University: Diagnostic Algorithm of CF Lower Respiratory Infections
VerifiedAdded on 2022/09/29
|8
|1681
|28
Report
AI Summary
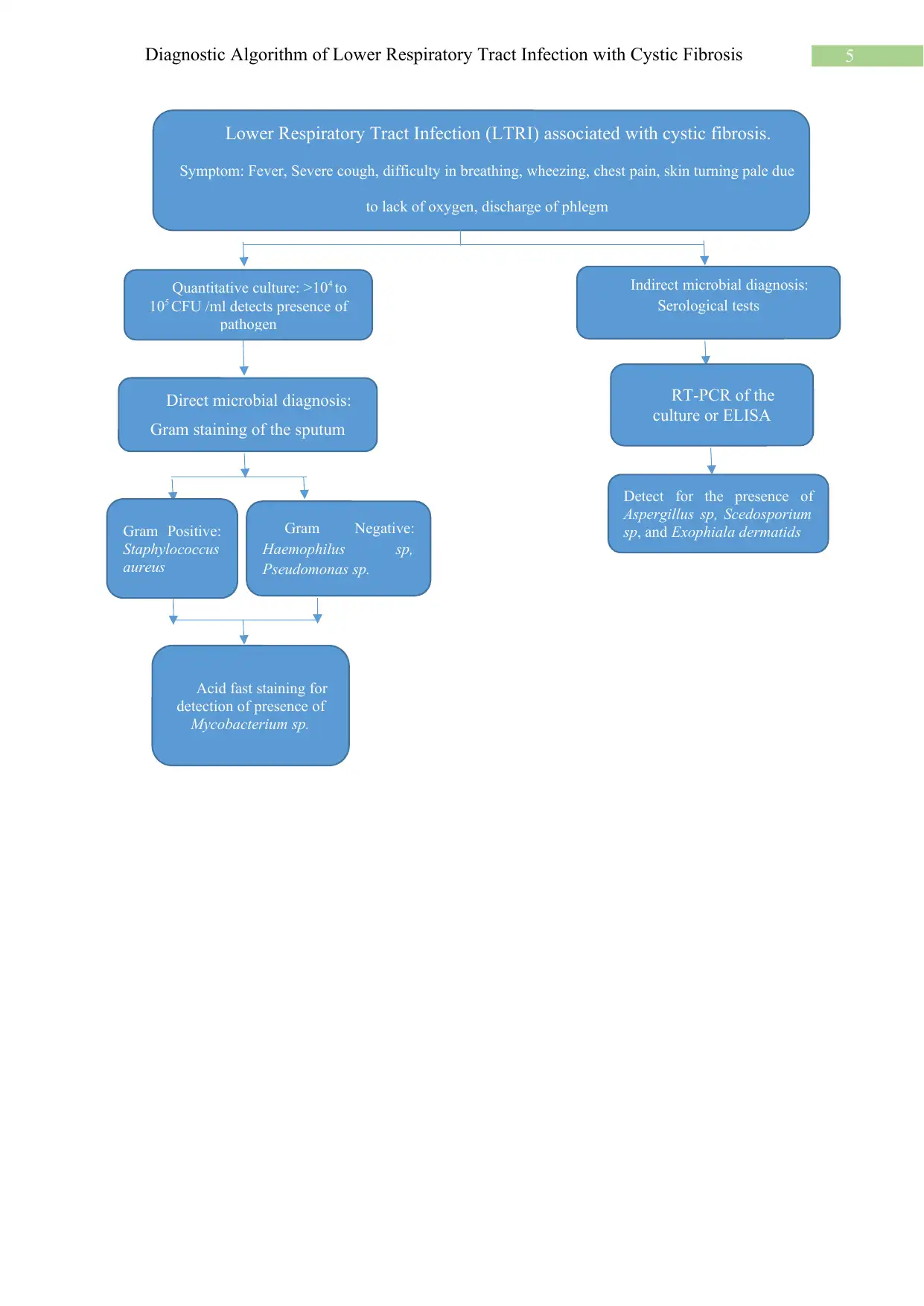
This report provides a diagnostic algorithm for the microbiological diagnosis of lower respiratory tract infections (LRTIs) in patients with cystic fibrosis (CF). It begins with an introduction highlighting the challenges in diagnosing these infections due to the complexity of the disease and the diversity of pathogens involved. The report then details various diagnostic methods, including Gram staining of sputum to identify common pathogens like Streptococcus pneumoniae and Staphylococcus aureus, and quantitative culture techniques using broncho-alveolar lavage (BAL) and other specimens. The report also discusses the detection of acute exacerbations of chronic bronchitis and the evaluation of pulmonary tuberculosis, emphasizing the role of both direct and indirect microbial diagnosis. Furthermore, it covers the significance of detecting opportunistic pathogens and the use of molecular methods like PCR for accurate diagnosis. The report concludes with a summary of the diagnostic algorithm, incorporating symptoms, direct and indirect microbial diagnosis, and quantitative culture results to guide effective management of CF-related LRTIs.


1 out of 8
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.