Optimizing Prehospital Asthma Care: Management and Interventions
VerifiedAdded on 2024/07/22
|9
|1311
|98
Report
AI Summary
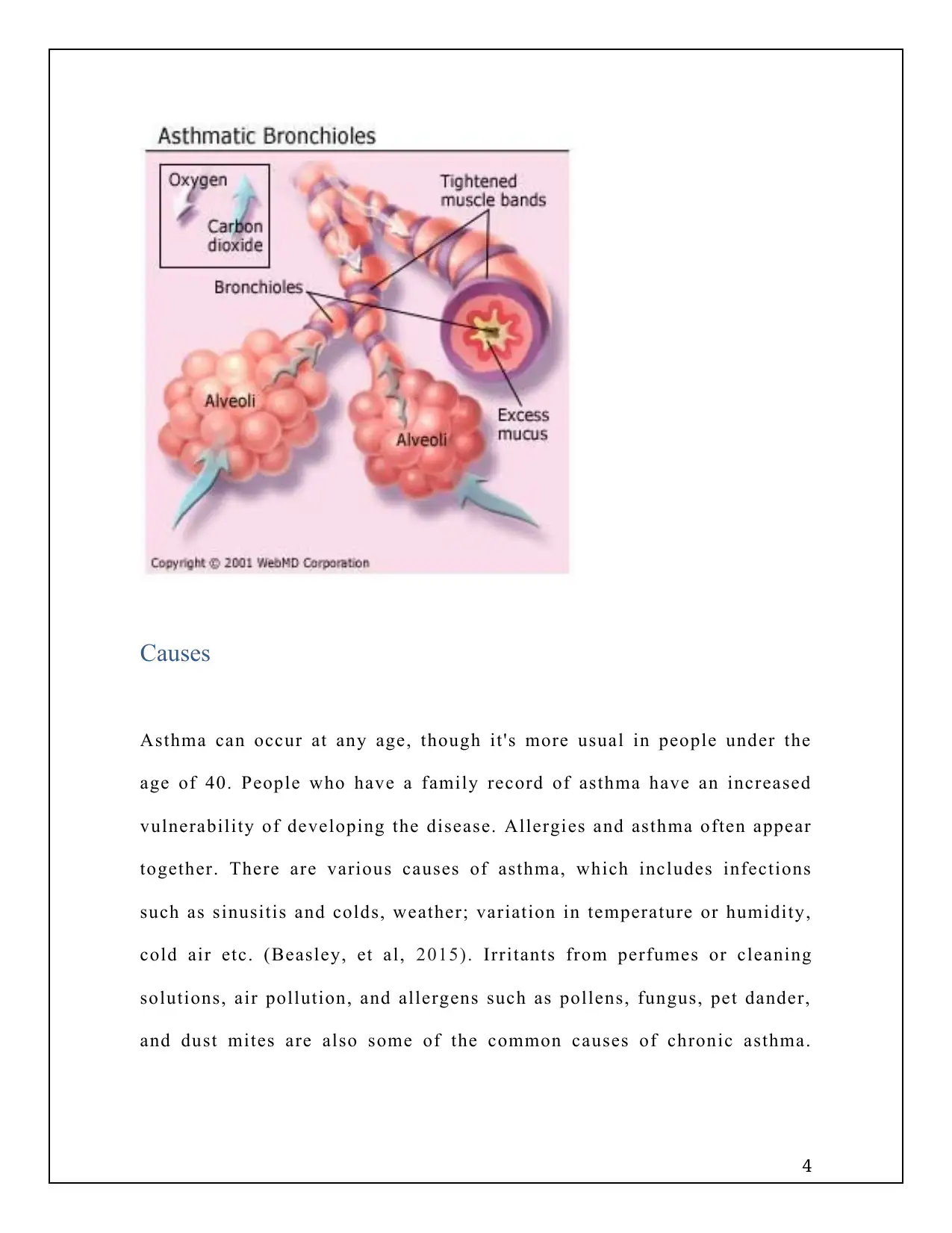
This report provides a detailed overview of managing asthma in the prehospital environment, emphasizing strategies to reduce hospital admissions. It begins by defining asthma as a chronic inflammatory disease affecting the airways and lungs, highlighting the importance of effective prehospital management to prevent exacerbations. The report discusses the causes of asthma, including allergies, infections, and environmental irritants, and explains the pathophysiology involving inflammation, airflow obstruction, and increased airway responsiveness. Key management and treatment approaches include periodic assessment, written action plans, allergen reduction, and pharmacological therapies such as corticosteroids and inhaled beta-agonists. The report concludes that implementing these strategies can significantly decrease hospitalization rates for asthma patients, underscoring the benefits of extended care and monitoring.
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.