutritional intake against recommended values and identifying key concerns such as excessive sodium, sugar, and saturated fat intake, along with deficiencies in calcium, water, and essential nutrients. The study explores physiological changes associated with aging, like neuronal atrophy, muscle loss (sarcopenia), and bone density reduction, and their impact on nutritional needs. It investigates indicators of osteoporosis and dietary risk factors. The analysis includes detailed tables of nutrient intake, food group consumption, and comparisons to Australian Dietary Guidelines. The student identifies potential underlying issues, such as chronic diseases and sensory limitations, and proposes strategies to improve Agnes's diet, including nutritional health literacy programs, outdoor activities, and modifications to the facility's menu. The suggested changes include replacing processed foods with healthier alternatives, adjusting fat and sugar content, and incorporating texture-modified foods to aid ingestion and digestion. The assignment also involves creating a fact sheet for residents and their families to promote improved dietary intake.

Running head: LIFESPAN NUTRITION FOR THE ELDERLY
LIFESPAN NUTRITION FOR THE ELDERLY
Name of the Student:
Name of the University:
Author note:
LIFESPAN NUTRITION FOR THE ELDERLY
Name of the Student:
Name of the University:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1LIFESPAN NUTRITION FOR THE ELDERY
Part A
Physiological Changes
Neurological based physiological changes are prevalent physiological changes of concern
within the elderly. Ageing is associated with a neuronal atrophy and cerebral cortex shrinkage,
largely due to increased rates of free radical formation and inflammation within an aged person.
Such inflammatory processes also result in the formation and deposition of pro-inflammatory
pigments and components like lipofuscin and advanced glycated end products (AGEs) [1]. Such
neuronal degradation increase the susceptibility of cognitive disorders like Alzheimer’s and
dementia within the aged person. Additionally, enhanced pro-inflammatory mechanisms within
the elderly reduce the strength of their immune system and increase their risk of chronic
metabolic diseases like cardiovascular diseases, diabetes, renal and kidney malfunctioning and
even cancers [2]. Such detrimental changes must be looked into by the aged care facility since
these enhanced the nutritional need for consuming diets rich in protective micronutrients like
antioxidants, vitamin C, vitamin E, polyphenols and flavonoids [3].
As a person ages, the rate of muscle breakdown and catabolism increases as compared to
muscle buildup or ‘anabolism’. This results in a negative energy balance and a state of
sarcopenia, extensive loss of muscle and frailty within the elderly [4]. In addition to the above,
rates of calcification and remodeling of bones also decreases within the elderly which results in
the loss of bone mass, density and strength of the skeletal system. Such musculoskeletal changes
within an aged person must be considered by the aged care facility since these increase their
nutritional needs of consuming body building macro and micronutrients like proteins, calcium,
phosphorous and vitamin D [5].
Part A
Physiological Changes
Neurological based physiological changes are prevalent physiological changes of concern
within the elderly. Ageing is associated with a neuronal atrophy and cerebral cortex shrinkage,
largely due to increased rates of free radical formation and inflammation within an aged person.
Such inflammatory processes also result in the formation and deposition of pro-inflammatory
pigments and components like lipofuscin and advanced glycated end products (AGEs) [1]. Such
neuronal degradation increase the susceptibility of cognitive disorders like Alzheimer’s and
dementia within the aged person. Additionally, enhanced pro-inflammatory mechanisms within
the elderly reduce the strength of their immune system and increase their risk of chronic
metabolic diseases like cardiovascular diseases, diabetes, renal and kidney malfunctioning and
even cancers [2]. Such detrimental changes must be looked into by the aged care facility since
these enhanced the nutritional need for consuming diets rich in protective micronutrients like
antioxidants, vitamin C, vitamin E, polyphenols and flavonoids [3].
As a person ages, the rate of muscle breakdown and catabolism increases as compared to
muscle buildup or ‘anabolism’. This results in a negative energy balance and a state of
sarcopenia, extensive loss of muscle and frailty within the elderly [4]. In addition to the above,
rates of calcification and remodeling of bones also decreases within the elderly which results in
the loss of bone mass, density and strength of the skeletal system. Such musculoskeletal changes
within an aged person must be considered by the aged care facility since these increase their
nutritional needs of consuming body building macro and micronutrients like proteins, calcium,
phosphorous and vitamin D [5].
2LIFESPAN NUTRITION FOR THE ELDERY
Nutritional Concerns
Along with physiological changes, old age is also accompanied by a number of
nutritional concerns which must be considered by the aged care facility. One of the most
common concerns exerting severe negative implications is the loss of appetite within the elderly
[6]. With ageing and the associated alterations in nervous system functioning, an old person is
likely to lose their olfactory abilities – resulting in reduced sensory receptor functioning in the
nose and taste buds. This impacts taste and smell sensations and thus, an inability to gain
pleasurable experiences from foods [7]. Further, aged-associated reductions in esophageal
peristalsis makes it difficult for an aged person to swallow foods. Such muscular and sensory
changes contribute to low appetite, inadequate food consumption and poor nutritional status
within the elderly, further aggravating sarcopenia [8]. Additionally, ageing results in decreased
gastric acid secretions and associated indigestion, diarrhea and gastrointestinal disorders. Such
digestive problems affect food intake as well as nutrient absorption within the elderly, hence
contributing to their poor nutritional status and frailty. Thus, it is suggested that the menu
provided by the aged care facility is nutritionally balanced, comprising of core food groups as
per the Australian Dietary Guidelines (ADGs) and modified or softened in terms of texture [9].
Osteoporosis Indicators
Osteoporosis is a chronic bone disease associated with fragile and porous bones, due to
the interplay of a number of risk factors prevalent within the elderly. Anthropometric risk factors
include a state of frailty and inadequately low body mass since it is indicative of decreased
strength of weight bearing joints [10]. Since osteoporosis is directly associated with increased
osteoclastic processes – it is likely that the key biochemical and clinical risk factors include:
inadequately low serum levels of calcium, vitamin D and phosphorous and a bone density 2.5
Nutritional Concerns
Along with physiological changes, old age is also accompanied by a number of
nutritional concerns which must be considered by the aged care facility. One of the most
common concerns exerting severe negative implications is the loss of appetite within the elderly
[6]. With ageing and the associated alterations in nervous system functioning, an old person is
likely to lose their olfactory abilities – resulting in reduced sensory receptor functioning in the
nose and taste buds. This impacts taste and smell sensations and thus, an inability to gain
pleasurable experiences from foods [7]. Further, aged-associated reductions in esophageal
peristalsis makes it difficult for an aged person to swallow foods. Such muscular and sensory
changes contribute to low appetite, inadequate food consumption and poor nutritional status
within the elderly, further aggravating sarcopenia [8]. Additionally, ageing results in decreased
gastric acid secretions and associated indigestion, diarrhea and gastrointestinal disorders. Such
digestive problems affect food intake as well as nutrient absorption within the elderly, hence
contributing to their poor nutritional status and frailty. Thus, it is suggested that the menu
provided by the aged care facility is nutritionally balanced, comprising of core food groups as
per the Australian Dietary Guidelines (ADGs) and modified or softened in terms of texture [9].
Osteoporosis Indicators
Osteoporosis is a chronic bone disease associated with fragile and porous bones, due to
the interplay of a number of risk factors prevalent within the elderly. Anthropometric risk factors
include a state of frailty and inadequately low body mass since it is indicative of decreased
strength of weight bearing joints [10]. Since osteoporosis is directly associated with increased
osteoclastic processes – it is likely that the key biochemical and clinical risk factors include:
inadequately low serum levels of calcium, vitamin D and phosphorous and a bone density 2.5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3LIFESPAN NUTRITION FOR THE ELDERY
standards deviations less than mean adult values. Decreased bone calcification is directly linked
to an inadequate consumption of calcium and hence, dietary assessment risk factors include
inadequate consumption of calcium and vitamin D-rich foods like dairy, soy, seeds and nuts [11].
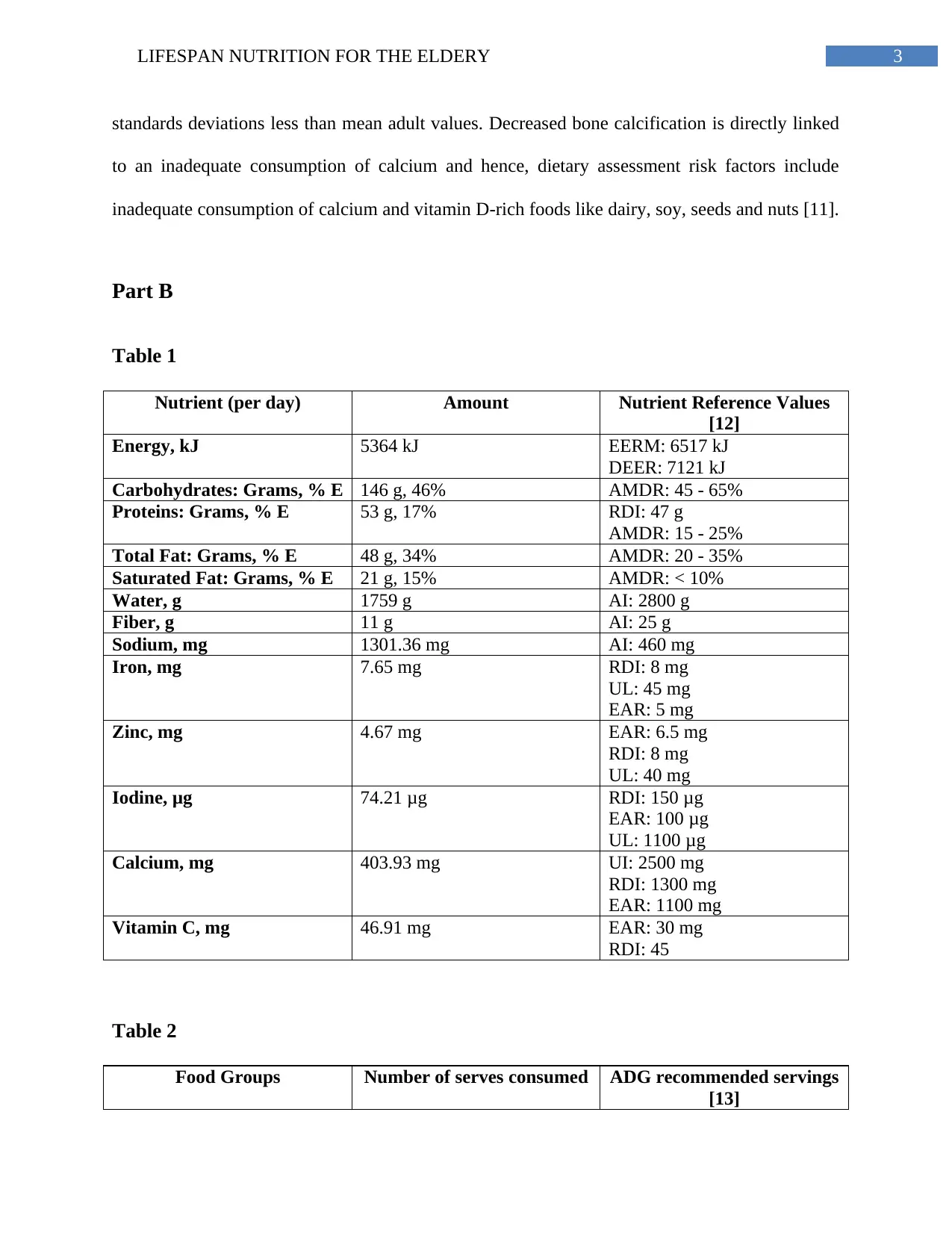
Part B
Table 1
Nutrient (per day) Amount Nutrient Reference Values
[12]
Energy, kJ 5364 kJ EERM: 6517 kJ
DEER: 7121 kJ
Carbohydrates: Grams, % E 146 g, 46% AMDR: 45 - 65%
Proteins: Grams, % E 53 g, 17% RDI: 47 g
AMDR: 15 - 25%
Total Fat: Grams, % E 48 g, 34% AMDR: 20 - 35%
Saturated Fat: Grams, % E 21 g, 15% AMDR: < 10%
Water, g 1759 g AI: 2800 g
Fiber, g 11 g AI: 25 g
Sodium, mg 1301.36 mg AI: 460 mg
Iron, mg 7.65 mg RDI: 8 mg
UL: 45 mg
EAR: 5 mg
Zinc, mg 4.67 mg EAR: 6.5 mg
RDI: 8 mg
UL: 40 mg
Iodine, μg 74.21 μg RDI: 150 μg
EAR: 100 μg
UL: 1100 μg
Calcium, mg 403.93 mg UI: 2500 mg
RDI: 1300 mg
EAR: 1100 mg
Vitamin C, mg 46.91 mg EAR: 30 mg
RDI: 45
Table 2
Food Groups Number of serves consumed ADG recommended servings
[13]
standards deviations less than mean adult values. Decreased bone calcification is directly linked
to an inadequate consumption of calcium and hence, dietary assessment risk factors include
inadequate consumption of calcium and vitamin D-rich foods like dairy, soy, seeds and nuts [11].
Part B
Table 1
Nutrient (per day) Amount Nutrient Reference Values
[12]
Energy, kJ 5364 kJ EERM: 6517 kJ
DEER: 7121 kJ
Carbohydrates: Grams, % E 146 g, 46% AMDR: 45 - 65%
Proteins: Grams, % E 53 g, 17% RDI: 47 g
AMDR: 15 - 25%
Total Fat: Grams, % E 48 g, 34% AMDR: 20 - 35%
Saturated Fat: Grams, % E 21 g, 15% AMDR: < 10%
Water, g 1759 g AI: 2800 g
Fiber, g 11 g AI: 25 g
Sodium, mg 1301.36 mg AI: 460 mg
Iron, mg 7.65 mg RDI: 8 mg
UL: 45 mg
EAR: 5 mg
Zinc, mg 4.67 mg EAR: 6.5 mg
RDI: 8 mg
UL: 40 mg
Iodine, μg 74.21 μg RDI: 150 μg
EAR: 100 μg
UL: 1100 μg
Calcium, mg 403.93 mg UI: 2500 mg
RDI: 1300 mg
EAR: 1100 mg
Vitamin C, mg 46.91 mg EAR: 30 mg
RDI: 45
Table 2
Food Groups Number of serves consumed ADG recommended servings
[13]
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4LIFESPAN NUTRITION FOR THE ELDERY
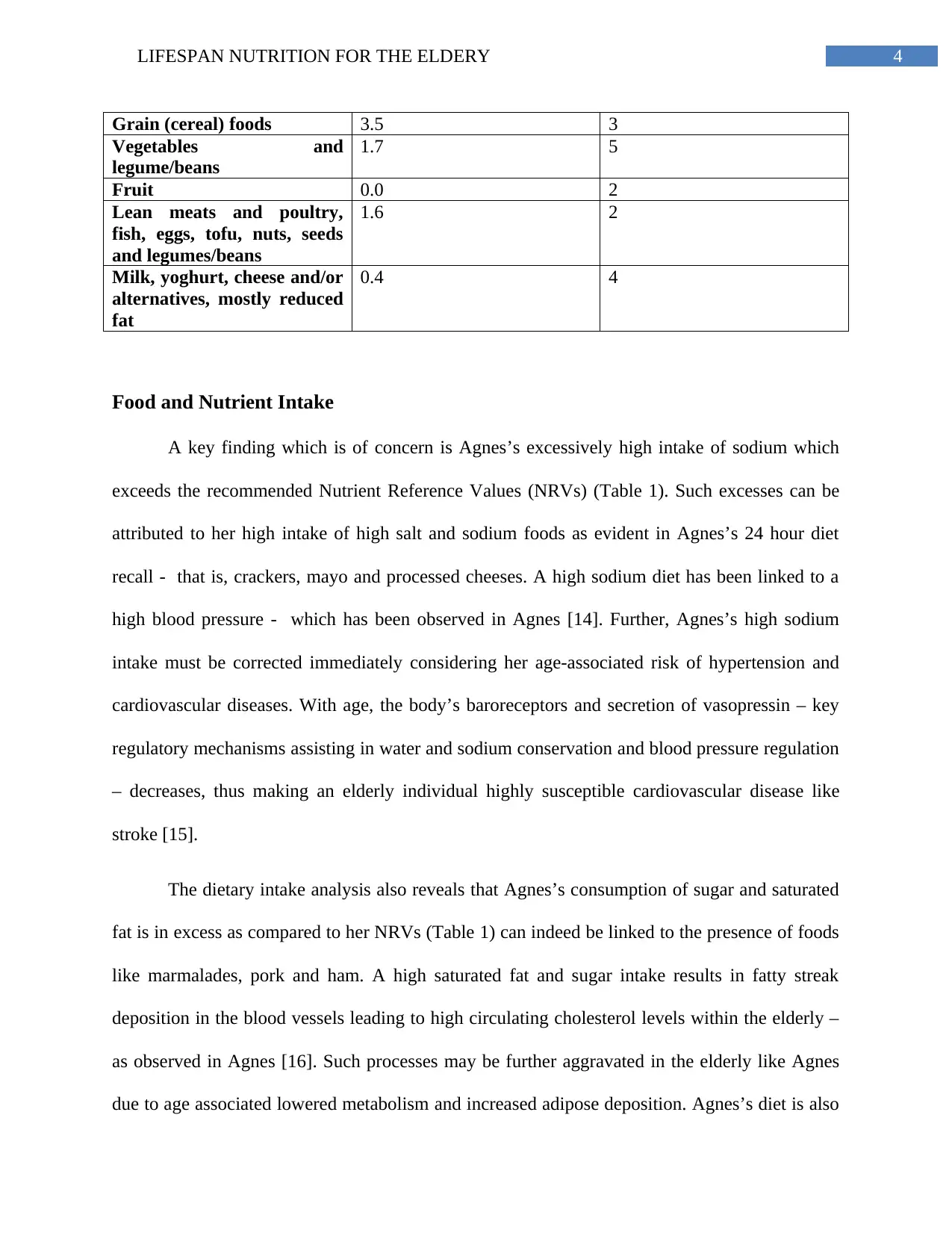
Grain (cereal) foods 3.5 3
Vegetables and
legume/beans
1.7 5
Fruit 0.0 2
Lean meats and poultry,
fish, eggs, tofu, nuts, seeds
and legumes/beans
1.6 2
Milk, yoghurt, cheese and/or
alternatives, mostly reduced
fat
0.4 4
Food and Nutrient Intake
A key finding which is of concern is Agnes’s excessively high intake of sodium which
exceeds the recommended Nutrient Reference Values (NRVs) (Table 1). Such excesses can be
attributed to her high intake of high salt and sodium foods as evident in Agnes’s 24 hour diet
recall - that is, crackers, mayo and processed cheeses. A high sodium diet has been linked to a
high blood pressure - which has been observed in Agnes [14]. Further, Agnes’s high sodium
intake must be corrected immediately considering her age-associated risk of hypertension and
cardiovascular diseases. With age, the body’s baroreceptors and secretion of vasopressin – key
regulatory mechanisms assisting in water and sodium conservation and blood pressure regulation
– decreases, thus making an elderly individual highly susceptible cardiovascular disease like
stroke [15].
The dietary intake analysis also reveals that Agnes’s consumption of sugar and saturated
fat is in excess as compared to her NRVs (Table 1) can indeed be linked to the presence of foods
like marmalades, pork and ham. A high saturated fat and sugar intake results in fatty streak
deposition in the blood vessels leading to high circulating cholesterol levels within the elderly –
as observed in Agnes [16]. Such processes may be further aggravated in the elderly like Agnes
due to age associated lowered metabolism and increased adipose deposition. Agnes’s diet is also
Grain (cereal) foods 3.5 3
Vegetables and
legume/beans
1.7 5
Fruit 0.0 2
Lean meats and poultry,
fish, eggs, tofu, nuts, seeds
and legumes/beans
1.6 2
Milk, yoghurt, cheese and/or
alternatives, mostly reduced
fat
0.4 4
Food and Nutrient Intake
A key finding which is of concern is Agnes’s excessively high intake of sodium which
exceeds the recommended Nutrient Reference Values (NRVs) (Table 1). Such excesses can be
attributed to her high intake of high salt and sodium foods as evident in Agnes’s 24 hour diet
recall - that is, crackers, mayo and processed cheeses. A high sodium diet has been linked to a
high blood pressure - which has been observed in Agnes [14]. Further, Agnes’s high sodium
intake must be corrected immediately considering her age-associated risk of hypertension and
cardiovascular diseases. With age, the body’s baroreceptors and secretion of vasopressin – key
regulatory mechanisms assisting in water and sodium conservation and blood pressure regulation
– decreases, thus making an elderly individual highly susceptible cardiovascular disease like
stroke [15].
The dietary intake analysis also reveals that Agnes’s consumption of sugar and saturated
fat is in excess as compared to her NRVs (Table 1) can indeed be linked to the presence of foods
like marmalades, pork and ham. A high saturated fat and sugar intake results in fatty streak
deposition in the blood vessels leading to high circulating cholesterol levels within the elderly –
as observed in Agnes [16]. Such processes may be further aggravated in the elderly like Agnes
due to age associated lowered metabolism and increased adipose deposition. Agnes’s diet is also
5LIFESPAN NUTRITION FOR THE ELDERY
found to be low in protective unsaturated fats and oils (Table 2). If not controlled, such excesses
can work simultaneously with hypertension and increase Agnes’s risk of fatal coronary diseases
[17].
Agnes’s dietary intake and serving size consumption (Table 1, Table 2) reveals an
inadequate intake of calcium in her diet. Indeed, Agnes’s consumption of foods like dairy, seeds
and legumes is extremely low – a major risk factor for osteoporosis and fractures [18]. Lastly,
Agnes’s diet is revealed to be devoid of adequate water, vegetable and fruit content. A lack of
water intake and dehydration is linked to excessive production of the ant-diuretic hormone
vasopressin, resulting in hypertension [19]. Further low vegetable and fruit intake results in poor
antioxidant consumption, oxidative stress and increased risk of chronic metabolic diseases thus
calling for immediate mitigation in Agnes [20].
Other Indicators
A number of reasons can contribute to poor appetite within an aged person of which,
presence of disease is a major concern. It has been evidenced that chronic conditions like cancer,
cardiovascular conditions, diseases of the liver and kidney, pulmonary disorders and obstructions
in the gastrointestinal tract, can impair appetite within an aged individual [21]. Thus, additional
information would include understanding whether Agnes’s appetite is linked to any chronic
disease for which the age care facility must conduct health assessments like cardiovascular,
abdominal, respiratory, vital signs, liver and kidney assessments as well as biochemical tests
[22].
A key contributor to poor appetite within the elderly, as discussed previously is the
availability of foods which are too hard or firm in texture or have been inadequately flavored to
found to be low in protective unsaturated fats and oils (Table 2). If not controlled, such excesses
can work simultaneously with hypertension and increase Agnes’s risk of fatal coronary diseases
[17].
Agnes’s dietary intake and serving size consumption (Table 1, Table 2) reveals an
inadequate intake of calcium in her diet. Indeed, Agnes’s consumption of foods like dairy, seeds
and legumes is extremely low – a major risk factor for osteoporosis and fractures [18]. Lastly,
Agnes’s diet is revealed to be devoid of adequate water, vegetable and fruit content. A lack of
water intake and dehydration is linked to excessive production of the ant-diuretic hormone
vasopressin, resulting in hypertension [19]. Further low vegetable and fruit intake results in poor
antioxidant consumption, oxidative stress and increased risk of chronic metabolic diseases thus
calling for immediate mitigation in Agnes [20].
Other Indicators
A number of reasons can contribute to poor appetite within an aged person of which,
presence of disease is a major concern. It has been evidenced that chronic conditions like cancer,
cardiovascular conditions, diseases of the liver and kidney, pulmonary disorders and obstructions
in the gastrointestinal tract, can impair appetite within an aged individual [21]. Thus, additional
information would include understanding whether Agnes’s appetite is linked to any chronic
disease for which the age care facility must conduct health assessments like cardiovascular,
abdominal, respiratory, vital signs, liver and kidney assessments as well as biochemical tests
[22].
A key contributor to poor appetite within the elderly, as discussed previously is the
availability of foods which are too hard or firm in texture or have been inadequately flavored to
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6LIFESPAN NUTRITION FOR THE ELDERY
suit the palates and digestive ability of the elderly [23]. Thus, to understand whether Agnes’s
poor dietary intake is due to poor sensory qualities of the facility’s menu, a 9 point hedonic
sensory examination can be conducted where Agnes can rate foods based on her likes and
dislikes accordingly. This can be helpful in understand whether Agnes’s poor dietary intake is
linked to the way in which foods are prepared at the facility [24]. In addition to a sensory
evaluation, comparing the facility’s foods with the guidelines stipulated in the Australian
Standards for Texture Modified Foods and Fluids can assist in identifying texture discrepancies
which can contribute to low food intake n Agnes [25].
Poor food intake is also linked to orthorexia – a condition where an individual’s
eagerness towards food consumption decreases, due to psychological, social and underlying
mental health issues. To assess whether the same is present in Agnes, conducting an assessment
such as the Bratman Test for Orthorexia will be beneficial and pave the way for further
assessments [26].
Strategies
1. It is known that families visiting the facility are allowed to bring food for the residents.
To ensure healthy food choices from homes, it advisable if the aged care facility arranges
for a nutritional health literacy program where both families and residents can participate.
This will include a short educational session on the importance of consuming a balanced
diet, strategies for healthy food preparation and importance of exercise or outdoor
activities. This will be helpful in enhancing the awareness of residents and families on the
ways in which food intake and disease prevention can be improved [27].
2. A notable information from Agnes’s case scenario is her low engagement in outdoor
activities. Low exposure to sunlight is directly linked to vitamin D deficiency and bone
suit the palates and digestive ability of the elderly [23]. Thus, to understand whether Agnes’s
poor dietary intake is due to poor sensory qualities of the facility’s menu, a 9 point hedonic
sensory examination can be conducted where Agnes can rate foods based on her likes and
dislikes accordingly. This can be helpful in understand whether Agnes’s poor dietary intake is
linked to the way in which foods are prepared at the facility [24]. In addition to a sensory
evaluation, comparing the facility’s foods with the guidelines stipulated in the Australian
Standards for Texture Modified Foods and Fluids can assist in identifying texture discrepancies
which can contribute to low food intake n Agnes [25].
Poor food intake is also linked to orthorexia – a condition where an individual’s
eagerness towards food consumption decreases, due to psychological, social and underlying
mental health issues. To assess whether the same is present in Agnes, conducting an assessment
such as the Bratman Test for Orthorexia will be beneficial and pave the way for further
assessments [26].
Strategies
1. It is known that families visiting the facility are allowed to bring food for the residents.
To ensure healthy food choices from homes, it advisable if the aged care facility arranges
for a nutritional health literacy program where both families and residents can participate.
This will include a short educational session on the importance of consuming a balanced
diet, strategies for healthy food preparation and importance of exercise or outdoor
activities. This will be helpful in enhancing the awareness of residents and families on the
ways in which food intake and disease prevention can be improved [27].
2. A notable information from Agnes’s case scenario is her low engagement in outdoor
activities. Low exposure to sunlight is directly linked to vitamin D deficiency and bone
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7LIFESPAN NUTRITION FOR THE ELDERY
disorders. The beneficial strategy which can be undertaken to ensure positive health
outcomes in Agnes is an implementation of enjoyable social activities outdoors which
can encourage social interaction as well as exposure to essential sunlight [28].
3. The case scenario reveals that Agnes’s diet is rich in processed foods like packaged
juices, crackers, mayonnaise, cheeses and marmalades, which are likely to be
contributing to her high sodium and sugar intake. To prevent such nutrient excesses and
to mitigate nutrient deficiencies in terms of the fiber, mineral and vitamin content, it is
advisable that the aged care facility replace the above foods with homemade fruits
spreads, low salt whole meal breads and pastas and freshly prepared cheeses from low fat
milk [29].
4. To improve Agnes’s calcium intake without increasing her intake of saturated fat, it is
advisable that the aged care facility replace any whole milk or processed cheese varieties
with reduced fat variations like skimmed milk, low fat feta or cottage cheese and yoghurt
or low fat milk beverages. Additional of soy based beverages and products, legumes,
seeds and nuts are also equally beneficial non-dairy sources which can improve Agnes’s
calcium, fiber, zinc and iron intake [30].
5. To prevent Agnes’s cardiovascular disease risk due to saturated fat intake, it is advisable
that the aged care facility replace foods like red meats, butter and cheeses with lean or
vegetarian protein rich foods like chicken and fatty fish without the skin, fortified eggs,
soy and legumes. This will in turn improver her intake of anti-inflammatory, omega 3
fatty acids [31].
6. The aged care facility must replace crackers and cheese with healthier snack options like
whole wheat sandwiches, dry fruits and toasted seeds and nuts. Such choices will control
disorders. The beneficial strategy which can be undertaken to ensure positive health
outcomes in Agnes is an implementation of enjoyable social activities outdoors which
can encourage social interaction as well as exposure to essential sunlight [28].
3. The case scenario reveals that Agnes’s diet is rich in processed foods like packaged
juices, crackers, mayonnaise, cheeses and marmalades, which are likely to be
contributing to her high sodium and sugar intake. To prevent such nutrient excesses and
to mitigate nutrient deficiencies in terms of the fiber, mineral and vitamin content, it is
advisable that the aged care facility replace the above foods with homemade fruits
spreads, low salt whole meal breads and pastas and freshly prepared cheeses from low fat
milk [29].
4. To improve Agnes’s calcium intake without increasing her intake of saturated fat, it is
advisable that the aged care facility replace any whole milk or processed cheese varieties
with reduced fat variations like skimmed milk, low fat feta or cottage cheese and yoghurt
or low fat milk beverages. Additional of soy based beverages and products, legumes,
seeds and nuts are also equally beneficial non-dairy sources which can improve Agnes’s
calcium, fiber, zinc and iron intake [30].
5. To prevent Agnes’s cardiovascular disease risk due to saturated fat intake, it is advisable
that the aged care facility replace foods like red meats, butter and cheeses with lean or
vegetarian protein rich foods like chicken and fatty fish without the skin, fortified eggs,
soy and legumes. This will in turn improver her intake of anti-inflammatory, omega 3
fatty acids [31].
6. The aged care facility must replace crackers and cheese with healthier snack options like
whole wheat sandwiches, dry fruits and toasted seeds and nuts. Such choices will control
8LIFESPAN NUTRITION FOR THE ELDERY
her saturated fat intake and increase her intake of unsaturated fats, fiber, iron and calcium
[32].
7. To ensure that Agnes is not encountering any difficulties in terms of ingestion of food, it
is recommended that the aged care facility incorporate soft foods such as gruels,
porridges, smoothies and juices. To improve the nutrient content in such foods, adding
fruit and vegetable purees, cooked meal and nut and seed pastes can prove to be
beneficial. Texture modification will not ensure improved dietary intake but also
improved digestion and nutrient absorption in Agnes [33].
8. Lastly, to ensure that the menu provided by the facility is balanced in terms of all core
food groups and hence, beneficial for the residents to maintain optimum nutritional
status, it is recommended that the staff prepare foods and the menu as per the
recommendations stipulated by the ADGs [34].
her saturated fat intake and increase her intake of unsaturated fats, fiber, iron and calcium
[32].
7. To ensure that Agnes is not encountering any difficulties in terms of ingestion of food, it
is recommended that the aged care facility incorporate soft foods such as gruels,
porridges, smoothies and juices. To improve the nutrient content in such foods, adding
fruit and vegetable purees, cooked meal and nut and seed pastes can prove to be
beneficial. Texture modification will not ensure improved dietary intake but also
improved digestion and nutrient absorption in Agnes [33].
8. Lastly, to ensure that the menu provided by the facility is balanced in terms of all core
food groups and hence, beneficial for the residents to maintain optimum nutritional
status, it is recommended that the staff prepare foods and the menu as per the
recommendations stipulated by the ADGs [34].
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9LIFESPAN NUTRITION FOR THE ELDERY
References
1. Hepple RT, Rice CL. Innervation and neuromuscular control in ageing skeletal muscle.
The Journal of physiology. 2016 Apr 15;594(8):1965-78.
2. Rawji KS, Mishra MK, Michaels NJ, Rivest S, Stys PK, Yong VW. Immunosenescence
of microglia and macrophages: impact on the ageing central nervous system. Brain. 2016
Jan 29;139(3):653-61.
3. Zhang J, Rane G, Dai X, Shanmugam MK, Arfuso F, Samy RP, Lai MK, Kappei D,
Kumar AP, Sethi G. Ageing and the telomere connection: An intimate relationship with
inflammation. Ageing research reviews. 2016 Jan 1;25:55-69.
4. Morley JE. Anorexia of ageing: a key component in the pathogenesis of both sarcopenia
and cachexia. Journal of cachexia, sarcopenia and muscle. 2017 Aug;8(4):523-6.
5. Rygiel KA, Picard M, Turnbull DM. The ageing neuromuscular system and sarcopenia: a
mitochondrial perspective. The Journal of physiology. 2016 Aug 15;594(16):4499-512.
6. Pilgrim A, Robinson S, Sayer AA, Roberts H. An overview of appetite decline in older
people. Nursing older people. 2015 Jun;27(5):29.
7. Nifli AP. Appetite, metabolism and hormonal regulation in normal ageing and dementia.
Diseases. 2018 Sep;6(3):66.
8. Peterson G. Aged care: Unintentional weight loss in the elderly. Australian Pharmacist.
2015 Jan;34(1):31.
9. Gallo M. Taste neophobia over the life span. InFood Neophobia 2018 Jan 1 (pp. 25-41).
Woodhead Publishing.
References
1. Hepple RT, Rice CL. Innervation and neuromuscular control in ageing skeletal muscle.
The Journal of physiology. 2016 Apr 15;594(8):1965-78.
2. Rawji KS, Mishra MK, Michaels NJ, Rivest S, Stys PK, Yong VW. Immunosenescence
of microglia and macrophages: impact on the ageing central nervous system. Brain. 2016
Jan 29;139(3):653-61.
3. Zhang J, Rane G, Dai X, Shanmugam MK, Arfuso F, Samy RP, Lai MK, Kappei D,
Kumar AP, Sethi G. Ageing and the telomere connection: An intimate relationship with
inflammation. Ageing research reviews. 2016 Jan 1;25:55-69.
4. Morley JE. Anorexia of ageing: a key component in the pathogenesis of both sarcopenia
and cachexia. Journal of cachexia, sarcopenia and muscle. 2017 Aug;8(4):523-6.
5. Rygiel KA, Picard M, Turnbull DM. The ageing neuromuscular system and sarcopenia: a
mitochondrial perspective. The Journal of physiology. 2016 Aug 15;594(16):4499-512.
6. Pilgrim A, Robinson S, Sayer AA, Roberts H. An overview of appetite decline in older
people. Nursing older people. 2015 Jun;27(5):29.
7. Nifli AP. Appetite, metabolism and hormonal regulation in normal ageing and dementia.
Diseases. 2018 Sep;6(3):66.
8. Peterson G. Aged care: Unintentional weight loss in the elderly. Australian Pharmacist.
2015 Jan;34(1):31.
9. Gallo M. Taste neophobia over the life span. InFood Neophobia 2018 Jan 1 (pp. 25-41).
Woodhead Publishing.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10LIFESPAN NUTRITION FOR THE ELDERY
10. Body JJ, Terpos E, Tombal B, Hadji P, Arif A, Young A, Aapro M, Coleman R. Bone
health in the elderly cancer patient: a SIOG position paper. Cancer treatment reviews.
2016 Dec 1;51:46-53.
11. Lee JH, Lee YK, Oh SH, Ahn J, Lee YE, Pyo JH, Choi YY, Kim D, Bae SC, Sung YK,
Kim DY. A systematic review of diagnostic accuracy of vertebral fracture assessment
(VFA) in postmenopausal women and elderly men. Osteoporosis International. 2016 May
1;27(5):1691-9.
12. National Health and Medical Research Council. Nutrients | Nutrient Reference Values
[Internet]. Nrv.gov.au. 2019 [cited 27 September 2019]. Available from:
https://www.nrv.gov.au/nutrients.
13. Nutrition Australia. Australian Dietary Guidelines: Recommended daily intakes |
Nutrition Australia [Internet]. Nutritionaustralia.org. 2019 [cited 27 September 2019].
Available from: http://www.nutritionaustralia.org/national/resource/australian-dietary-
guidelines-recommended-daily-intakes.
14. Eshkoor S, Hamid T, Shahar S, Ng C, Mun C. Factors affecting hypertension among the
Malaysian elderly. Journal of cardiovascular development and disease. 2016 Mar;3(1):8.
15. Pinto IC, Martins D. Prevalence and risk factors of arterial hypertension: A literature
review. Journal of Cardiovascular Medicine and Therapeutics. 2017;1(2):1-7.
16. Vermeulen E, Stronks K, Snijder MB, Schene AH, Lok A, De Vries JH, Visser M,
Brouwer IA, Nicolaou M. A combined high-sugar and high-saturated-fat dietary pattern
is associated with more depressive symptoms in a multi-ethnic population: The helius
(healthy life in an urban setting) study. Public health nutrition. 2017 Sep;20(13):2374-82.
10. Body JJ, Terpos E, Tombal B, Hadji P, Arif A, Young A, Aapro M, Coleman R. Bone
health in the elderly cancer patient: a SIOG position paper. Cancer treatment reviews.
2016 Dec 1;51:46-53.
11. Lee JH, Lee YK, Oh SH, Ahn J, Lee YE, Pyo JH, Choi YY, Kim D, Bae SC, Sung YK,
Kim DY. A systematic review of diagnostic accuracy of vertebral fracture assessment
(VFA) in postmenopausal women and elderly men. Osteoporosis International. 2016 May
1;27(5):1691-9.
12. National Health and Medical Research Council. Nutrients | Nutrient Reference Values
[Internet]. Nrv.gov.au. 2019 [cited 27 September 2019]. Available from:
https://www.nrv.gov.au/nutrients.
13. Nutrition Australia. Australian Dietary Guidelines: Recommended daily intakes |
Nutrition Australia [Internet]. Nutritionaustralia.org. 2019 [cited 27 September 2019].
Available from: http://www.nutritionaustralia.org/national/resource/australian-dietary-
guidelines-recommended-daily-intakes.
14. Eshkoor S, Hamid T, Shahar S, Ng C, Mun C. Factors affecting hypertension among the
Malaysian elderly. Journal of cardiovascular development and disease. 2016 Mar;3(1):8.
15. Pinto IC, Martins D. Prevalence and risk factors of arterial hypertension: A literature
review. Journal of Cardiovascular Medicine and Therapeutics. 2017;1(2):1-7.
16. Vermeulen E, Stronks K, Snijder MB, Schene AH, Lok A, De Vries JH, Visser M,
Brouwer IA, Nicolaou M. A combined high-sugar and high-saturated-fat dietary pattern
is associated with more depressive symptoms in a multi-ethnic population: The helius
(healthy life in an urban setting) study. Public health nutrition. 2017 Sep;20(13):2374-82.
11LIFESPAN NUTRITION FOR THE ELDERY
17. Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, Thompson PL,
Lewis JR. Dietary saturated fat intake and atherosclerotic vascular disease mortality in
elderly women: a prospective cohort study. The American journal of clinical nutrition.
2015 Jun 1;101(6):1263-8.
18. Fard NR, Karimi M, Baghaei MH, Haghighatdoost F, Rouhani MH, Esmaillzadeh A,
Azadbakht L. Dairy consumption, cardiovascular risk factors and inflammation in elderly
subjects. ARYA atherosclerosis. 2015 Nov;11(6):323.
19. Pinto ES, Castro CC, Campos ID, Teles JB, Mendes CM. Self-reported Hydration in
Diabetic and Hypertensive Elderly. J Community Med Health Educ. 2017;7(544):2161-
0711.
20. Zujko ME, Witkowska AM, Waśkiewicz A, Mirończuk-Chodakowska I. Dietary
antioxidant and flavonoid intakes are reduced in the elderly. Oxidative medicine and
cellular longevity. 2015;2015.
21. Jagielak D, Wernio E, Kozaryn R, Bramlage P, Gruchała-Niedoszytko M, Rogowski J,
Małgorzewicz S. The impact of nutritional status and appetite on the hospital length of
stay and postoperative complications in elderly patients with severe aortic stenosis before
aortic valve replacement. Kardiochirurgia i torakochirurgia polska= Polish journal of
cardio-thoracic surgery. 2016 Jun;13(2):105.
22. Pilgrim AL, Baylis D, Jameson KA, Cooper C, Sayer AA, Robinson SM, Roberts HC.
Measuring appetite with the simplified nutritional appetite questionnaire identifies
hospitalised older people at risk of worse health outcomes. The journal of nutrition,
health & aging. 2016 Jan 1;20(1):3-7.
17. Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, Thompson PL,
Lewis JR. Dietary saturated fat intake and atherosclerotic vascular disease mortality in
elderly women: a prospective cohort study. The American journal of clinical nutrition.
2015 Jun 1;101(6):1263-8.
18. Fard NR, Karimi M, Baghaei MH, Haghighatdoost F, Rouhani MH, Esmaillzadeh A,
Azadbakht L. Dairy consumption, cardiovascular risk factors and inflammation in elderly
subjects. ARYA atherosclerosis. 2015 Nov;11(6):323.
19. Pinto ES, Castro CC, Campos ID, Teles JB, Mendes CM. Self-reported Hydration in
Diabetic and Hypertensive Elderly. J Community Med Health Educ. 2017;7(544):2161-
0711.
20. Zujko ME, Witkowska AM, Waśkiewicz A, Mirończuk-Chodakowska I. Dietary
antioxidant and flavonoid intakes are reduced in the elderly. Oxidative medicine and
cellular longevity. 2015;2015.
21. Jagielak D, Wernio E, Kozaryn R, Bramlage P, Gruchała-Niedoszytko M, Rogowski J,
Małgorzewicz S. The impact of nutritional status and appetite on the hospital length of
stay and postoperative complications in elderly patients with severe aortic stenosis before
aortic valve replacement. Kardiochirurgia i torakochirurgia polska= Polish journal of
cardio-thoracic surgery. 2016 Jun;13(2):105.
22. Pilgrim AL, Baylis D, Jameson KA, Cooper C, Sayer AA, Robinson SM, Roberts HC.
Measuring appetite with the simplified nutritional appetite questionnaire identifies
hospitalised older people at risk of worse health outcomes. The journal of nutrition,
health & aging. 2016 Jan 1;20(1):3-7.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.