Deakin University HSN702 Lifespan Nutrition Case Study and Analysis
VerifiedAdded on 2023/03/31
|13
|2955
|494
Case Study
AI Summary
This assignment presents a detailed case study and nutritional analysis focusing on an elderly patient, Agnes, with hypertension and a risk of osteoporosis. The analysis begins with a discussion of physiological changes in the elderly, including sarcopenia, bone mineral density loss, and increased inflammation, which necessitate specific nutritional considerations. The assignment then examines Agnes's dietary intake, comparing it to recommended nutrient reference values and Australian Dietary Guidelines. The analysis reveals deficiencies in water intake, excessive sodium and saturated fat consumption, and inadequate calcium and energy intake, contributing to her health concerns. The assignment further explores assessment strategies beyond dietary recall, such as interviews and blood tests. Finally, the assignment proposes practical strategies to improve Agnes's dietary intake, including educational resources, texture modifications, and food substitutions to address her specific nutritional needs and health risks, such as reducing saturated fat intake and increasing calcium and water consumption. The assignment also includes a review of the patient's food intake and suggests modifications based on the findings.

Running head: CASE STUDY AND NUTRITIONAL ANALYSIS
CASE STUDY AND NUTRITIONAL ANALYSIS
Name of the Student:
Name of the University:
Author note:
CASE STUDY AND NUTRITIONAL ANALYSIS
Name of the Student:
Name of the University:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CASE STUDY AND NUTRITIONAL ANALYSIS
Part A
Section 1
Musculoskeletal changes in the elderly is associated with muscle mass loss and
catabolism, known as sarcopenia – which necessitates the need for the elderly to consider
increasing their nutritional intake of good quality sources of proteins to counter such losses [1].
An additional physiological change associated with the elderly includes decrease of bone mineral
density and mass resulting in increased bone loss and porosity. Hence, such age-related
conditions in the elderly results in an increased nutritional need to enhance dietary intake of
calcium and vitamin D in their diets [2].
With age, the rate of inflammatory mechanisms and free radical formation increases
across the elderly further causes damage and loss of neurons in the brain and the nervous system,
which increases their risk of acquiring neuro-cognitive diseases like dementia and Alzheimer’s.
The high rates of inflammation are also associated with high accumulation of harmful advanced
glycation end products (AGEs) which have been known to cause damage to the immune system
and tissues of the elderly [3]. Thus, such physiological changes within the elderly increase their
susceptibility to acquire long term infectious and chronic diseases which calls for the need for
old age individuals to consume a diet rich in antioxidants and protective factors like minerals and
vitamins [4].
Section 2
Old age also increases the risk of facing difficulties in consuming required nutrients. As a
person ages, he or she frequently encounters digestive problems like indigestion, loose stools,
Part A
Section 1
Musculoskeletal changes in the elderly is associated with muscle mass loss and
catabolism, known as sarcopenia – which necessitates the need for the elderly to consider
increasing their nutritional intake of good quality sources of proteins to counter such losses [1].
An additional physiological change associated with the elderly includes decrease of bone mineral
density and mass resulting in increased bone loss and porosity. Hence, such age-related
conditions in the elderly results in an increased nutritional need to enhance dietary intake of
calcium and vitamin D in their diets [2].
With age, the rate of inflammatory mechanisms and free radical formation increases
across the elderly further causes damage and loss of neurons in the brain and the nervous system,
which increases their risk of acquiring neuro-cognitive diseases like dementia and Alzheimer’s.
The high rates of inflammation are also associated with high accumulation of harmful advanced
glycation end products (AGEs) which have been known to cause damage to the immune system
and tissues of the elderly [3]. Thus, such physiological changes within the elderly increase their
susceptibility to acquire long term infectious and chronic diseases which calls for the need for
old age individuals to consume a diet rich in antioxidants and protective factors like minerals and
vitamins [4].
Section 2
Old age also increases the risk of facing difficulties in consuming required nutrients. As a
person ages, he or she frequently encounters digestive problems like indigestion, loose stools,
2CASE STUDY AND NUTRITIONAL ANALYSIS
bloating and heartburn after consuming foods which were previously tolerable [5]. This is due to
the fact that old age results in a reduced secretion of gastric acid by the stomach and hence, also
affects appetite and the ability of ageing body to obtain and absorb required nutrients from food.
Thus, the aged care facility must keep this nutritional concern in mind and prepare foods which
are appealing, easily digestible and nutritious for the residents [6].
Old age results in simultaneous nerve damage, which leads to an increased sensitivity or
lack of it, towards the taste and smell of food across the elderly. Further, older age often leads to
physiological changes like loss of teeth and decreased salivary secretion. All these sensory and
oral changes thus make it difficult for the elderly to chew or swallow food and thus consume
adequate amount of nutrients required by the body [7]. The loss of appetite, sensory alterations
and loss of muscle - all contribute to poor nutritional status and concerns of malnutrition in the
elderly. It is thus advisable that the aged care facility provided foods which have modified or
softened in terms of texture so as to ensure optimum food intake and malnutrition prevention
across its residents [8].
Section 3
Osteoporosis across the elderly is caused due to a number of factors, mainly: reduced
strength or frailty, low anthropometric measurements, consumption of a diet deficient in vitamin
D and calcium and inadequate levels of calcium, phosphorous and vitamin D in the serum [9].
Thus, considering the above, a major anthropometric risk factors of osteoporosis is a status of
underweight, frailty or low body mass index. In case of biochemical parameters, low serum
levels of calcium, vitamin D and phosphorus are major risks factors underlying osteoporosis
[10]. Prevalent clinical risk factors indicative of this condition include a low bone density of 2.5
standard deviation or less as per average bone density values. Lastly, a diet does not comprise
bloating and heartburn after consuming foods which were previously tolerable [5]. This is due to
the fact that old age results in a reduced secretion of gastric acid by the stomach and hence, also
affects appetite and the ability of ageing body to obtain and absorb required nutrients from food.
Thus, the aged care facility must keep this nutritional concern in mind and prepare foods which
are appealing, easily digestible and nutritious for the residents [6].
Old age results in simultaneous nerve damage, which leads to an increased sensitivity or
lack of it, towards the taste and smell of food across the elderly. Further, older age often leads to
physiological changes like loss of teeth and decreased salivary secretion. All these sensory and
oral changes thus make it difficult for the elderly to chew or swallow food and thus consume
adequate amount of nutrients required by the body [7]. The loss of appetite, sensory alterations
and loss of muscle - all contribute to poor nutritional status and concerns of malnutrition in the
elderly. It is thus advisable that the aged care facility provided foods which have modified or
softened in terms of texture so as to ensure optimum food intake and malnutrition prevention
across its residents [8].
Section 3
Osteoporosis across the elderly is caused due to a number of factors, mainly: reduced
strength or frailty, low anthropometric measurements, consumption of a diet deficient in vitamin
D and calcium and inadequate levels of calcium, phosphorous and vitamin D in the serum [9].
Thus, considering the above, a major anthropometric risk factors of osteoporosis is a status of
underweight, frailty or low body mass index. In case of biochemical parameters, low serum
levels of calcium, vitamin D and phosphorus are major risks factors underlying osteoporosis
[10]. Prevalent clinical risk factors indicative of this condition include a low bone density of 2.5
standard deviation or less as per average bone density values. Lastly, a diet does not comprise
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CASE STUDY AND NUTRITIONAL ANALYSIS
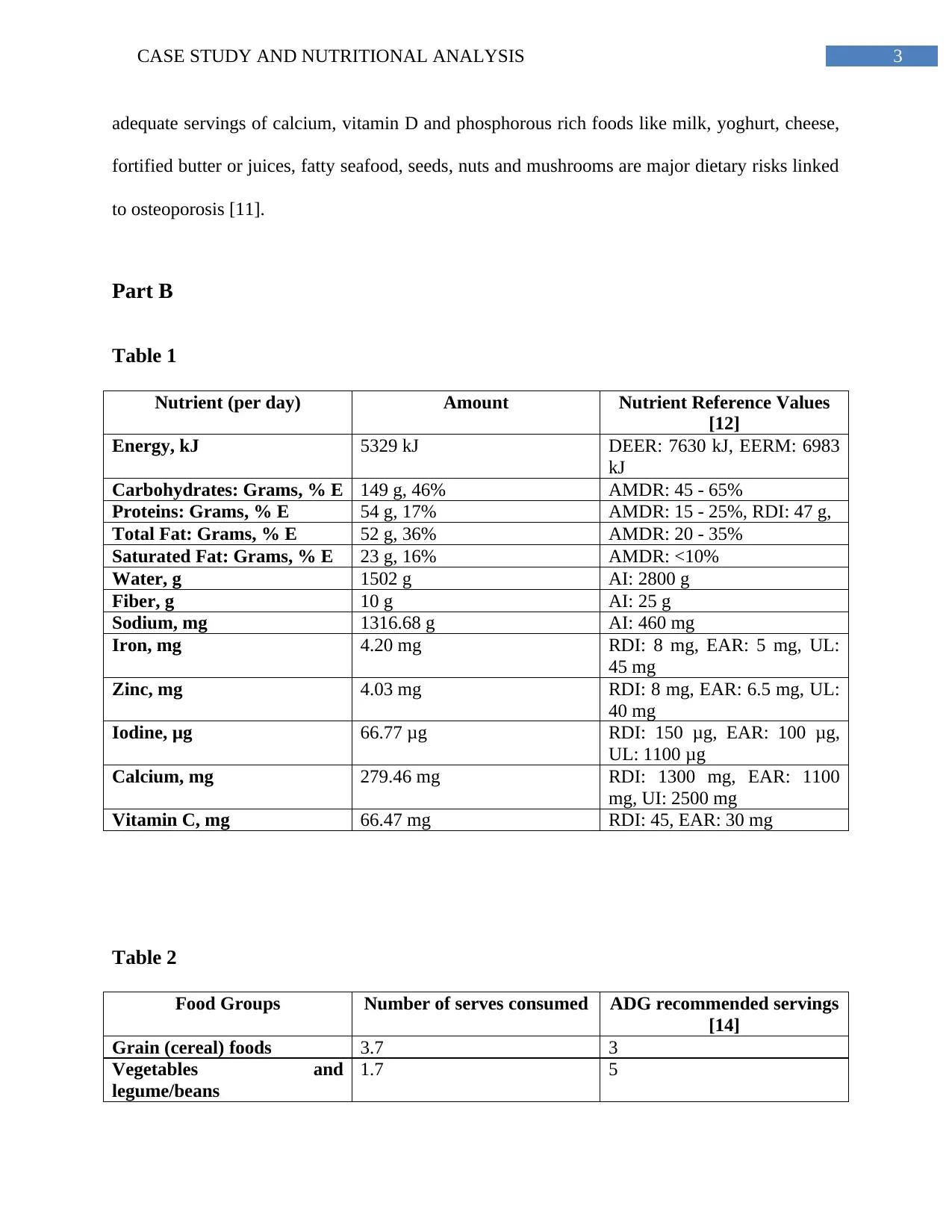
adequate servings of calcium, vitamin D and phosphorous rich foods like milk, yoghurt, cheese,
fortified butter or juices, fatty seafood, seeds, nuts and mushrooms are major dietary risks linked
to osteoporosis [11].
Part B
Table 1
Nutrient (per day) Amount Nutrient Reference Values
[12]
Energy, kJ 5329 kJ DEER: 7630 kJ, EERM: 6983
kJ
Carbohydrates: Grams, % E 149 g, 46% AMDR: 45 - 65%
Proteins: Grams, % E 54 g, 17% AMDR: 15 - 25%, RDI: 47 g,
Total Fat: Grams, % E 52 g, 36% AMDR: 20 - 35%
Saturated Fat: Grams, % E 23 g, 16% AMDR: <10%
Water, g 1502 g AI: 2800 g
Fiber, g 10 g AI: 25 g
Sodium, mg 1316.68 g AI: 460 mg
Iron, mg 4.20 mg RDI: 8 mg, EAR: 5 mg, UL:
45 mg
Zinc, mg 4.03 mg RDI: 8 mg, EAR: 6.5 mg, UL:
40 mg
Iodine, μg 66.77 μg RDI: 150 μg, EAR: 100 μg,
UL: 1100 μg
Calcium, mg 279.46 mg RDI: 1300 mg, EAR: 1100
mg, UI: 2500 mg
Vitamin C, mg 66.47 mg RDI: 45, EAR: 30 mg
Table 2
Food Groups Number of serves consumed ADG recommended servings
[14]
Grain (cereal) foods 3.7 3
Vegetables and
legume/beans
1.7 5
adequate servings of calcium, vitamin D and phosphorous rich foods like milk, yoghurt, cheese,
fortified butter or juices, fatty seafood, seeds, nuts and mushrooms are major dietary risks linked
to osteoporosis [11].
Part B
Table 1
Nutrient (per day) Amount Nutrient Reference Values
[12]
Energy, kJ 5329 kJ DEER: 7630 kJ, EERM: 6983
kJ
Carbohydrates: Grams, % E 149 g, 46% AMDR: 45 - 65%
Proteins: Grams, % E 54 g, 17% AMDR: 15 - 25%, RDI: 47 g,
Total Fat: Grams, % E 52 g, 36% AMDR: 20 - 35%
Saturated Fat: Grams, % E 23 g, 16% AMDR: <10%
Water, g 1502 g AI: 2800 g
Fiber, g 10 g AI: 25 g
Sodium, mg 1316.68 g AI: 460 mg
Iron, mg 4.20 mg RDI: 8 mg, EAR: 5 mg, UL:
45 mg
Zinc, mg 4.03 mg RDI: 8 mg, EAR: 6.5 mg, UL:
40 mg
Iodine, μg 66.77 μg RDI: 150 μg, EAR: 100 μg,
UL: 1100 μg
Calcium, mg 279.46 mg RDI: 1300 mg, EAR: 1100
mg, UI: 2500 mg
Vitamin C, mg 66.47 mg RDI: 45, EAR: 30 mg
Table 2
Food Groups Number of serves consumed ADG recommended servings
[14]
Grain (cereal) foods 3.7 3
Vegetables and
legume/beans
1.7 5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CASE STUDY AND NUTRITIONAL ANALYSIS
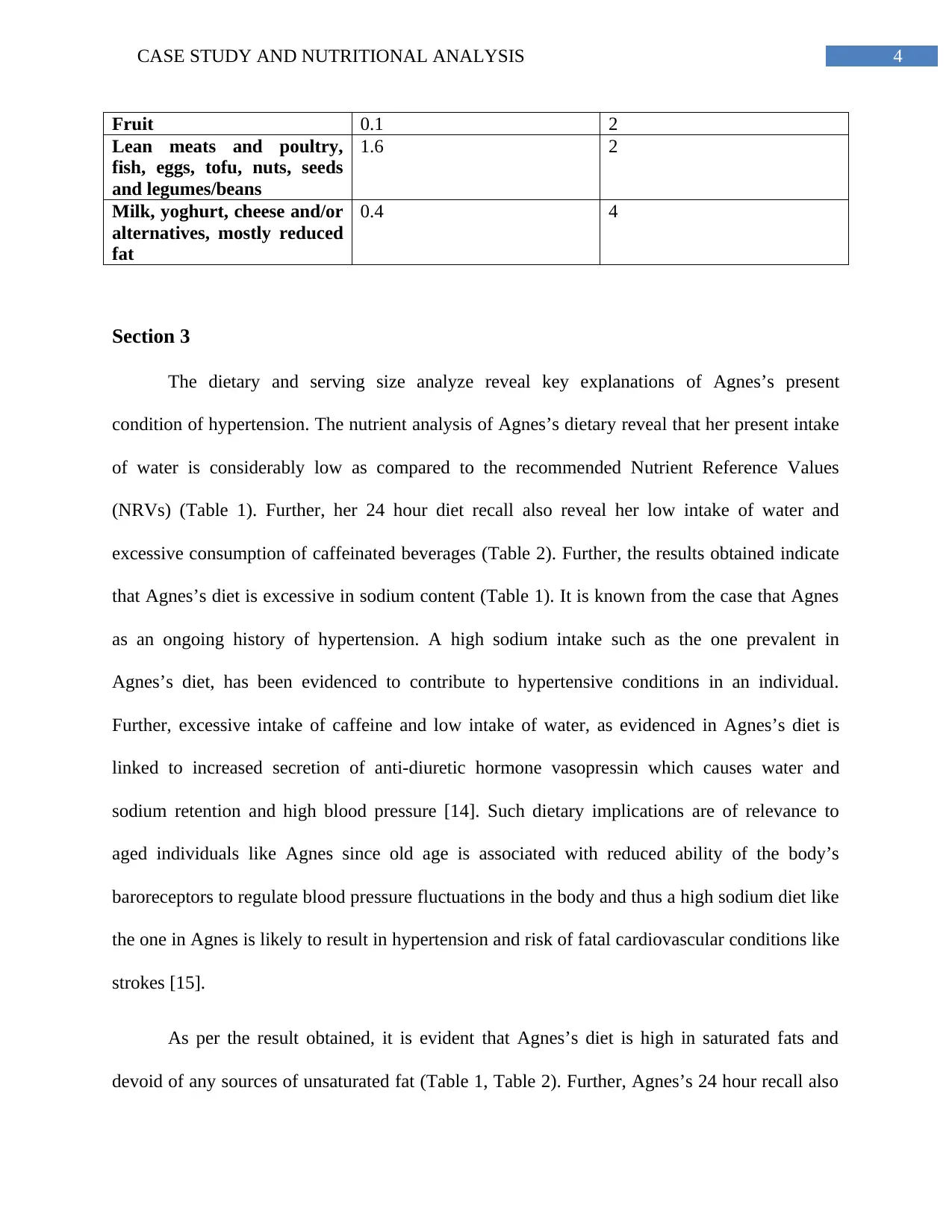
Fruit 0.1 2
Lean meats and poultry,
fish, eggs, tofu, nuts, seeds
and legumes/beans
1.6 2
Milk, yoghurt, cheese and/or
alternatives, mostly reduced
fat
0.4 4
Section 3
The dietary and serving size analyze reveal key explanations of Agnes’s present
condition of hypertension. The nutrient analysis of Agnes’s dietary reveal that her present intake
of water is considerably low as compared to the recommended Nutrient Reference Values
(NRVs) (Table 1). Further, her 24 hour diet recall also reveal her low intake of water and
excessive consumption of caffeinated beverages (Table 2). Further, the results obtained indicate
that Agnes’s diet is excessive in sodium content (Table 1). It is known from the case that Agnes
as an ongoing history of hypertension. A high sodium intake such as the one prevalent in
Agnes’s diet, has been evidenced to contribute to hypertensive conditions in an individual.
Further, excessive intake of caffeine and low intake of water, as evidenced in Agnes’s diet is
linked to increased secretion of anti-diuretic hormone vasopressin which causes water and
sodium retention and high blood pressure [14]. Such dietary implications are of relevance to
aged individuals like Agnes since old age is associated with reduced ability of the body’s
baroreceptors to regulate blood pressure fluctuations in the body and thus a high sodium diet like
the one in Agnes is likely to result in hypertension and risk of fatal cardiovascular conditions like
strokes [15].
As per the result obtained, it is evident that Agnes’s diet is high in saturated fats and
devoid of any sources of unsaturated fat (Table 1, Table 2). Further, Agnes’s 24 hour recall also
Fruit 0.1 2
Lean meats and poultry,
fish, eggs, tofu, nuts, seeds
and legumes/beans
1.6 2
Milk, yoghurt, cheese and/or
alternatives, mostly reduced
fat
0.4 4
Section 3
The dietary and serving size analyze reveal key explanations of Agnes’s present
condition of hypertension. The nutrient analysis of Agnes’s dietary reveal that her present intake
of water is considerably low as compared to the recommended Nutrient Reference Values
(NRVs) (Table 1). Further, her 24 hour diet recall also reveal her low intake of water and
excessive consumption of caffeinated beverages (Table 2). Further, the results obtained indicate
that Agnes’s diet is excessive in sodium content (Table 1). It is known from the case that Agnes
as an ongoing history of hypertension. A high sodium intake such as the one prevalent in
Agnes’s diet, has been evidenced to contribute to hypertensive conditions in an individual.
Further, excessive intake of caffeine and low intake of water, as evidenced in Agnes’s diet is
linked to increased secretion of anti-diuretic hormone vasopressin which causes water and
sodium retention and high blood pressure [14]. Such dietary implications are of relevance to
aged individuals like Agnes since old age is associated with reduced ability of the body’s
baroreceptors to regulate blood pressure fluctuations in the body and thus a high sodium diet like
the one in Agnes is likely to result in hypertension and risk of fatal cardiovascular conditions like
strokes [15].
As per the result obtained, it is evident that Agnes’s diet is high in saturated fats and
devoid of any sources of unsaturated fat (Table 1, Table 2). Further, Agnes’s 24 hour recall also
5CASE STUDY AND NUTRITIONAL ANALYSIS
reveals a high consumption of sugary foods like juices and marmalades and saturated fat sources
like butter, pork, mayo and ham. It has been researched that a diet which is rich in saturated fat
sources and low in essential unsaturated or ‘healthy fats’ result in high cholesterol and a risk of
cardiovascular diseases – which must be corrected in Agnes [16]. Further, calories from
excessive sugar consumption - like the diet in Agnes – is linked to fat conversion and
cholesterol and may be aggravated in the elderly like Agnes due to low rates of metabolism due
to ageing. It is thus expected that the ages care facility address both concerns of hypertension and
high cholesterol in Agnes to their link to cardiovascular diseases [17].
Finally, the dietary analysis reveals low consumption of energy, dairy and calcium in
Agnes’s diet which increases her risk of osteoporosis (Table 1, Table 2). We know that Agnes’s
body mass index (BMI) is in the underweight range. This can be linked to her age-associated loss
of muscle and bone and her low intake of calorie rich carbohydrate foods like whole grains,
cereals and legumes (Table 1, Table 2) [18]. Such anthropometric measurements and dietary
inadequacies are major contributors of malnutrition and risk factors of osteoporosis which must
be corrected immediately in Agnes. Further her food servings indicate an absence of foods rich
in calcium and micronutrients like dairy, fruits and green leafy vegetables – a dietary risk factor
of osteoporosis and vitamin, mineral deficiencies, which the aged care facility must correct
immediately [19].
Section 4
Apart from the above tabulated values of diet and food serving consumption, the aged
care facility or the concerned healthcare professional can also revert to other assessment
strategies to understand the reasons influence her inadequate food consumption. Old age, as
discussed previously, is common linked to low levels of appetite. Thus, a face-to-face interview
reveals a high consumption of sugary foods like juices and marmalades and saturated fat sources
like butter, pork, mayo and ham. It has been researched that a diet which is rich in saturated fat
sources and low in essential unsaturated or ‘healthy fats’ result in high cholesterol and a risk of
cardiovascular diseases – which must be corrected in Agnes [16]. Further, calories from
excessive sugar consumption - like the diet in Agnes – is linked to fat conversion and
cholesterol and may be aggravated in the elderly like Agnes due to low rates of metabolism due
to ageing. It is thus expected that the ages care facility address both concerns of hypertension and
high cholesterol in Agnes to their link to cardiovascular diseases [17].
Finally, the dietary analysis reveals low consumption of energy, dairy and calcium in
Agnes’s diet which increases her risk of osteoporosis (Table 1, Table 2). We know that Agnes’s
body mass index (BMI) is in the underweight range. This can be linked to her age-associated loss
of muscle and bone and her low intake of calorie rich carbohydrate foods like whole grains,
cereals and legumes (Table 1, Table 2) [18]. Such anthropometric measurements and dietary
inadequacies are major contributors of malnutrition and risk factors of osteoporosis which must
be corrected immediately in Agnes. Further her food servings indicate an absence of foods rich
in calcium and micronutrients like dairy, fruits and green leafy vegetables – a dietary risk factor
of osteoporosis and vitamin, mineral deficiencies, which the aged care facility must correct
immediately [19].
Section 4
Apart from the above tabulated values of diet and food serving consumption, the aged
care facility or the concerned healthcare professional can also revert to other assessment
strategies to understand the reasons influence her inadequate food consumption. Old age, as
discussed previously, is common linked to low levels of appetite. Thus, a face-to-face interview
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CASE STUDY AND NUTRITIONAL ANALYSIS
can be conducted with Agnes where aged facility works can understand the subjective reasons
contributing to her low food intake [20]. Such an interview can be done with a 10 part
questionnaire known as the ‘Bratman Test for Orthorexia’ - a common tool which assess
‘orthorexia’ or appetite losses in individuals and assists in finding out whether this loss occurs
due to decreased self-esteem or quality of health and wellbeing [21].
Often inadequate dietary intake due to appetite loss is observed in the elderly suffering
tom chronic diseases like cystic fibrosis, chronic obstructive pulmonary disorder, cancer, heart
failure and chronic kidney diseases. Thus, to observe whether Agnes’s loss of appetite is to due
to such conditions, health workers can conduct screening or blood tests relevant to organ systems
like the heart, respiration, liver or kidneys [22].
The Australian Dietary Guidelines (ADGs) have laid guideline for the recommended
servings of core foods groups which the elderly must adhere to [13]. Additionally, the Dietitians
Association of Australia (DAA) has also laid standards on requirements to be maintained in
terms of texture modification of foods [23]. Not only do the elderly need a diet a nutritionally
balanced diet as per the ADGs, they also need foods modified as per their ingestion needs to
ensure appetite and acceptability. Thus the menu provided with the aged care facility can be
compared with the ADGs as well as DAA specifications to assess compliance with nutritional
and texture requirements of the elderly. This can help in understanding the reasons underlying
Agnes’s nutritional concerns and inadequate intake [24].
Section 5
For improving dietary intake across elderly individuals like Agnes, the following
strategies can be considered:
can be conducted with Agnes where aged facility works can understand the subjective reasons
contributing to her low food intake [20]. Such an interview can be done with a 10 part
questionnaire known as the ‘Bratman Test for Orthorexia’ - a common tool which assess
‘orthorexia’ or appetite losses in individuals and assists in finding out whether this loss occurs
due to decreased self-esteem or quality of health and wellbeing [21].
Often inadequate dietary intake due to appetite loss is observed in the elderly suffering
tom chronic diseases like cystic fibrosis, chronic obstructive pulmonary disorder, cancer, heart
failure and chronic kidney diseases. Thus, to observe whether Agnes’s loss of appetite is to due
to such conditions, health workers can conduct screening or blood tests relevant to organ systems
like the heart, respiration, liver or kidneys [22].
The Australian Dietary Guidelines (ADGs) have laid guideline for the recommended
servings of core foods groups which the elderly must adhere to [13]. Additionally, the Dietitians
Association of Australia (DAA) has also laid standards on requirements to be maintained in
terms of texture modification of foods [23]. Not only do the elderly need a diet a nutritionally
balanced diet as per the ADGs, they also need foods modified as per their ingestion needs to
ensure appetite and acceptability. Thus the menu provided with the aged care facility can be
compared with the ADGs as well as DAA specifications to assess compliance with nutritional
and texture requirements of the elderly. This can help in understanding the reasons underlying
Agnes’s nutritional concerns and inadequate intake [24].
Section 5
For improving dietary intake across elderly individuals like Agnes, the following
strategies can be considered:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CASE STUDY AND NUTRITIONAL ANALYSIS
1. Families visiting the aged care facility can be educated on the foods they must avoid or
bring considering the health conditions and nutritional needs of the elderly. This can be
done by distributing educational resources containing information on core food groups
whose consumption is to be encouraged across the elderly [25].
2. A similar educational session can also be conducted across the elderly patients as well as
the workers preparing food within the aged care facility on the importance of consuming
adequate water and a balanced diet and the need to prepare textually modified foods
compliant to the ADG and DAA specifications [26].
3. Taking insights from Agnes’s diet, firm foods like toasts, crackers and vegetables must
be prepared or replaced with soft foods like soft, untoasted breads and steamed
vegetables or a vegetable gruel. This is will ensure adequate intake of fiber and
micronutrients in forms which are easy to chew [27].
4. Sources of red meat like pork and ham as well as saturated fats like butter, mayonnaise
and cheese must be replaced with proteins which are lean and vegetarian in nature (such
as chicken, fish, legumes, soy) cooked in unsaturated sources like olive oils, seeds and
nuts. This will help in reducing the intake of saturated fats and cardiovascular risk along
with increasing the intake of beneficial sources of anti-inflammatory, unsaturated fats like
omega 3 fatty acids [28].
5. To reduce the risk of hypertension in patients like Agnes, it is recommended that
processed, salty foods like crackers as well as caffeine containing foods be replaced with
adequate water intake or with foods prepared in limited salt like, sandwiches, salads or
gruels comprising of colorful vegetables and herbs [29].
1. Families visiting the aged care facility can be educated on the foods they must avoid or
bring considering the health conditions and nutritional needs of the elderly. This can be
done by distributing educational resources containing information on core food groups
whose consumption is to be encouraged across the elderly [25].
2. A similar educational session can also be conducted across the elderly patients as well as
the workers preparing food within the aged care facility on the importance of consuming
adequate water and a balanced diet and the need to prepare textually modified foods
compliant to the ADG and DAA specifications [26].
3. Taking insights from Agnes’s diet, firm foods like toasts, crackers and vegetables must
be prepared or replaced with soft foods like soft, untoasted breads and steamed
vegetables or a vegetable gruel. This is will ensure adequate intake of fiber and
micronutrients in forms which are easy to chew [27].
4. Sources of red meat like pork and ham as well as saturated fats like butter, mayonnaise
and cheese must be replaced with proteins which are lean and vegetarian in nature (such
as chicken, fish, legumes, soy) cooked in unsaturated sources like olive oils, seeds and
nuts. This will help in reducing the intake of saturated fats and cardiovascular risk along
with increasing the intake of beneficial sources of anti-inflammatory, unsaturated fats like
omega 3 fatty acids [28].
5. To reduce the risk of hypertension in patients like Agnes, it is recommended that
processed, salty foods like crackers as well as caffeine containing foods be replaced with
adequate water intake or with foods prepared in limited salt like, sandwiches, salads or
gruels comprising of colorful vegetables and herbs [29].
8CASE STUDY AND NUTRITIONAL ANALYSIS
6. To correct the risk of hypercholesterolemia and high sugar intake, the aged care facility
must ensure to replace sugary sources like marmalades, added sugar in coffee and
processed juices with stewed or boiled fruits, freshly prepared juices made without added
sugar and green tea or coffee comprising of limited sugar.
7. Finally, to prevent the risk of osteoporosis and improve her calcium intake without
increasing saturated fat consumption, the aged care facility must consider replacing
whole milk sources from Agnes or other elderly patients’ diets with low fat forms of
milk, yoghurt, cheese, soy or low fat milk based beverages.
6. To correct the risk of hypercholesterolemia and high sugar intake, the aged care facility
must ensure to replace sugary sources like marmalades, added sugar in coffee and
processed juices with stewed or boiled fruits, freshly prepared juices made without added
sugar and green tea or coffee comprising of limited sugar.
7. Finally, to prevent the risk of osteoporosis and improve her calcium intake without
increasing saturated fat consumption, the aged care facility must consider replacing
whole milk sources from Agnes or other elderly patients’ diets with low fat forms of
milk, yoghurt, cheese, soy or low fat milk based beverages.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CASE STUDY AND NUTRITIONAL ANALYSIS
References
1. Rong YD, Bian AL, Hu HY, Ma Y, Zhou XZ. Study on relationship between elderly
sarcopenia and inflammatory cytokine IL-6, anti-inflammatory cytokine IL-10. BMC
geriatrics. 2018 Dec;18(1):308.
2. Fukuda Y, Yamamoto K, Hirao M, Nishikawa K, Nagatsuma Y, Nakayama T, Tanikawa
S, Maeda S, Uemura M, Miyake M, Hama N. Sarcopenia is associated with severe
postoperative complications in elderly gastric cancer patients undergoing gastrectomy.
Gastric Cancer. 2016 Jul 1;19(3):986-93.
3. Zhang J, Rane G, Dai X, Shanmugam MK, Arfuso F, Samy RP, Lai MK, Kappei D,
Kumar AP, Sethi G. Ageing and the telomere connection: An intimate relationship with
inflammation. Ageing research reviews. 2016 Jan 1;25:55-69.
4. Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular
disease, and frailty. Nature Reviews Cardiology. 2018 Sep;15(9):505.
5. Soenen S, Rayner CK, Jones KL, Horowitz M. The ageing gastrointestinal tract. Current
Opinion in Clinical Nutrition & Metabolic Care. 2016 Jan 1;19(1):12-8.
6. Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. The effect of emotional stress and
depression on the prevalence of digestive diseases. Journal of neurogastroenterology and
motility. 2015 Apr;21(2):273.
7. Rath AA. Clinical concerns of oral health in old age: an Indian perspective. JGCR.
2017;4(1):17.
8. Ogawa T, Annear MJ, Ikebe K, Maeda Y. Taste‐related sensations in old age. Journal of
oral rehabilitation. 2017 Aug;44(8):626-35.
References
1. Rong YD, Bian AL, Hu HY, Ma Y, Zhou XZ. Study on relationship between elderly
sarcopenia and inflammatory cytokine IL-6, anti-inflammatory cytokine IL-10. BMC
geriatrics. 2018 Dec;18(1):308.
2. Fukuda Y, Yamamoto K, Hirao M, Nishikawa K, Nagatsuma Y, Nakayama T, Tanikawa
S, Maeda S, Uemura M, Miyake M, Hama N. Sarcopenia is associated with severe
postoperative complications in elderly gastric cancer patients undergoing gastrectomy.
Gastric Cancer. 2016 Jul 1;19(3):986-93.
3. Zhang J, Rane G, Dai X, Shanmugam MK, Arfuso F, Samy RP, Lai MK, Kappei D,
Kumar AP, Sethi G. Ageing and the telomere connection: An intimate relationship with
inflammation. Ageing research reviews. 2016 Jan 1;25:55-69.
4. Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular
disease, and frailty. Nature Reviews Cardiology. 2018 Sep;15(9):505.
5. Soenen S, Rayner CK, Jones KL, Horowitz M. The ageing gastrointestinal tract. Current
Opinion in Clinical Nutrition & Metabolic Care. 2016 Jan 1;19(1):12-8.
6. Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. The effect of emotional stress and
depression on the prevalence of digestive diseases. Journal of neurogastroenterology and
motility. 2015 Apr;21(2):273.
7. Rath AA. Clinical concerns of oral health in old age: an Indian perspective. JGCR.
2017;4(1):17.
8. Ogawa T, Annear MJ, Ikebe K, Maeda Y. Taste‐related sensations in old age. Journal of
oral rehabilitation. 2017 Aug;44(8):626-35.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10CASE STUDY AND NUTRITIONAL ANALYSIS
9. Li G, Thabane L, Papaioannou A, Ioannidis G, Levine MA, Adachi JD. An overview of
osteoporosis and frailty in the elderly. BMC musculoskeletal disorders. 2017
Dec;18(1):46.
10. Klop C, Welsing PM, Leufkens HG, Elders PJ, Overbeek JA, van den Bergh JP, Bijlsma
JW, de Vries F. The epidemiology of hip and major osteoporotic fractures in a Dutch
population of community-dwelling elderly: implications for the Dutch FRAX®
algorithm. PloS one. 2015 Dec 3;10(12):e0143800.
11. Popp AW, Meer S, Krieg MA, Perrelet R, Hans D, Lippuner K. Bone mineral density
(BMD) and vertebral trabecular bone score (TBS) for the identification of elderly women
at high risk for fracture: the SEMOF cohort study. European spine journal. 2016 Nov
1;25(11):3432-8.
12. National Health and Medical Research Council. Nutrients | Nutrient Reference Values
[Internet]. Nrv.gov.au. 2019 [cited 25 September 2019]. Available from:
https://www.nrv.gov.au/nutrients.
13. Nutrition Australia. Australian Dietary Guidelines: Recommended daily intakes |
Nutrition Australia [Internet]. Nutritionaustralia.org. 2019 [cited 25 September 2019].
Available from: http://www.nutritionaustralia.org/national/resource/australian-dietary-
guidelines-recommended-daily-intakes.
14. Abdelhafiz AH, Marshall R, Kavanagh J, El Nahas M. Hypertension in the Elderly.
InClinical Nephrogeriatrics 2019 (pp. 63-85). Springer, Cham.
15. Imprialos KP, Boutari C, Stavropoulos K, Doumas M, Athyros VG, Karagiannis AI.
Current challenges in antihypertensive treatment in the elderly. Pol Arch Med Wewn.
2016 Aug 25;126(7-8):540-51.
9. Li G, Thabane L, Papaioannou A, Ioannidis G, Levine MA, Adachi JD. An overview of
osteoporosis and frailty in the elderly. BMC musculoskeletal disorders. 2017
Dec;18(1):46.
10. Klop C, Welsing PM, Leufkens HG, Elders PJ, Overbeek JA, van den Bergh JP, Bijlsma
JW, de Vries F. The epidemiology of hip and major osteoporotic fractures in a Dutch
population of community-dwelling elderly: implications for the Dutch FRAX®
algorithm. PloS one. 2015 Dec 3;10(12):e0143800.
11. Popp AW, Meer S, Krieg MA, Perrelet R, Hans D, Lippuner K. Bone mineral density
(BMD) and vertebral trabecular bone score (TBS) for the identification of elderly women
at high risk for fracture: the SEMOF cohort study. European spine journal. 2016 Nov
1;25(11):3432-8.
12. National Health and Medical Research Council. Nutrients | Nutrient Reference Values
[Internet]. Nrv.gov.au. 2019 [cited 25 September 2019]. Available from:
https://www.nrv.gov.au/nutrients.
13. Nutrition Australia. Australian Dietary Guidelines: Recommended daily intakes |
Nutrition Australia [Internet]. Nutritionaustralia.org. 2019 [cited 25 September 2019].
Available from: http://www.nutritionaustralia.org/national/resource/australian-dietary-
guidelines-recommended-daily-intakes.
14. Abdelhafiz AH, Marshall R, Kavanagh J, El Nahas M. Hypertension in the Elderly.
InClinical Nephrogeriatrics 2019 (pp. 63-85). Springer, Cham.
15. Imprialos KP, Boutari C, Stavropoulos K, Doumas M, Athyros VG, Karagiannis AI.
Current challenges in antihypertensive treatment in the elderly. Pol Arch Med Wewn.
2016 Aug 25;126(7-8):540-51.
11CASE STUDY AND NUTRITIONAL ANALYSIS
16. Praagman J, de Jonge EA, Kiefte-de Jong JC, Beulens JW, Sluijs I, Schoufour JD,
Hofman A, van der Schouw YT, Franco OH. Dietary saturated fatty acids and coronary
heart disease risk in a Dutch middle-aged and elderly population. Arteriosclerosis,
thrombosis, and vascular biology. 2016 Sep;36(9):2011-8.
17. Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, Thompson PL,
Lewis JR. Dietary saturated fat intake and atherosclerotic vascular disease mortality in
elderly women: a prospective cohort study. The American journal of clinical nutrition.
2015 Jun 1;101(6):1263-8.
18. Siddique N, O'Donoghue M, Casey MC, Walsh JB. Malnutrition in the elderly and its
effects on bone health–A review. Clinical nutrition ESPEN. 2017 Oct 1;21:31-9.
19. Corcoran C, Murphy C, Culligan EP, Walton J, Sleator RD. Malnutrition in the elderly.
Science Progress. 2019 Jun;102(2):171-80.
20. Ueland Ø. Appetite for life-Maintaining appetite for foods at old and very old age.
21. . Dietitians Association of Australia. Orthorexia: The unhealthy side of healthy eating –
Dietitians Association of Australia [Internet]. Daa.asn.au. 2019 [cited 25 September
2019]. Available from:
https://daa.asn.au/smart-eating-for-you/smart-eating-fast-facts/medical/orthorexia-the-
unhealthy-side-of-healthy-eating/.
22. Pilgrim A, Robinson S, Sayer AA, Roberts H. An overview of appetite decline in older
people. Nursing older people. 2015 Jun;27(5):29.
23. Dietitians Association of Australia. Australian Standards for Texture Modified Foods and
Fluids [Internet]. Daa.asn.au. 2019 [cited 25 September 2019]. Available from:
16. Praagman J, de Jonge EA, Kiefte-de Jong JC, Beulens JW, Sluijs I, Schoufour JD,
Hofman A, van der Schouw YT, Franco OH. Dietary saturated fatty acids and coronary
heart disease risk in a Dutch middle-aged and elderly population. Arteriosclerosis,
thrombosis, and vascular biology. 2016 Sep;36(9):2011-8.
17. Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, Thompson PL,
Lewis JR. Dietary saturated fat intake and atherosclerotic vascular disease mortality in
elderly women: a prospective cohort study. The American journal of clinical nutrition.
2015 Jun 1;101(6):1263-8.
18. Siddique N, O'Donoghue M, Casey MC, Walsh JB. Malnutrition in the elderly and its
effects on bone health–A review. Clinical nutrition ESPEN. 2017 Oct 1;21:31-9.
19. Corcoran C, Murphy C, Culligan EP, Walton J, Sleator RD. Malnutrition in the elderly.
Science Progress. 2019 Jun;102(2):171-80.
20. Ueland Ø. Appetite for life-Maintaining appetite for foods at old and very old age.
21. . Dietitians Association of Australia. Orthorexia: The unhealthy side of healthy eating –
Dietitians Association of Australia [Internet]. Daa.asn.au. 2019 [cited 25 September
2019]. Available from:
https://daa.asn.au/smart-eating-for-you/smart-eating-fast-facts/medical/orthorexia-the-
unhealthy-side-of-healthy-eating/.
22. Pilgrim A, Robinson S, Sayer AA, Roberts H. An overview of appetite decline in older
people. Nursing older people. 2015 Jun;27(5):29.
23. Dietitians Association of Australia. Australian Standards for Texture Modified Foods and
Fluids [Internet]. Daa.asn.au. 2019 [cited 25 September 2019]. Available from:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.