Case Study Analysis: Liver Cirrhosis, Patient Symptoms, and Care
VerifiedAdded on 2023/04/07
|10
|2227
|454
Case Study
AI Summary
This case study focuses on a patient diagnosed with liver cirrhosis, exploring the disease's causes, incidence, and risk factors, including chronic hepatitis C and alcohol consumption. The study delves into the impact of the disease on the patient and his family, highlighting physical symptoms like ascites, edema, and jaundice, as well as psychological distress and financial burdens. It further examines three common signs and symptoms with their underlying pathophysiology, such as portal hypertension and liver malfunction. The case study includes a discussion of Furosemide's pharmacodynamics and pharmacokinetics, a common medication used in treating ascites. Finally, a comprehensive nursing care plan is presented, detailing goals, interventions, and rationales for stabilizing oxygen saturation, managing edema, restricting fluid intake, and preventing infection, thus providing a holistic approach to patient care.

Running head:CASE STUDY ON LIVER CIRRHOSIS
CASE STUDY ON LIVER CIRRHOSIS
Name of the Student:
Name of the University:
Author Note:
CASE STUDY ON LIVER CIRRHOSIS
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1CASE STUDY ON LIVER CIRRHOSIS
Answer: 1
Liver cirrhosis causes scarring of liver. It is caused by different forms of liver or
hepatic anomalies. Chronic alcohol consumption and hepatitis can cause liver cirrhosis. If the
liver is abused due to any past diseases like hepatitis or excessive alcohol consumption the
scar tissues form to repair the damage (Tsochatzis, Bosch & Burroughs, 2014). The
disproportionate formation of scar tissues makes it difficult for the liver to function and can
become life threatening.
Causes:
Excessive consumption of alcohol
Viral hepatitis B,C and D (Wiest, Lawson & Geuking, 2014).
Hemochromatosis or iron accumulation in the body.
Cystic fibrosis.
Accumulation of excess fat in the liver.
Wilson’s disease due to copper accumulation in the liver.
Biliary atresia.
Glycogen storage or Galactosemia disease.
Digestive disorder Alagille syndrome.
Deficiency of Alpha-1 antitrypsin.
Biliary cirrhosis.
Autoimmune hepatitis disease.
Syphilis infection.
Scarring and toughening of the bile ducts which are called as sclerosing cholangitis
(Zhou, Zhang &Qiao, 2014).
Answer: 1
Liver cirrhosis causes scarring of liver. It is caused by different forms of liver or
hepatic anomalies. Chronic alcohol consumption and hepatitis can cause liver cirrhosis. If the
liver is abused due to any past diseases like hepatitis or excessive alcohol consumption the
scar tissues form to repair the damage (Tsochatzis, Bosch & Burroughs, 2014). The
disproportionate formation of scar tissues makes it difficult for the liver to function and can
become life threatening.
Causes:
Excessive consumption of alcohol
Viral hepatitis B,C and D (Wiest, Lawson & Geuking, 2014).
Hemochromatosis or iron accumulation in the body.
Cystic fibrosis.
Accumulation of excess fat in the liver.
Wilson’s disease due to copper accumulation in the liver.
Biliary atresia.
Glycogen storage or Galactosemia disease.
Digestive disorder Alagille syndrome.
Deficiency of Alpha-1 antitrypsin.
Biliary cirrhosis.
Autoimmune hepatitis disease.
Syphilis infection.
Scarring and toughening of the bile ducts which are called as sclerosing cholangitis
(Zhou, Zhang &Qiao, 2014).
2CASE STUDY ON LIVER CIRRHOSIS
The main cause of liver cirrhosis by Mr. Nathan James is hepatitis C-infection before 10
years. Wiest, Lawson and Geuking (2014) stated that chronic hepatitis C infection increases
the vulnerability of developing hepatitis c via damaging the hepatic cells and promoting the
occurrence of the progressive liver injury. This damage of the liver cells and progressive liver
injury promotes the development of the liver cirrhosis during the later part of life, after 10 to
20 years. Another reason which has increased the vulnerability of developing liver cirrhosis
in Mr. James is his addiction towards alcohol. As per the case study, Mr. James used of
consume 2 cans of beer per day. Since the liver of Mr. James is already damage due to the
previous infection history of hepatitis C, further charring of the liver cells by alchol made the
disease development an indispensible case (Tsochatzis, Bosch & Burroughs, 2014). However,
from the case study it is still not clear that whether Mr. Jams is suffering from alcoholic on
non-alcoholic liver disease.
Incidence:
The estimation of liver cirrhosis is about 14 people out of 100000. Common aetiology
of liver cirrhosis is excessive alcohol consumption which is 58% of total incidents of liver
cirrhosis. Hepatitis C is the reason of 13% while 12% is caused by cryptogenic cirrhosis.
Ascites is diagnosed in 43% of the cases while encephalopathy and variceal bleeding is seen
in 4% and 6% of the cases respectively. 1 year survival rate is 79%, 5 years of survival rate is
47% while 10 years of survival rate is 27% (Mokdad et al., 2014). Women have better
survival rate than men.
Risk factors:
Overconsumption of alcohol is a risk factor for cirrhosis.
Being obese may lead to liver cirrhosis like and such cirrhosis can be driven
by non-alcoholic or alcoholic liver disease
The main cause of liver cirrhosis by Mr. Nathan James is hepatitis C-infection before 10
years. Wiest, Lawson and Geuking (2014) stated that chronic hepatitis C infection increases
the vulnerability of developing hepatitis c via damaging the hepatic cells and promoting the
occurrence of the progressive liver injury. This damage of the liver cells and progressive liver
injury promotes the development of the liver cirrhosis during the later part of life, after 10 to
20 years. Another reason which has increased the vulnerability of developing liver cirrhosis
in Mr. James is his addiction towards alcohol. As per the case study, Mr. James used of
consume 2 cans of beer per day. Since the liver of Mr. James is already damage due to the
previous infection history of hepatitis C, further charring of the liver cells by alchol made the
disease development an indispensible case (Tsochatzis, Bosch & Burroughs, 2014). However,
from the case study it is still not clear that whether Mr. Jams is suffering from alcoholic on
non-alcoholic liver disease.
Incidence:
The estimation of liver cirrhosis is about 14 people out of 100000. Common aetiology
of liver cirrhosis is excessive alcohol consumption which is 58% of total incidents of liver
cirrhosis. Hepatitis C is the reason of 13% while 12% is caused by cryptogenic cirrhosis.
Ascites is diagnosed in 43% of the cases while encephalopathy and variceal bleeding is seen
in 4% and 6% of the cases respectively. 1 year survival rate is 79%, 5 years of survival rate is
47% while 10 years of survival rate is 27% (Mokdad et al., 2014). Women have better
survival rate than men.
Risk factors:
Overconsumption of alcohol is a risk factor for cirrhosis.
Being obese may lead to liver cirrhosis like and such cirrhosis can be driven
by non-alcoholic or alcoholic liver disease
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CASE STUDY ON LIVER CIRRHOSIS
Viral hepatitis eventually leads to liver cirrhosis in most of the cases (Qin et
al., 2014). Mr. Nathan James also suffered from Hepatitis C ten years ago.
Impact of liver cirrhosis on the patient and his family:
Mr. Nathan James is married and has two sons. He is an interstate truck driver. He is a
lethargic guy and slightly ill-tempered. His health conditions due to liver cirrhosis are getting
deteriorated. As a truck driver he needs to drive for a long time and stay out of home but in
this condition he needs to take rest and go through the required treatment procedures. If he
cannot work then it will create a financial crisis in the family and the cost of treatment will be
an added burden in this situation. His family members are anxious and distressed because of
his health conditions and the economic crisis they have to go through. Under psychological
distress parameter it can be said that Mr. James is spitting blood stained sputum along with a
drastic weight loss and loss of appetite. He has also developed few unexplained scars and
bruises on his arms along with the development of the distended abdomen. This constant
psychological tension along with problematic physiological parameters is the reason behind
which Mr. James remain irritated. This affects how overall quality of life of Mr. James is
affected du to the development of chronic disease (Golics et al., 2013).
Answer: 2
Common sign and symptoms of liver cirrhosis are:
Swelling in the abdomen and legs: High pressure in the portal vein leads to
accumulation of fluid in legs called as edema and in the abdomen known as ascites.
The liver cannot produce enough blood proteins like albumin so the edema and ascites
are caused. Due to lack of clotting proteins which is produced by the liver Mr. James
had bruises on his legs and arms. Abnormal blood vessels and delayed clotting of
blood is the reason behind this symptom which was caused by the lack blood clotting
Viral hepatitis eventually leads to liver cirrhosis in most of the cases (Qin et
al., 2014). Mr. Nathan James also suffered from Hepatitis C ten years ago.
Impact of liver cirrhosis on the patient and his family:
Mr. Nathan James is married and has two sons. He is an interstate truck driver. He is a
lethargic guy and slightly ill-tempered. His health conditions due to liver cirrhosis are getting
deteriorated. As a truck driver he needs to drive for a long time and stay out of home but in
this condition he needs to take rest and go through the required treatment procedures. If he
cannot work then it will create a financial crisis in the family and the cost of treatment will be
an added burden in this situation. His family members are anxious and distressed because of
his health conditions and the economic crisis they have to go through. Under psychological
distress parameter it can be said that Mr. James is spitting blood stained sputum along with a
drastic weight loss and loss of appetite. He has also developed few unexplained scars and
bruises on his arms along with the development of the distended abdomen. This constant
psychological tension along with problematic physiological parameters is the reason behind
which Mr. James remain irritated. This affects how overall quality of life of Mr. James is
affected du to the development of chronic disease (Golics et al., 2013).
Answer: 2
Common sign and symptoms of liver cirrhosis are:
Swelling in the abdomen and legs: High pressure in the portal vein leads to
accumulation of fluid in legs called as edema and in the abdomen known as ascites.
The liver cannot produce enough blood proteins like albumin so the edema and ascites
are caused. Due to lack of clotting proteins which is produced by the liver Mr. James
had bruises on his legs and arms. Abnormal blood vessels and delayed clotting of
blood is the reason behind this symptom which was caused by the lack blood clotting
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CASE STUDY ON LIVER CIRRHOSIS
proteins (Louvet&Mathurin, 2015).Mr. James reported ascites in the abdomen which
was bloated up and tight. Edema was reported in his ankles.
Portal hypertension and Bleeding:Portal hypertension is the reason that the blood is
redirected to the smaller veins. Portal hypertension is caused by high BP. This results
in extra pressure and the smaller veins burst due to this (Kinjo et al., 2014). This
causes serious bleeding. Portal hypertension causes varices in the veins, esophagus
and stomach which are called as varices, esophageal varices and gastric varices
respectively. This causes excess bleeding which can be life-threatening. As the liver
cannot produce enough clotting proteins the bleeding does not stop easily. It was
reported that Mr. James was spitting blood stained sputum in the last few weeks.
There were no shortness of breath or cough along with that.
Malfunction of liver:Accumulation of scar tissues on the liver causes malfunction of
the liver. So the body cannot process nutrients which leads to weakness and loss of
bodyweight. This leads to loss of appetite as the digestion system gets disrupted. Mr.
James reported about loss of 9 kilos of body weight due to lack of appetite.Jaundice
can develop when the liver does not remove bilirubin which is a waste end product of
blood.It causes darkening of urine. Yellow skin and white eye is resulted from
jaundice.
Answer: 3
Answer:Furosemide can be used for the ascites developed from liver cirrhosis.
Pharmacodynamics of furosemide
Furosemide is a loop diuretic of sulphonamide type which is related to bumetanide. It
is used to control hypertension and edema associated with liver cirrhosis. Furosemide is a
loop diuretic. It inhibits the reabsorption of water from the nephron by blocking sodium-
proteins (Louvet&Mathurin, 2015).Mr. James reported ascites in the abdomen which
was bloated up and tight. Edema was reported in his ankles.
Portal hypertension and Bleeding:Portal hypertension is the reason that the blood is
redirected to the smaller veins. Portal hypertension is caused by high BP. This results
in extra pressure and the smaller veins burst due to this (Kinjo et al., 2014). This
causes serious bleeding. Portal hypertension causes varices in the veins, esophagus
and stomach which are called as varices, esophageal varices and gastric varices
respectively. This causes excess bleeding which can be life-threatening. As the liver
cannot produce enough clotting proteins the bleeding does not stop easily. It was
reported that Mr. James was spitting blood stained sputum in the last few weeks.
There were no shortness of breath or cough along with that.
Malfunction of liver:Accumulation of scar tissues on the liver causes malfunction of
the liver. So the body cannot process nutrients which leads to weakness and loss of
bodyweight. This leads to loss of appetite as the digestion system gets disrupted. Mr.
James reported about loss of 9 kilos of body weight due to lack of appetite.Jaundice
can develop when the liver does not remove bilirubin which is a waste end product of
blood.It causes darkening of urine. Yellow skin and white eye is resulted from
jaundice.
Answer: 3
Answer:Furosemide can be used for the ascites developed from liver cirrhosis.
Pharmacodynamics of furosemide
Furosemide is a loop diuretic of sulphonamide type which is related to bumetanide. It
is used to control hypertension and edema associated with liver cirrhosis. Furosemide is a
loop diuretic. It inhibits the reabsorption of water from the nephron by blocking sodium-
5CASE STUDY ON LIVER CIRRHOSIS
potassium (K+)/Chloride(Cl-) co-transporter (NKCC2) present in the thick ascending limb of
Henle’s loop. Competitive inhibition at Cl-binding site on the co-transporter leads to the
inactivation of K+/Cl- ion channel. This results in prevention of sodium transport from the
lumen of Henle’s Loop to the basolateral interstitium. Subsequently lumen of loop of Henle
becomes more hypertonic and the basolateral interstitium becomes comparatively less
hypertonic (Brater, 2013). Osmotic gradient for water reabsorption in nephron is diminished
as a result the thick ascending limb contributes to 25% of the total sodium reabsorption in the
nephron.
Pharmacokinetics of furosemide
Furosemide constrains reabsorption of water in the nephron by inhibiting NKCC2 in
thick ascending limb, which is a part of the loop of Henle. This diuretic is used in anti-
hypertensive therapy to improve the condition of edema. Half-life of furosemide is 1 hour
with oral bioavailability of 65% as it is absorbed quickly but in an incomplete way after it is
administered orally (Huang et al., 2016). Peak concentration of plasma drug is reached after 1
to 2 hours. It is bound to plasma proteins so the delivery to the tubule is limited by filtration.
65% of the furosemide is excreted in an unchanged manner through urine. The remaining part
is conjugated in the kidneyto the glucuronic acid.
Answer: 4
Nursing Care Plan Goals Interventions Rationales
Stabilization of the oxygen
saturation (at present Mr.
Nathan James has SpO2:
88% on RA and 95% on
6L through Hudson mask)
Keeping the oxygen saturation
steady by continuation of the
titrated external oxygen supply
with the help of the Hudson
mark or by the installation of the
nasal canulla
1. Proper oxygen saturation (SpO2: 95 to
100%) will help to decrease the severity
of the tachypnnoia
2. Patients like Mr. James who are
suffering from liver diseases are
vulnerable towards developing hypoxic
potassium (K+)/Chloride(Cl-) co-transporter (NKCC2) present in the thick ascending limb of
Henle’s loop. Competitive inhibition at Cl-binding site on the co-transporter leads to the
inactivation of K+/Cl- ion channel. This results in prevention of sodium transport from the
lumen of Henle’s Loop to the basolateral interstitium. Subsequently lumen of loop of Henle
becomes more hypertonic and the basolateral interstitium becomes comparatively less
hypertonic (Brater, 2013). Osmotic gradient for water reabsorption in nephron is diminished
as a result the thick ascending limb contributes to 25% of the total sodium reabsorption in the
nephron.
Pharmacokinetics of furosemide
Furosemide constrains reabsorption of water in the nephron by inhibiting NKCC2 in
thick ascending limb, which is a part of the loop of Henle. This diuretic is used in anti-
hypertensive therapy to improve the condition of edema. Half-life of furosemide is 1 hour
with oral bioavailability of 65% as it is absorbed quickly but in an incomplete way after it is
administered orally (Huang et al., 2016). Peak concentration of plasma drug is reached after 1
to 2 hours. It is bound to plasma proteins so the delivery to the tubule is limited by filtration.
65% of the furosemide is excreted in an unchanged manner through urine. The remaining part
is conjugated in the kidneyto the glucuronic acid.
Answer: 4
Nursing Care Plan Goals Interventions Rationales
Stabilization of the oxygen
saturation (at present Mr.
Nathan James has SpO2:
88% on RA and 95% on
6L through Hudson mask)
Keeping the oxygen saturation
steady by continuation of the
titrated external oxygen supply
with the help of the Hudson
mark or by the installation of the
nasal canulla
1. Proper oxygen saturation (SpO2: 95 to
100%) will help to decrease the severity
of the tachypnnoia
2. Patients like Mr. James who are
suffering from liver diseases are
vulnerable towards developing hypoxic
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CASE STUDY ON LIVER CIRRHOSIS
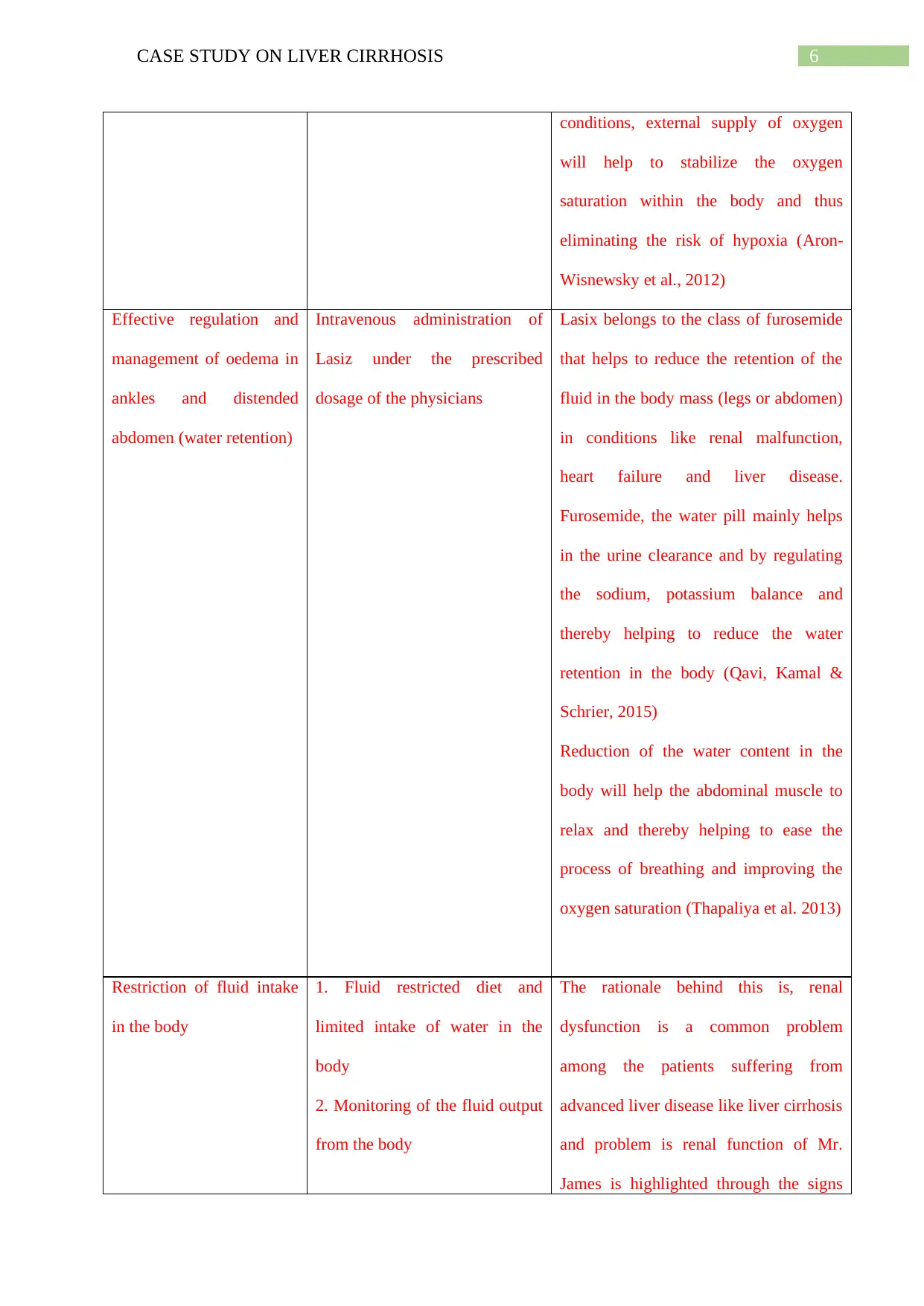
conditions, external supply of oxygen
will help to stabilize the oxygen
saturation within the body and thus
eliminating the risk of hypoxia (Aron-
Wisnewsky et al., 2012)
Effective regulation and
management of oedema in
ankles and distended
abdomen (water retention)
Intravenous administration of
Lasiz under the prescribed
dosage of the physicians
Lasix belongs to the class of furosemide
that helps to reduce the retention of the
fluid in the body mass (legs or abdomen)
in conditions like renal malfunction,
heart failure and liver disease.
Furosemide, the water pill mainly helps
in the urine clearance and by regulating
the sodium, potassium balance and
thereby helping to reduce the water
retention in the body (Qavi, Kamal &
Schrier, 2015)
Reduction of the water content in the
body will help the abdominal muscle to
relax and thereby helping to ease the
process of breathing and improving the
oxygen saturation (Thapaliya et al. 2013)
Restriction of fluid intake
in the body
1. Fluid restricted diet and
limited intake of water in the
body
2. Monitoring of the fluid output
from the body
The rationale behind this is, renal
dysfunction is a common problem
among the patients suffering from
advanced liver disease like liver cirrhosis
and problem is renal function of Mr.
James is highlighted through the signs
conditions, external supply of oxygen
will help to stabilize the oxygen
saturation within the body and thus
eliminating the risk of hypoxia (Aron-
Wisnewsky et al., 2012)
Effective regulation and
management of oedema in
ankles and distended
abdomen (water retention)
Intravenous administration of
Lasiz under the prescribed
dosage of the physicians
Lasix belongs to the class of furosemide
that helps to reduce the retention of the
fluid in the body mass (legs or abdomen)
in conditions like renal malfunction,
heart failure and liver disease.
Furosemide, the water pill mainly helps
in the urine clearance and by regulating
the sodium, potassium balance and
thereby helping to reduce the water
retention in the body (Qavi, Kamal &
Schrier, 2015)
Reduction of the water content in the
body will help the abdominal muscle to
relax and thereby helping to ease the
process of breathing and improving the
oxygen saturation (Thapaliya et al. 2013)
Restriction of fluid intake
in the body
1. Fluid restricted diet and
limited intake of water in the
body
2. Monitoring of the fluid output
from the body
The rationale behind this is, renal
dysfunction is a common problem
among the patients suffering from
advanced liver disease like liver cirrhosis
and problem is renal function of Mr.
James is highlighted through the signs
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CASE STUDY ON LIVER CIRRHOSIS
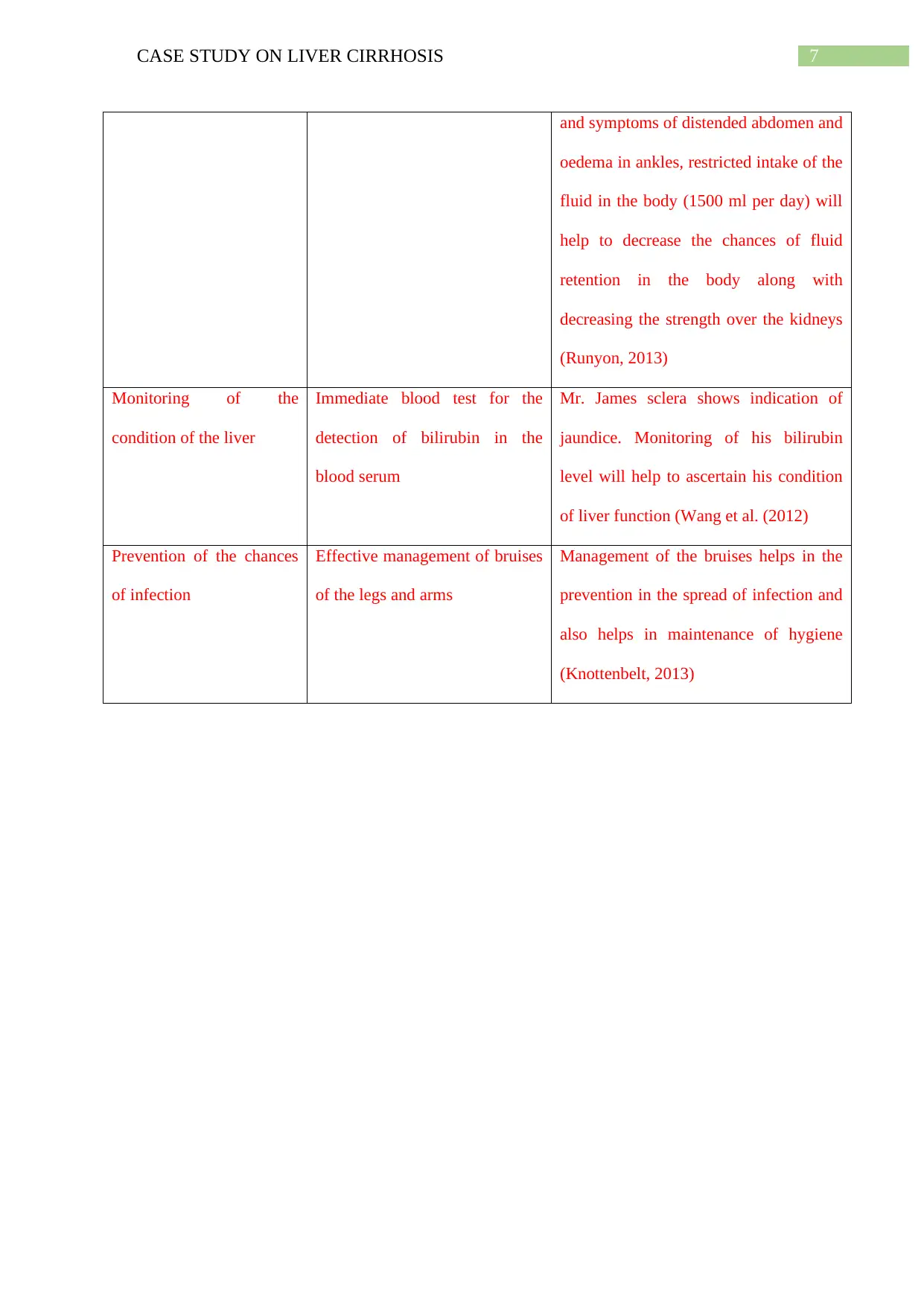
and symptoms of distended abdomen and
oedema in ankles, restricted intake of the
fluid in the body (1500 ml per day) will
help to decrease the chances of fluid
retention in the body along with
decreasing the strength over the kidneys
(Runyon, 2013)
Monitoring of the
condition of the liver
Immediate blood test for the
detection of bilirubin in the
blood serum
Mr. James sclera shows indication of
jaundice. Monitoring of his bilirubin
level will help to ascertain his condition
of liver function (Wang et al. (2012)
Prevention of the chances
of infection
Effective management of bruises
of the legs and arms
Management of the bruises helps in the
prevention in the spread of infection and
also helps in maintenance of hygiene
(Knottenbelt, 2013)
and symptoms of distended abdomen and
oedema in ankles, restricted intake of the
fluid in the body (1500 ml per day) will
help to decrease the chances of fluid
retention in the body along with
decreasing the strength over the kidneys
(Runyon, 2013)
Monitoring of the
condition of the liver
Immediate blood test for the
detection of bilirubin in the
blood serum
Mr. James sclera shows indication of
jaundice. Monitoring of his bilirubin
level will help to ascertain his condition
of liver function (Wang et al. (2012)
Prevention of the chances
of infection
Effective management of bruises
of the legs and arms
Management of the bruises helps in the
prevention in the spread of infection and
also helps in maintenance of hygiene
(Knottenbelt, 2013)
8CASE STUDY ON LIVER CIRRHOSIS
References
Aron-Wisnewsky, J., Minville, C., Tordjman, J., Lévy, P., Bouillot, J. L., Basdevant,
A., ...&Pépin, J. L. (2012). Chronic intermittent hypoxia is a major trigger for non-
alcoholic fatty liver disease in morbid obese. Journal of hepatology, 56(1), 225-233.
Brater, D. C. (2013). Mechanism of action of diuretics. UpToDate. http://0-www. uptodate.
com. library. cedarville. edu/contents/mechanism-of-actionof-diuretics.
Golics, C. J., Basra, M. K. A., Salek, M. S., & Finlay, A. Y. (2013).The impact of patients’
chronic disease on family quality of life: an experience from 26
specialties. International journal of general medicine, 6, 787.
Huang, X., DorhoutMees, E., Vos, P., Hamza, S., &Braam, B. (2016). Everything we always
wanted to know about furosemide but were afraid to ask. American Journal of
Physiology-Renal Physiology, 310(10), F958-F971.
Kinjo, N., Kawanaka, H., Akahoshi, T., Matsumoto, Y., Kamori, M., Nagao,
Y., ...&Maehara, Y. (2014). Portal vein thrombosis in liver cirrhosis. World journal of
hepatology, 6(2), 64.
Knottenbelt, D. C. (2013). Handbook of Equine Wound Management E-Book. Elsevier Health
Sciences.
Louvet, A., &Mathurin, P. (2015). Alcoholic liver disease: mechanisms of injury and targeted
treatment. Nature reviews Gastroenterology &hepatology, 12(4), 231.
Mokdad, A. A., Lopez, A. D., Shahraz, S., Lozano, R., Mokdad, A. H., Stanaway,
J., ...&Naghavi, M. (2014). Liver cirrhosis mortality in 187 countries between 1980
and 2010: a systematic analysis. BMC medicine, 12(1), 145.
References
Aron-Wisnewsky, J., Minville, C., Tordjman, J., Lévy, P., Bouillot, J. L., Basdevant,
A., ...&Pépin, J. L. (2012). Chronic intermittent hypoxia is a major trigger for non-
alcoholic fatty liver disease in morbid obese. Journal of hepatology, 56(1), 225-233.
Brater, D. C. (2013). Mechanism of action of diuretics. UpToDate. http://0-www. uptodate.
com. library. cedarville. edu/contents/mechanism-of-actionof-diuretics.
Golics, C. J., Basra, M. K. A., Salek, M. S., & Finlay, A. Y. (2013).The impact of patients’
chronic disease on family quality of life: an experience from 26
specialties. International journal of general medicine, 6, 787.
Huang, X., DorhoutMees, E., Vos, P., Hamza, S., &Braam, B. (2016). Everything we always
wanted to know about furosemide but were afraid to ask. American Journal of
Physiology-Renal Physiology, 310(10), F958-F971.
Kinjo, N., Kawanaka, H., Akahoshi, T., Matsumoto, Y., Kamori, M., Nagao,
Y., ...&Maehara, Y. (2014). Portal vein thrombosis in liver cirrhosis. World journal of
hepatology, 6(2), 64.
Knottenbelt, D. C. (2013). Handbook of Equine Wound Management E-Book. Elsevier Health
Sciences.
Louvet, A., &Mathurin, P. (2015). Alcoholic liver disease: mechanisms of injury and targeted
treatment. Nature reviews Gastroenterology &hepatology, 12(4), 231.
Mokdad, A. A., Lopez, A. D., Shahraz, S., Lozano, R., Mokdad, A. H., Stanaway,
J., ...&Naghavi, M. (2014). Liver cirrhosis mortality in 187 countries between 1980
and 2010: a systematic analysis. BMC medicine, 12(1), 145.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CASE STUDY ON LIVER CIRRHOSIS
Qavi, A. H., Kamal, R., &Schrier, R. W. (2015).Clinical use of diuretics in heart failure,
cirrhosis, and nephrotic syndrome. International journal of nephrology, 2015.
Qin, N., Yang, F., Li, A., Prifti, E., Chen, Y., Shao, L., ...& Zhou, J. (2014). Alterations of
the human gut microbiome in liver cirrhosis. Nature, 513(7516), 59.
Runyon, B. A. (2013). Introduction to the revised American Association for the Study of
Liver Diseases Practice Guideline management of adult patients with ascites due to
cirrhosis 2012. Hepatology, 57(4), 1651-1653.
Thapaliya, K., Bhandary, A., Basnet, S., &Aryal, B. (2013).Clinical status of furosemide on
liver cirrhosis with portal hypertension and ascites. Journal of Chitwan Medical
College, 3(1), 65-66.
Tsochatzis, E. A., Bosch, J., & Burroughs, A. K. (2014). Liver cirrhosis. The Lancet,
383(9930), 1749-1761.
Wang, X., Zhang, A., Han, Y., Wang, P., Sun, H., Song, G., ...&Xie, N. (2012). Urine
metabolomics analysis for biomarker discovery and detection of jaundice syndrome in
patients with liver disease. Molecular & Cellular Proteomics, 11(8), 370-380.
Wiest, R., Lawson, M., & Geuking, M. (2014). Pathological bacterial translocation in liver
cirrhosis. Journal of hepatology, 60(1), 197-209.
Zhou, W. C., Zhang, Q. B., &Qiao, L. (2014). Pathogenesis of liver cirrhosis. World journal
of gastroenterology: WJG, 20(23), 7312.
Qavi, A. H., Kamal, R., &Schrier, R. W. (2015).Clinical use of diuretics in heart failure,
cirrhosis, and nephrotic syndrome. International journal of nephrology, 2015.
Qin, N., Yang, F., Li, A., Prifti, E., Chen, Y., Shao, L., ...& Zhou, J. (2014). Alterations of
the human gut microbiome in liver cirrhosis. Nature, 513(7516), 59.
Runyon, B. A. (2013). Introduction to the revised American Association for the Study of
Liver Diseases Practice Guideline management of adult patients with ascites due to
cirrhosis 2012. Hepatology, 57(4), 1651-1653.
Thapaliya, K., Bhandary, A., Basnet, S., &Aryal, B. (2013).Clinical status of furosemide on
liver cirrhosis with portal hypertension and ascites. Journal of Chitwan Medical
College, 3(1), 65-66.
Tsochatzis, E. A., Bosch, J., & Burroughs, A. K. (2014). Liver cirrhosis. The Lancet,
383(9930), 1749-1761.
Wang, X., Zhang, A., Han, Y., Wang, P., Sun, H., Song, G., ...&Xie, N. (2012). Urine
metabolomics analysis for biomarker discovery and detection of jaundice syndrome in
patients with liver disease. Molecular & Cellular Proteomics, 11(8), 370-380.
Wiest, R., Lawson, M., & Geuking, M. (2014). Pathological bacterial translocation in liver
cirrhosis. Journal of hepatology, 60(1), 197-209.
Zhou, W. C., Zhang, Q. B., &Qiao, L. (2014). Pathogenesis of liver cirrhosis. World journal
of gastroenterology: WJG, 20(23), 7312.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.