Systematic Review: Validity and Reliability of Myers-Briggs Indicator
VerifiedAdded on 2022/12/30
|28
|12353
|44
Report
AI Summary
This report presents a systematic review and meta-analysis of the Myers-Briggs Type Indicator (MBTI), examining its validity and reliability. The study analyzed seven studies to assess the psychometric properties of the MBTI, which is frequently used in health professions and educational programs. The review investigated construct validity and test-retest reliability across the Extravert-Introvert, Sensing-Intuition, Thinking-Feeling, and Judging-Perceiving subscales. Findings suggest satisfactory reliabilities for most subscales, though heterogeneity was noted. The report highlights the importance of considering the MBTI's applicability to different populations, as the majority of studies were conducted on college-age students. The study underscores the need for careful interpretation of MBTI results and provides valuable insights for educators and practitioners using the instrument. This report is contributed by a student to be published on Desklib, a platform offering AI-based study tools.
J Best Pract Health Prof Divers (Spring, 2017), 10(1), 1–27.
ISSN: 2745-2843 © Winston-Salem State University
ORIGINAL RESEARCH
Validity and Reliability of the
Myers-Briggs Personality Type Indicator
A Systematic Review and Meta-analysis
Ken Randall,1 PhD, MHR, PT; Mary Isaacson,1 EdD;
Carrie Ciro,1 PhD, OTR/L, FAOTA
Author Affiliations:1Department of Rehabilitation Sciences, University of Oklahoma Health
Sciences Center, Tulsa and Oklahoma City, Oklahoma
Corresponding Author: Ken Randall, Department of Rehabilitation Sciences, University
of Oklahoma Schusterman Center, 4502 East 41st Street, Room 2H20, Tulsa, OK 74135
(Ken-Randall@ouhsc.edu)
ABSTRACT
The Myers-Briggs Type Indicator is frequently used by health professions and educationa
programs to address the diversity of personalities that exist. No systematic review of the
ture or meta-analysis of its validity and reliability has occurred. This comprehensive liter
search identified 221 potential studies, of which seven met our inclusion criteria. Four of
studies examined construct validity, but their varying methods did not permit pooling fo
meta-analysis. These studies agree that the instrument has reasonable construct validity
three studies of test-retest reliability did allow a meta-analysis to be performed, albeit w
tion due to substantial heterogeneity. Results indicate that the Extravert-Introvert, Sens
Intuition, and Judging-Perceiving Subscales have satisfactory reliabilities of .75 or higher
that the Thinking-Feeling subscale has a reliability of .61. The majority of studies were co
ducted on college-age students; thus, the evidence to support the tool’s utility applies m
to this group, and careful thought should be given when applying it to other individuals.
Keywordsn Myers-Briggs Type Indicatorn Personalityn Reliabilityn Validity
ISSN: 2745-2843 © Winston-Salem State University
ORIGINAL RESEARCH
Validity and Reliability of the
Myers-Briggs Personality Type Indicator
A Systematic Review and Meta-analysis
Ken Randall,1 PhD, MHR, PT; Mary Isaacson,1 EdD;
Carrie Ciro,1 PhD, OTR/L, FAOTA
Author Affiliations:1Department of Rehabilitation Sciences, University of Oklahoma Health
Sciences Center, Tulsa and Oklahoma City, Oklahoma
Corresponding Author: Ken Randall, Department of Rehabilitation Sciences, University
of Oklahoma Schusterman Center, 4502 East 41st Street, Room 2H20, Tulsa, OK 74135
(Ken-Randall@ouhsc.edu)
ABSTRACT
The Myers-Briggs Type Indicator is frequently used by health professions and educationa
programs to address the diversity of personalities that exist. No systematic review of the
ture or meta-analysis of its validity and reliability has occurred. This comprehensive liter
search identified 221 potential studies, of which seven met our inclusion criteria. Four of
studies examined construct validity, but their varying methods did not permit pooling fo
meta-analysis. These studies agree that the instrument has reasonable construct validity
three studies of test-retest reliability did allow a meta-analysis to be performed, albeit w
tion due to substantial heterogeneity. Results indicate that the Extravert-Introvert, Sens
Intuition, and Judging-Perceiving Subscales have satisfactory reliabilities of .75 or higher
that the Thinking-Feeling subscale has a reliability of .61. The majority of studies were co
ducted on college-age students; thus, the evidence to support the tool’s utility applies m
to this group, and careful thought should be given when applying it to other individuals.
Keywordsn Myers-Briggs Type Indicatorn Personalityn Reliabilityn Validity
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
INTRODUCTION
Personality is a commonly used term with a meaning that most of us readily comprehe
yet it is an elusive concept to fully describe or quantify. Broadly defined, it is the comb
of an individual’s cognitive, emotional, attitudinal, and behavioral response patterns (A
2009; McAdams, 2009). It has been studied since antiquity, with Hippocrates being am
the first to describe personality by grouping individuals into temperaments that relate
particular characteristics or types (Hippocrates 1923). Since then, countless theo
instruments have attempted to explicate and measure differences in personality more
Included in these instruments is the Myers-Briggs Type Indicator (MBTI), which is repo
to be one of the most widely used instruments in the world for understanding persona
differences (Briggs Myers, 1998; Jackson, Parker, & Dipboye, 1996; Lorr, 1991; Saggin
Kline, 1996; Salter, Evans, & Forney, 2006; Tzeng, Outcalt, Boyer, Ware, & Landis, 198
Zumbo & Taylor, 1993).
The MBTI is used extensively in human resource management and is one of the mo
commonly used instruments in higher education research and counseling (Hojat, Erdm
& Gonnella, 2013). Its application in medical education is quite varied and includes stu
of how certain preferences affect decision making (Pretz & Folse, 2011) and how know
of an individual’s type can enhance communication (Eksteen & Basson, 2015). Moreov
addressing the differences in type and preferences between instructors and students m
mize negative outcomes in both academic and clinical settings (Bell et al., 2011). In th
thors’ experience, we use the MBTI as both an educational and an academic adviseme
Our occupational therapy and physical therapy students learn about the 16 MBTI types
about how differing preferences can influence interactions with members of the health
team and with patients and their loved ones. We also provide academic advisors and c
instructors with information about individual student types that includes tips grounded
the MBTI literature on how to enhance their learning, communication, and feedback ba
on each student’s preference. Although we pay attention to the preferences of all stud
we also examine the preferences of learners from diverse backgrounds to determine i
trends exist in personality type. In an ongoing effort to use the best evidence to inform
educational program, we wanted to understand the psychometric properties of the MB
determine whether we should continue to use it with our students.
Since its inception in the 1940s, numerous studies have examined various aspects
MBTI, including many related to validity and reliability. Over the past 35 years, a numb
of relatively thorough reviews of the literature regarding these features of the MBTI ha
peared (Carlson, 1985; Carlyn, 1977; Gardner & Martinko, 1996; Murray, 1990; Pitteng
1993), including a compendium of research by the publishers of the tool itself (Thorne
Gough, 1999). However, none of these reviews was systematic in nature, nor did any a
INTRODUCTION
Personality is a commonly used term with a meaning that most of us readily comprehe
yet it is an elusive concept to fully describe or quantify. Broadly defined, it is the comb
of an individual’s cognitive, emotional, attitudinal, and behavioral response patterns (A
2009; McAdams, 2009). It has been studied since antiquity, with Hippocrates being am
the first to describe personality by grouping individuals into temperaments that relate
particular characteristics or types (Hippocrates 1923). Since then, countless theo
instruments have attempted to explicate and measure differences in personality more
Included in these instruments is the Myers-Briggs Type Indicator (MBTI), which is repo
to be one of the most widely used instruments in the world for understanding persona
differences (Briggs Myers, 1998; Jackson, Parker, & Dipboye, 1996; Lorr, 1991; Saggin
Kline, 1996; Salter, Evans, & Forney, 2006; Tzeng, Outcalt, Boyer, Ware, & Landis, 198
Zumbo & Taylor, 1993).
The MBTI is used extensively in human resource management and is one of the mo
commonly used instruments in higher education research and counseling (Hojat, Erdm
& Gonnella, 2013). Its application in medical education is quite varied and includes stu
of how certain preferences affect decision making (Pretz & Folse, 2011) and how know
of an individual’s type can enhance communication (Eksteen & Basson, 2015). Moreov
addressing the differences in type and preferences between instructors and students m
mize negative outcomes in both academic and clinical settings (Bell et al., 2011). In th
thors’ experience, we use the MBTI as both an educational and an academic adviseme
Our occupational therapy and physical therapy students learn about the 16 MBTI types
about how differing preferences can influence interactions with members of the health
team and with patients and their loved ones. We also provide academic advisors and c
instructors with information about individual student types that includes tips grounded
the MBTI literature on how to enhance their learning, communication, and feedback ba
on each student’s preference. Although we pay attention to the preferences of all stud
we also examine the preferences of learners from diverse backgrounds to determine i
trends exist in personality type. In an ongoing effort to use the best evidence to inform
educational program, we wanted to understand the psychometric properties of the MB
determine whether we should continue to use it with our students.
Since its inception in the 1940s, numerous studies have examined various aspects
MBTI, including many related to validity and reliability. Over the past 35 years, a numb
of relatively thorough reviews of the literature regarding these features of the MBTI ha
peared (Carlson, 1985; Carlyn, 1977; Gardner & Martinko, 1996; Murray, 1990; Pitteng
1993), including a compendium of research by the publishers of the tool itself (Thorne
Gough, 1999). However, none of these reviews was systematic in nature, nor did any a
Myers-Briggs Personality Type Indicator 3
the guidelines of the Cochrane Collaboration (2016), considered the standard for comp
hensive literature searches (Sampson et al., 2006) and quality appraisal. In 2002, Cap
and Capraro conducted a meta-analytic reliability generalization study of articles inves
a number of the psychometric properties of the MBTI; however, the scope of the study
limited to articles published between 1998 and 2001. To date, we could find no compl
systematic review of the literature or in-depth meta-analysis of studies that meet the
suggested by the Cochrane Collaboration to assess the psychometric properties of the
THE MYERS BRIGGS TYPE INDICATOR
The MBTI measures the degree to which an individual prefers to operate from four dic
mous type pairs using a series of forced-choice questions that represent behavioral pr
ences. In accord with Jung’s theory of types, it proposes that everyone has a natural p
for one of the two opposites on each of four scales, emphasizing that one preference i
better than another. According to supporters of the MBTI, this distinguishes it from mo
psychological assessments, which quantify personality traits, many of which consider
of the scale to be more positive and the other more negative (Schaubhut, Herk, & Tho
2009, p. 4). The MBTI emphasizes the word preference and uses single letters of the a
to denote its eight preferences. The definitions for each MBTI preference show a distin
with Jung’s original definitions:
Extraversion (E) is the tendency to focus on the outer world of people and
external events. People who prefer extraversion direct their energy and at-
tention outward and receive energy from external events, experiences, and
interactions.
Introversion (I) is the preference to focus on the inner world of ideas and ex-
periences. Individuals direct their energy and attention inward and receive
energy from their internal thoughts, feelings, reflections, and time alone.
Sensing (S) is the preference to take information in through the eyes, ears,
and other senses. People who are predominantly sensing are observant of
what is going on around them and are especially good at recognizing the
practical realities of a situation.
Intuition (N) is the ability to take in information by seeing the big picture,
focusing on relationships and connections between facts. People who prefer
intuition tend to grasp patterns and are especially adept at seeing new pos-
sibilities and different perspectives.
the guidelines of the Cochrane Collaboration (2016), considered the standard for comp
hensive literature searches (Sampson et al., 2006) and quality appraisal. In 2002, Cap
and Capraro conducted a meta-analytic reliability generalization study of articles inves
a number of the psychometric properties of the MBTI; however, the scope of the study
limited to articles published between 1998 and 2001. To date, we could find no compl
systematic review of the literature or in-depth meta-analysis of studies that meet the
suggested by the Cochrane Collaboration to assess the psychometric properties of the
THE MYERS BRIGGS TYPE INDICATOR
The MBTI measures the degree to which an individual prefers to operate from four dic
mous type pairs using a series of forced-choice questions that represent behavioral pr
ences. In accord with Jung’s theory of types, it proposes that everyone has a natural p
for one of the two opposites on each of four scales, emphasizing that one preference i
better than another. According to supporters of the MBTI, this distinguishes it from mo
psychological assessments, which quantify personality traits, many of which consider
of the scale to be more positive and the other more negative (Schaubhut, Herk, & Tho
2009, p. 4). The MBTI emphasizes the word preference and uses single letters of the a
to denote its eight preferences. The definitions for each MBTI preference show a distin
with Jung’s original definitions:
Extraversion (E) is the tendency to focus on the outer world of people and
external events. People who prefer extraversion direct their energy and at-
tention outward and receive energy from external events, experiences, and
interactions.
Introversion (I) is the preference to focus on the inner world of ideas and ex-
periences. Individuals direct their energy and attention inward and receive
energy from their internal thoughts, feelings, reflections, and time alone.
Sensing (S) is the preference to take information in through the eyes, ears,
and other senses. People who are predominantly sensing are observant of
what is going on around them and are especially good at recognizing the
practical realities of a situation.
Intuition (N) is the ability to take in information by seeing the big picture,
focusing on relationships and connections between facts. People who prefer
intuition tend to grasp patterns and are especially adept at seeing new pos-
sibilities and different perspectives.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
Thinking (T) is the preference in decision making to look at the logical con-
sequences of a choice or action. People who prefer this type try to mentally
remove themselves from a situation to examine it objectively and analyze
cause and effect.
Feeling (F) is the use of emotion in decision making, and people with this
preference tend to consider what is important to them and to other people.
They mentally place themselves in a situation and identify with the people
involved so that they can make decisions based on person-centered values.
Judging (J) is the preference to organize life in a planned, orderly way, with
a desire to regulate and control it. People who prefer judging make deci-
sions, achieve closure, and appreciate an environment that is structured
and organized.
Perceiving (P) is the tendency to live in a flexible, spontaneous way, seeking
to experience and understand life rather than control it. People who are
perceiving prefer to be open to experience and last-minute options. They
enjoy and trust their resourcefulness and ability to adapt to the demands of
a situation (Briggs-Myers, 1993; Hall & Nordby, 1973).
The MBTI treats each preference equally, so there are no principal functions or sub
ordinate functions as described by Jung. Given four sets of dichotomous preferences th
can occur in any combination, the MBTI proposes that there are sixteen different perso
types. With the MBTI, four letters represent each type, which indicate the four domina
preference areas. For example, ENFP is Extraversion Intuitive Feeling Perceiving, whic
its own set of characteristics, some like and some different from the other fifteen type
lar to Jung’s work in Psychological Types (1923), the MBTI addresses various combinat
each type, such as introverted-sensing or intuitive-thinking-perceiving. The MBTI allow
user to describe two people with the exact four-letter combination of preferences in ge
ties similar to both, yet accounts for the individual differences produced by variation o
extent (or strength) of each person’s preference. This echoes Jung’s belief that his typ
be used to describe groups of people as well as individuals (Jung, 1921/1923).
According to the companion manual to the MBTI, Introduction to Type (Briggs Myer
1998; Myers, Kirby, & Briggs Meyers, 2015), which was first published in 1970 and is c
in its seventh edition, the goal of the instrument is to foster self-understanding, enhan
learning and communication, assist with conflict management, and enhance relationsh
is a tool “with intent not to stereotype, but to allow understanding of individual prefere
(Jessup, 2002, p. 503). Between 1943 and 1975, the MBTI evolved through a number o
tions, spanning Forms A through F. In 1975 Consulting Psychologist Press acquired the
Thinking (T) is the preference in decision making to look at the logical con-
sequences of a choice or action. People who prefer this type try to mentally
remove themselves from a situation to examine it objectively and analyze
cause and effect.
Feeling (F) is the use of emotion in decision making, and people with this
preference tend to consider what is important to them and to other people.
They mentally place themselves in a situation and identify with the people
involved so that they can make decisions based on person-centered values.
Judging (J) is the preference to organize life in a planned, orderly way, with
a desire to regulate and control it. People who prefer judging make deci-
sions, achieve closure, and appreciate an environment that is structured
and organized.
Perceiving (P) is the tendency to live in a flexible, spontaneous way, seeking
to experience and understand life rather than control it. People who are
perceiving prefer to be open to experience and last-minute options. They
enjoy and trust their resourcefulness and ability to adapt to the demands of
a situation (Briggs-Myers, 1993; Hall & Nordby, 1973).
The MBTI treats each preference equally, so there are no principal functions or sub
ordinate functions as described by Jung. Given four sets of dichotomous preferences th
can occur in any combination, the MBTI proposes that there are sixteen different perso
types. With the MBTI, four letters represent each type, which indicate the four domina
preference areas. For example, ENFP is Extraversion Intuitive Feeling Perceiving, whic
its own set of characteristics, some like and some different from the other fifteen type
lar to Jung’s work in Psychological Types (1923), the MBTI addresses various combinat
each type, such as introverted-sensing or intuitive-thinking-perceiving. The MBTI allow
user to describe two people with the exact four-letter combination of preferences in ge
ties similar to both, yet accounts for the individual differences produced by variation o
extent (or strength) of each person’s preference. This echoes Jung’s belief that his typ
be used to describe groups of people as well as individuals (Jung, 1921/1923).
According to the companion manual to the MBTI, Introduction to Type (Briggs Myer
1998; Myers, Kirby, & Briggs Meyers, 2015), which was first published in 1970 and is c
in its seventh edition, the goal of the instrument is to foster self-understanding, enhan
learning and communication, assist with conflict management, and enhance relationsh
is a tool “with intent not to stereotype, but to allow understanding of individual prefere
(Jessup, 2002, p. 503). Between 1943 and 1975, the MBTI evolved through a number o
tions, spanning Forms A through F. In 1975 Consulting Psychologist Press acquired the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Myers-Briggs Personality Type Indicator 5
to sell the MBTI as a proprietary instrument (Pittenger, 1993), and it became readily a
for widespread use as Form G (McCaulley, 1990). In 1998, Form G underwent revision
was published as Form M, which can be administered by the publisher, by computer, o
using a self-scorable version. Additionally, two MBTI instruments that explore type mo
deeply are the Step II (first published as Form K in 1989 and subsequently revised as F
in 2001) and Step III (published in 2009). Step II explores differences within the same
and Step III is administered only by counselors specifically trained in the tool in one-on
sessions (Myers, McCaulley, Quenk, & Mitchell, 2009). There are currently four distinct
forms of the MBTI, each differing in its use and scoring: Form M and Form M self-scora
Step II Form Q, and Step III. The MBTI has a European version and has been translated
21 languages, including Chinese, German, Italian, Japanese, Norwegian, and Spanish (
& Briggs Foundation, 2016).
Most criticisms of the MBTI relate to the dichotomous nature of the instrument, its
translation of continuous scale scores into nominal categories of preference, and whet
reflects the theory on which it is based (Barbuto, 1997; Daisly, 2011; Pittenger, 1993;
1992). The forced-choice nature of the MBTI does not allow respondents to select a me
or neutral response (Barbuto, 1997); they must choose a response that places them in
preference or the other (either Extraversion or Introversion, Sensing or iNtuition, Think
or Feeling, Judging or Perceiving). Scoring for the MBTI reflects the most frequently se
side of the four dichotomies, which determines preference, reflected in the four-letter
bination that expresses overall type. Barbuto (1997) suggests that this nominal
the MBTI results deviates from Jung’s original theory. These observations lead to ques
regarding the validity and reliability of the MBTI (Zemke, 1992).
Key properties of an assessment tool such as the MBTI are validity and reliability. T
relate to aspects of its construction, evaluation, and documentation as described by th
dards for Educational and Psychological Testing (American Educational Research Asso
tion, American Psychological Association, & National Council on Measurement in Educa
tion, 2014). Validity is the degree to which evidence and theory support the interpreta
of scores for the proposed uses of the test. Construct validity refers to the extent to w
actually measures what the theory says it does. Reliability is the degree to which scor
individual or group are consistent over repeated administrations of the same test. Tes
reliability assesses the degree to which test scores are consistent from one test admin
to the next. Internal consistency reliability assesses the stability of results across item
test (American Educational Research Association, American Psychological Association,
National Council on Measurement in Education, 2014, chaps. 1, 2).
At present, no complete study has investigated the breadth of articles published ab
the MBTI or performed an in-depth analysis of the psychometric properties of the instr
ment as a whole or its various forms. This systematic review/meta-analysis seeks to in
our research question: in the adult population, is the MBTI a useful test in terms of con
to sell the MBTI as a proprietary instrument (Pittenger, 1993), and it became readily a
for widespread use as Form G (McCaulley, 1990). In 1998, Form G underwent revision
was published as Form M, which can be administered by the publisher, by computer, o
using a self-scorable version. Additionally, two MBTI instruments that explore type mo
deeply are the Step II (first published as Form K in 1989 and subsequently revised as F
in 2001) and Step III (published in 2009). Step II explores differences within the same
and Step III is administered only by counselors specifically trained in the tool in one-on
sessions (Myers, McCaulley, Quenk, & Mitchell, 2009). There are currently four distinct
forms of the MBTI, each differing in its use and scoring: Form M and Form M self-scora
Step II Form Q, and Step III. The MBTI has a European version and has been translated
21 languages, including Chinese, German, Italian, Japanese, Norwegian, and Spanish (
& Briggs Foundation, 2016).
Most criticisms of the MBTI relate to the dichotomous nature of the instrument, its
translation of continuous scale scores into nominal categories of preference, and whet
reflects the theory on which it is based (Barbuto, 1997; Daisly, 2011; Pittenger, 1993;
1992). The forced-choice nature of the MBTI does not allow respondents to select a me
or neutral response (Barbuto, 1997); they must choose a response that places them in
preference or the other (either Extraversion or Introversion, Sensing or iNtuition, Think
or Feeling, Judging or Perceiving). Scoring for the MBTI reflects the most frequently se
side of the four dichotomies, which determines preference, reflected in the four-letter
bination that expresses overall type. Barbuto (1997) suggests that this nominal
the MBTI results deviates from Jung’s original theory. These observations lead to ques
regarding the validity and reliability of the MBTI (Zemke, 1992).
Key properties of an assessment tool such as the MBTI are validity and reliability. T
relate to aspects of its construction, evaluation, and documentation as described by th
dards for Educational and Psychological Testing (American Educational Research Asso
tion, American Psychological Association, & National Council on Measurement in Educa
tion, 2014). Validity is the degree to which evidence and theory support the interpreta
of scores for the proposed uses of the test. Construct validity refers to the extent to w
actually measures what the theory says it does. Reliability is the degree to which scor
individual or group are consistent over repeated administrations of the same test. Tes
reliability assesses the degree to which test scores are consistent from one test admin
to the next. Internal consistency reliability assesses the stability of results across item
test (American Educational Research Association, American Psychological Association,
National Council on Measurement in Education, 2014, chaps. 1, 2).
At present, no complete study has investigated the breadth of articles published ab
the MBTI or performed an in-depth analysis of the psychometric properties of the instr
ment as a whole or its various forms. This systematic review/meta-analysis seeks to in
our research question: in the adult population, is the MBTI a useful test in terms of con
6 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
validity, test-retest reliability, and/or internal consistency reliability in determining per
ity preference in the areas of inward or outward focus (extraversion/introversion), info
tion processing (sensing/intuition), decision making (thinking/feeling), and organiz
(judging/perceiving)?
METHODS
Rationale for Methods
This systematic review of the key psychometric properties of the MBTI adhered
Cochrane guidelines and consisted of a priori identification of inclusion criteria,
determined our search strategy, followed by a two-phase process of critical appraisal o
cluded studies with the intent to extract data for analysis. Inclusion criteria for this rev
incorporated the Cochrane Collaboration guidelines (Cochrane Collaboration Diagnosti
Test Accuracy Working Group 2011; Deeks, Wisniewski, & Davenport, 2013; Higgins et
2011) and contained questions extracted from its tool for assessing risk of bias (Higgin
man, 2008), as well as strategies for systematic reviews proposed by Meline (2006) an
(1986). Some Cochrane criteria, such as those pertaining to randomized controlled tria
multiple-group designs, were not applicable and thus not used. Other recommended c
were incorporated into the rubric we applied to assess each article’s quality.
Inclusion Criteria and Rationale
The inclusion criteria for studies in this systematic review/meta-analysis were as follow
• The study was consistent with the research question.
• The study examined construct validity, test-retest reliability, and/or internal
consistency reliability for the MBTI as new data.
• Subjects in the study were adults (18 years or older).
• The study was written in English and published in a peer-reviewed journal
in 1975 or later, or the study was a dissertation written in English and pub-
lished in 2011 or later.
• Sample size and level of significance were reported or were obtainable from
study authors.
• The study authors expressed data for reliability as alpha coefficients, item-
total correlations, corrected item-total correlations, intraclass correlation
(ICC) coefficients, Pearson correlation coefficients, Spearman rank correla-
tion coefficients, or kappa coefficients; and/or expressed data for validity
as structural equation modeling, alpha coefficients, item-total correlations,
validity, test-retest reliability, and/or internal consistency reliability in determining per
ity preference in the areas of inward or outward focus (extraversion/introversion), info
tion processing (sensing/intuition), decision making (thinking/feeling), and organiz
(judging/perceiving)?
METHODS
Rationale for Methods
This systematic review of the key psychometric properties of the MBTI adhered
Cochrane guidelines and consisted of a priori identification of inclusion criteria,
determined our search strategy, followed by a two-phase process of critical appraisal o
cluded studies with the intent to extract data for analysis. Inclusion criteria for this rev
incorporated the Cochrane Collaboration guidelines (Cochrane Collaboration Diagnosti
Test Accuracy Working Group 2011; Deeks, Wisniewski, & Davenport, 2013; Higgins et
2011) and contained questions extracted from its tool for assessing risk of bias (Higgin
man, 2008), as well as strategies for systematic reviews proposed by Meline (2006) an
(1986). Some Cochrane criteria, such as those pertaining to randomized controlled tria
multiple-group designs, were not applicable and thus not used. Other recommended c
were incorporated into the rubric we applied to assess each article’s quality.
Inclusion Criteria and Rationale
The inclusion criteria for studies in this systematic review/meta-analysis were as follow
• The study was consistent with the research question.
• The study examined construct validity, test-retest reliability, and/or internal
consistency reliability for the MBTI as new data.
• Subjects in the study were adults (18 years or older).
• The study was written in English and published in a peer-reviewed journal
in 1975 or later, or the study was a dissertation written in English and pub-
lished in 2011 or later.
• Sample size and level of significance were reported or were obtainable from
study authors.
• The study authors expressed data for reliability as alpha coefficients, item-
total correlations, corrected item-total correlations, intraclass correlation
(ICC) coefficients, Pearson correlation coefficients, Spearman rank correla-
tion coefficients, or kappa coefficients; and/or expressed data for validity
as structural equation modeling, alpha coefficients, item-total correlations,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Myers-Briggs Personality Type Indicator 7
corrected-item total correlations, ICCs, Pearson r, Spearman r, kappa, or
item-level ICCs or factor analysis.
The publication date of 1975 or later was selected based on the assertion by McCa
ley (1990) that in 1975 the MBTI was readily accessible for use. We elected to study a
the three forms of the MBTI (Form F, G, or M) that were in use from 1975 to the presen
day, since they all measure the same theoretical construct and are simply refinements
instrument. We did not use any articles related to the MBTI Step II or Step III instrume
because these are different versions of the MBTI that are scored only through the pub
or by a certified MBTI counselor, and more pragmatically, no studies were found when
conducted our literature search. Given the potential time lapse between completing a
sertation and submitting it for publication, we selected five years as sufficient time to
dissertation that was completed longer than five years ago likely will not have been ac
for publication due to failure to meet certain quality thresholds (Meline, 2006). If a stu
not report its level of significance (alpha) and we could not confirm it with study autho
excluded it from analysis.
Search Strategy
The comprehensive literature search was conducted by a librarian with a master of lib
information science degree and who is a distinguished member of the Academy of Hea
Information. Databases searched were Ovid MEDLINE®, OVID OLDMEDLINE®, OVID
MEDLINE® In-Process & Other Non-Indexed Citations, OVID MEDLINE® Without Re-
visions, EMBASE+EMBASE CLASSIC, ERIC, PsycINFO, and HEALTH AND PSYCHO-
SOCIAL INSTRUMENTS (HAPI). Search terms used were Myers-Briggs, validity, reliabilit
and statistics. Results were limited to articles published in 1975 or later on adult popu
(older than 18 years). When possible, MeSH terms and descriptors were used and exp
Truncation was employed for a maximum number of results. Reference results from ea
database were reviewed, and the authors examined reference lists of individual article
ditional studies. A hand search was conducted on numerous compendiums of psychom
assessment and measurement for additional studies. The literature search produced 2
tential studies, which were assembled into the EndNote (Clarivate Analytics 2014) refe
management software system.
Study Selection Process
The application of this study’s inclusion criteria occurred in two phases, depicted in the
diagram of Figure 1. Phase I involved independent and blinded assessments of the ass
abstracts by two of the authors (MI and KR), applying the first four inclusion criteria. If
corrected-item total correlations, ICCs, Pearson r, Spearman r, kappa, or
item-level ICCs or factor analysis.
The publication date of 1975 or later was selected based on the assertion by McCa
ley (1990) that in 1975 the MBTI was readily accessible for use. We elected to study a
the three forms of the MBTI (Form F, G, or M) that were in use from 1975 to the presen
day, since they all measure the same theoretical construct and are simply refinements
instrument. We did not use any articles related to the MBTI Step II or Step III instrume
because these are different versions of the MBTI that are scored only through the pub
or by a certified MBTI counselor, and more pragmatically, no studies were found when
conducted our literature search. Given the potential time lapse between completing a
sertation and submitting it for publication, we selected five years as sufficient time to
dissertation that was completed longer than five years ago likely will not have been ac
for publication due to failure to meet certain quality thresholds (Meline, 2006). If a stu
not report its level of significance (alpha) and we could not confirm it with study autho
excluded it from analysis.
Search Strategy
The comprehensive literature search was conducted by a librarian with a master of lib
information science degree and who is a distinguished member of the Academy of Hea
Information. Databases searched were Ovid MEDLINE®, OVID OLDMEDLINE®, OVID
MEDLINE® In-Process & Other Non-Indexed Citations, OVID MEDLINE® Without Re-
visions, EMBASE+EMBASE CLASSIC, ERIC, PsycINFO, and HEALTH AND PSYCHO-
SOCIAL INSTRUMENTS (HAPI). Search terms used were Myers-Briggs, validity, reliabilit
and statistics. Results were limited to articles published in 1975 or later on adult popu
(older than 18 years). When possible, MeSH terms and descriptors were used and exp
Truncation was employed for a maximum number of results. Reference results from ea
database were reviewed, and the authors examined reference lists of individual article
ditional studies. A hand search was conducted on numerous compendiums of psychom
assessment and measurement for additional studies. The literature search produced 2
tential studies, which were assembled into the EndNote (Clarivate Analytics 2014) refe
management software system.
Study Selection Process
The application of this study’s inclusion criteria occurred in two phases, depicted in the
diagram of Figure 1. Phase I involved independent and blinded assessments of the ass
abstracts by two of the authors (MI and KR), applying the first four inclusion criteria. If
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
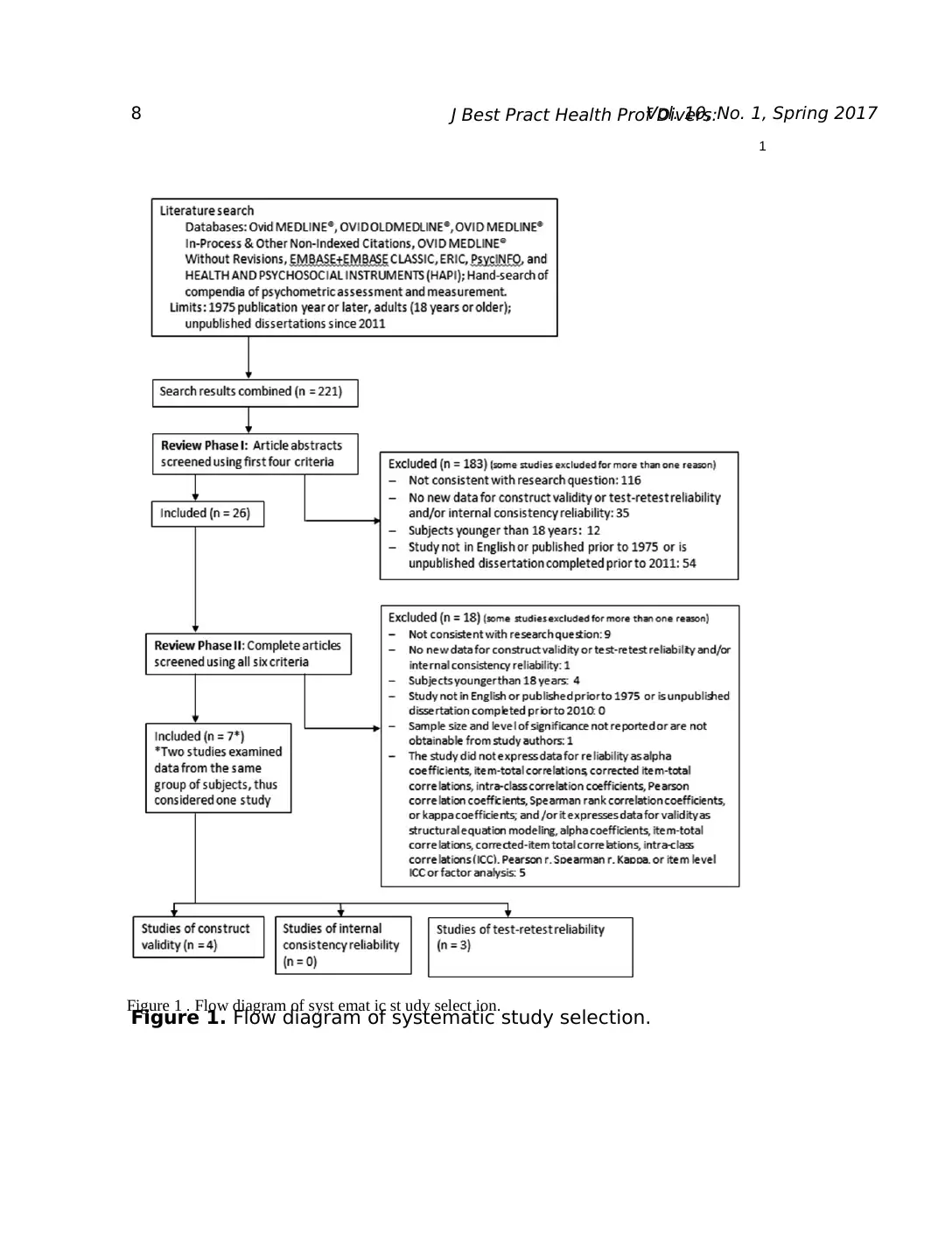
Figure 1. Flow diagram of systematic study selection.
1
Figure 1 . Flow diagram of syst emat ic st udy select ion.
Figure 1. Flow diagram of systematic study selection.
1
Figure 1 . Flow diagram of syst emat ic st udy select ion.
Myers-Briggs Personality Type Indicator 9
study did not meet one or more of the criteria, the reviewer identified it as excluded fr
the review. During this phase of the appraisal process, the two assessors agreed on 24
for inclusion and 185 for exclusion, for an agreement of 94.57%. They differed in opini
on 12 studies, for which the remaining author (CC) served to break the tie. If the revie
were unsure that a study met one or more criteria and no other reasons for exclusion
they then retained the study for Phase II, which involved review of the entire article. In
26 abstracts were included for the second phase of appraisal.
Prior to Phase II, a graduate assistant obtained complete copies of the articles, rem
all identifying information about the authors, placed them in random order, and assign
study number. Both reviewers then screened each study, applying all six of the inclusi
One study (Levy & Padilla, 1982) did not report an alpha level. The reviewers contacte
authors and received a response from one (Padilla) who was unable to provide the alp
for this study; therefore, it was excluded. During the process both reviewers conferred
studies; however, their initial determinations were in complete agreement. Of the 26 s
in Phase II, both reviewers excluded 17 studies and included 8, for 96.15% agreement
third author broke the tie on the only study (Tzeng, Ware, & Bharadwaj, 1991) on whic
reviewers disagreed, determining that is should be excluded, bringing the total exclud
Nearly half of the included studies did not report the specific ages of subjects; howeve
report them as “college-age students” or similar description. The reviewers agreed tha
the criterion that the subjects were adults. Once the articles were unblinded, the revie
covered that two of them (Thompson & Borrello, 1986a, 1986b) analyzed data from th
study and both reported on construct validity of the MBTI, with the second study (Thom
& Borrello, 1986b) reporting a second-order factor analysis. After conferring, both revi
agreed that these studies met the inclusion criteria but decided to consider them as o
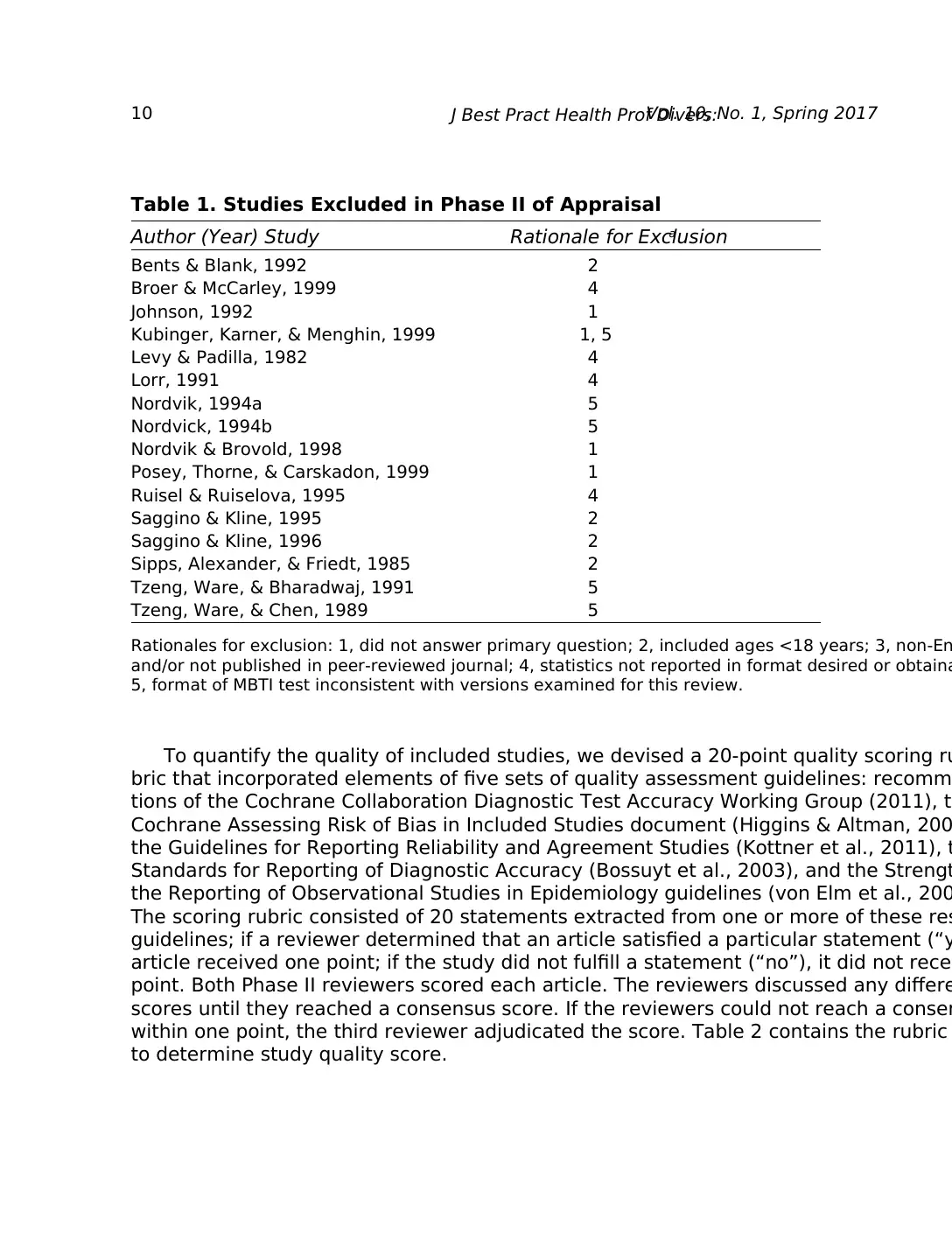
study for analysis. Excluded studies with rationale are listed in Table 1.
Data Abstraction and Quality-of-Study Score
Descriptive characteristics of each study were abstracted during the Phase II review p
for use in description and sensitivity analysis as follows:
• Characteristics of the article: author, journal, year published, publication
type
• Characteristics of the MBTI: form used, translation into another language,
format or delivery method
• Characteristics of the sample: age, gender, race/ethnicity, education level,
country of delivery, sample size
• Characteristics of the study: primary question, study design, sampling pro-
cedures, statistics collected
study did not meet one or more of the criteria, the reviewer identified it as excluded fr
the review. During this phase of the appraisal process, the two assessors agreed on 24
for inclusion and 185 for exclusion, for an agreement of 94.57%. They differed in opini
on 12 studies, for which the remaining author (CC) served to break the tie. If the revie
were unsure that a study met one or more criteria and no other reasons for exclusion
they then retained the study for Phase II, which involved review of the entire article. In
26 abstracts were included for the second phase of appraisal.
Prior to Phase II, a graduate assistant obtained complete copies of the articles, rem
all identifying information about the authors, placed them in random order, and assign
study number. Both reviewers then screened each study, applying all six of the inclusi
One study (Levy & Padilla, 1982) did not report an alpha level. The reviewers contacte
authors and received a response from one (Padilla) who was unable to provide the alp
for this study; therefore, it was excluded. During the process both reviewers conferred
studies; however, their initial determinations were in complete agreement. Of the 26 s
in Phase II, both reviewers excluded 17 studies and included 8, for 96.15% agreement
third author broke the tie on the only study (Tzeng, Ware, & Bharadwaj, 1991) on whic
reviewers disagreed, determining that is should be excluded, bringing the total exclud
Nearly half of the included studies did not report the specific ages of subjects; howeve
report them as “college-age students” or similar description. The reviewers agreed tha
the criterion that the subjects were adults. Once the articles were unblinded, the revie
covered that two of them (Thompson & Borrello, 1986a, 1986b) analyzed data from th
study and both reported on construct validity of the MBTI, with the second study (Thom
& Borrello, 1986b) reporting a second-order factor analysis. After conferring, both revi
agreed that these studies met the inclusion criteria but decided to consider them as o
study for analysis. Excluded studies with rationale are listed in Table 1.
Data Abstraction and Quality-of-Study Score
Descriptive characteristics of each study were abstracted during the Phase II review p
for use in description and sensitivity analysis as follows:
• Characteristics of the article: author, journal, year published, publication
type
• Characteristics of the MBTI: form used, translation into another language,
format or delivery method
• Characteristics of the sample: age, gender, race/ethnicity, education level,
country of delivery, sample size
• Characteristics of the study: primary question, study design, sampling pro-
cedures, statistics collected
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
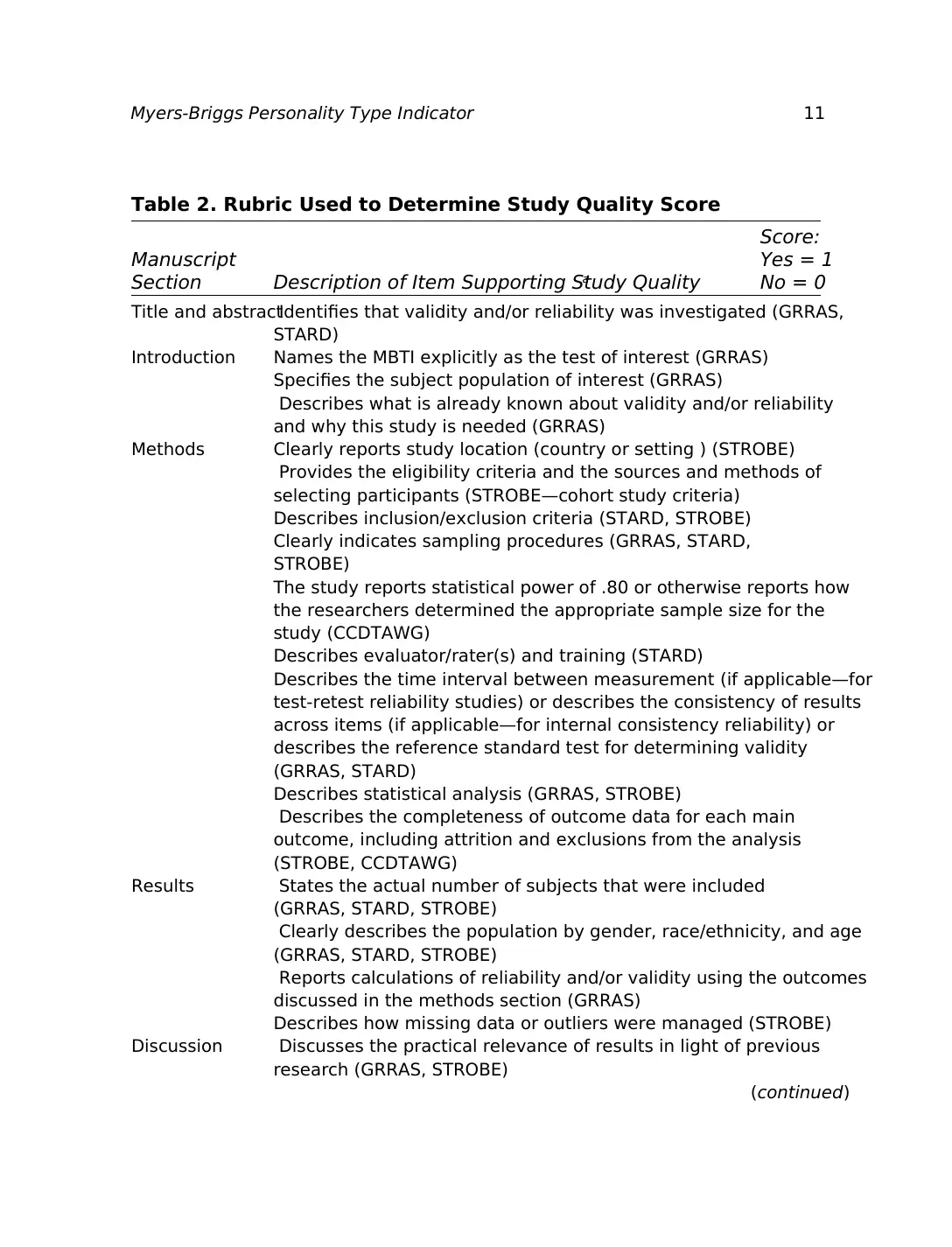
To quantify the quality of included studies, we devised a 20-point quality scoring ru
bric that incorporated elements of five sets of quality assessment guidelines: recomm
tions of the Cochrane Collaboration Diagnostic Test Accuracy Working Group (2011), th
Cochrane Assessing Risk of Bias in Included Studies document (Higgins & Altman, 200
the Guidelines for Reporting Reliability and Agreement Studies (Kottner et al., 2011), t
Standards for Reporting of Diagnostic Accuracy (Bossuyt et al., 2003), and the Strengt
the Reporting of Observational Studies in Epidemiology guidelines (von Elm et al., 200
The scoring rubric consisted of 20 statements extracted from one or more of these res
guidelines; if a reviewer determined that an article satisfied a particular statement (“y
article received one point; if the study did not fulfill a statement (“no”), it did not recei
point. Both Phase II reviewers scored each article. The reviewers discussed any differe
scores until they reached a consensus score. If the reviewers could not reach a consen
within one point, the third reviewer adjudicated the score. Table 2 contains the rubric
to determine study quality score.
Table 1. Studies Excluded in Phase II of Appraisal
Author (Year) Study Rationale for Exclusiona
Bents & Blank, 1992 2
Broer & McCarley, 1999 4
Johnson, 1992 1
Kubinger, Karner, & Menghin, 1999 1, 5
Levy & Padilla, 1982 4
Lorr, 1991 4
Nordvik, 1994a 5
Nordvick, 1994b 5
Nordvik & Brovold, 1998 1
Posey, Thorne, & Carskadon, 1999 1
Ruisel & Ruiselova, 1995 4
Saggino & Kline, 1995 2
Saggino & Kline, 1996 2
Sipps, Alexander, & Friedt, 1985 2
Tzeng, Ware, & Bharadwaj, 1991 5
Tzeng, Ware, & Chen, 1989 5
Rationales for exclusion: 1, did not answer primary question; 2, included ages <18 years; 3, non-En
and/or not published in peer-reviewed journal; 4, statistics not reported in format desired or obtaina
5, format of MBTI test inconsistent with versions examined for this review.
To quantify the quality of included studies, we devised a 20-point quality scoring ru
bric that incorporated elements of five sets of quality assessment guidelines: recomm
tions of the Cochrane Collaboration Diagnostic Test Accuracy Working Group (2011), th
Cochrane Assessing Risk of Bias in Included Studies document (Higgins & Altman, 200
the Guidelines for Reporting Reliability and Agreement Studies (Kottner et al., 2011), t
Standards for Reporting of Diagnostic Accuracy (Bossuyt et al., 2003), and the Strengt
the Reporting of Observational Studies in Epidemiology guidelines (von Elm et al., 200
The scoring rubric consisted of 20 statements extracted from one or more of these res
guidelines; if a reviewer determined that an article satisfied a particular statement (“y
article received one point; if the study did not fulfill a statement (“no”), it did not recei
point. Both Phase II reviewers scored each article. The reviewers discussed any differe
scores until they reached a consensus score. If the reviewers could not reach a consen
within one point, the third reviewer adjudicated the score. Table 2 contains the rubric
to determine study quality score.
Table 1. Studies Excluded in Phase II of Appraisal
Author (Year) Study Rationale for Exclusiona
Bents & Blank, 1992 2
Broer & McCarley, 1999 4
Johnson, 1992 1
Kubinger, Karner, & Menghin, 1999 1, 5
Levy & Padilla, 1982 4
Lorr, 1991 4
Nordvik, 1994a 5
Nordvick, 1994b 5
Nordvik & Brovold, 1998 1
Posey, Thorne, & Carskadon, 1999 1
Ruisel & Ruiselova, 1995 4
Saggino & Kline, 1995 2
Saggino & Kline, 1996 2
Sipps, Alexander, & Friedt, 1985 2
Tzeng, Ware, & Bharadwaj, 1991 5
Tzeng, Ware, & Chen, 1989 5
Rationales for exclusion: 1, did not answer primary question; 2, included ages <18 years; 3, non-En
and/or not published in peer-reviewed journal; 4, statistics not reported in format desired or obtaina
5, format of MBTI test inconsistent with versions examined for this review.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Myers-Briggs Personality Type Indicator 11
Table 2. Rubric Used to Determine Study Quality Score
Score:
Manuscript Yes = 1
Section Description of Item Supporting Study Qualitya No = 0
Title and abstractIdentifies that validity and/or reliability was investigated (GRRAS,
STARD)
Introduction Names the MBTI explicitly as the test of interest (GRRAS)
Specifies the subject population of interest (GRRAS)
Describes what is already known about validity and/or reliability
and why this study is needed (GRRAS)
Methods Clearly reports study location (country or setting ) (STROBE)
Provides the eligibility criteria and the sources and methods of
selecting participants (STROBE—cohort study criteria)
Describes inclusion/exclusion criteria (STARD, STROBE)
Clearly indicates sampling procedures (GRRAS, STARD,
STROBE)
The study reports statistical power of .80 or otherwise reports how
the researchers determined the appropriate sample size for the
study (CCDTAWG)
Describes evaluator/rater(s) and training (STARD)
Describes the time interval between measurement (if applicable—for
test-retest reliability studies) or describes the consistency of results
across items (if applicable—for internal consistency reliability) or
describes the reference standard test for determining validity
(GRRAS, STARD)
Describes statistical analysis (GRRAS, STROBE)
Describes the completeness of outcome data for each main
outcome, including attrition and exclusions from the analysis
(STROBE, CCDTAWG)
Results States the actual number of subjects that were included
(GRRAS, STARD, STROBE)
Clearly describes the population by gender, race/ethnicity, and age
(GRRAS, STARD, STROBE)
Reports calculations of reliability and/or validity using the outcomes
discussed in the methods section (GRRAS)
Describes how missing data or outliers were managed (STROBE)
Discussion Discusses the practical relevance of results in light of previous
research (GRRAS, STROBE)
(continued)
Table 2. Rubric Used to Determine Study Quality Score
Score:
Manuscript Yes = 1
Section Description of Item Supporting Study Qualitya No = 0
Title and abstractIdentifies that validity and/or reliability was investigated (GRRAS,
STARD)
Introduction Names the MBTI explicitly as the test of interest (GRRAS)
Specifies the subject population of interest (GRRAS)
Describes what is already known about validity and/or reliability
and why this study is needed (GRRAS)
Methods Clearly reports study location (country or setting ) (STROBE)
Provides the eligibility criteria and the sources and methods of
selecting participants (STROBE—cohort study criteria)
Describes inclusion/exclusion criteria (STARD, STROBE)
Clearly indicates sampling procedures (GRRAS, STARD,
STROBE)
The study reports statistical power of .80 or otherwise reports how
the researchers determined the appropriate sample size for the
study (CCDTAWG)
Describes evaluator/rater(s) and training (STARD)
Describes the time interval between measurement (if applicable—for
test-retest reliability studies) or describes the consistency of results
across items (if applicable—for internal consistency reliability) or
describes the reference standard test for determining validity
(GRRAS, STARD)
Describes statistical analysis (GRRAS, STROBE)
Describes the completeness of outcome data for each main
outcome, including attrition and exclusions from the analysis
(STROBE, CCDTAWG)
Results States the actual number of subjects that were included
(GRRAS, STARD, STROBE)
Clearly describes the population by gender, race/ethnicity, and age
(GRRAS, STARD, STROBE)
Reports calculations of reliability and/or validity using the outcomes
discussed in the methods section (GRRAS)
Describes how missing data or outliers were managed (STROBE)
Discussion Discusses the practical relevance of results in light of previous
research (GRRAS, STROBE)
(continued)
12 J Best Pract Health Prof Divers:Vol. 10, No. 1, Spring 2017
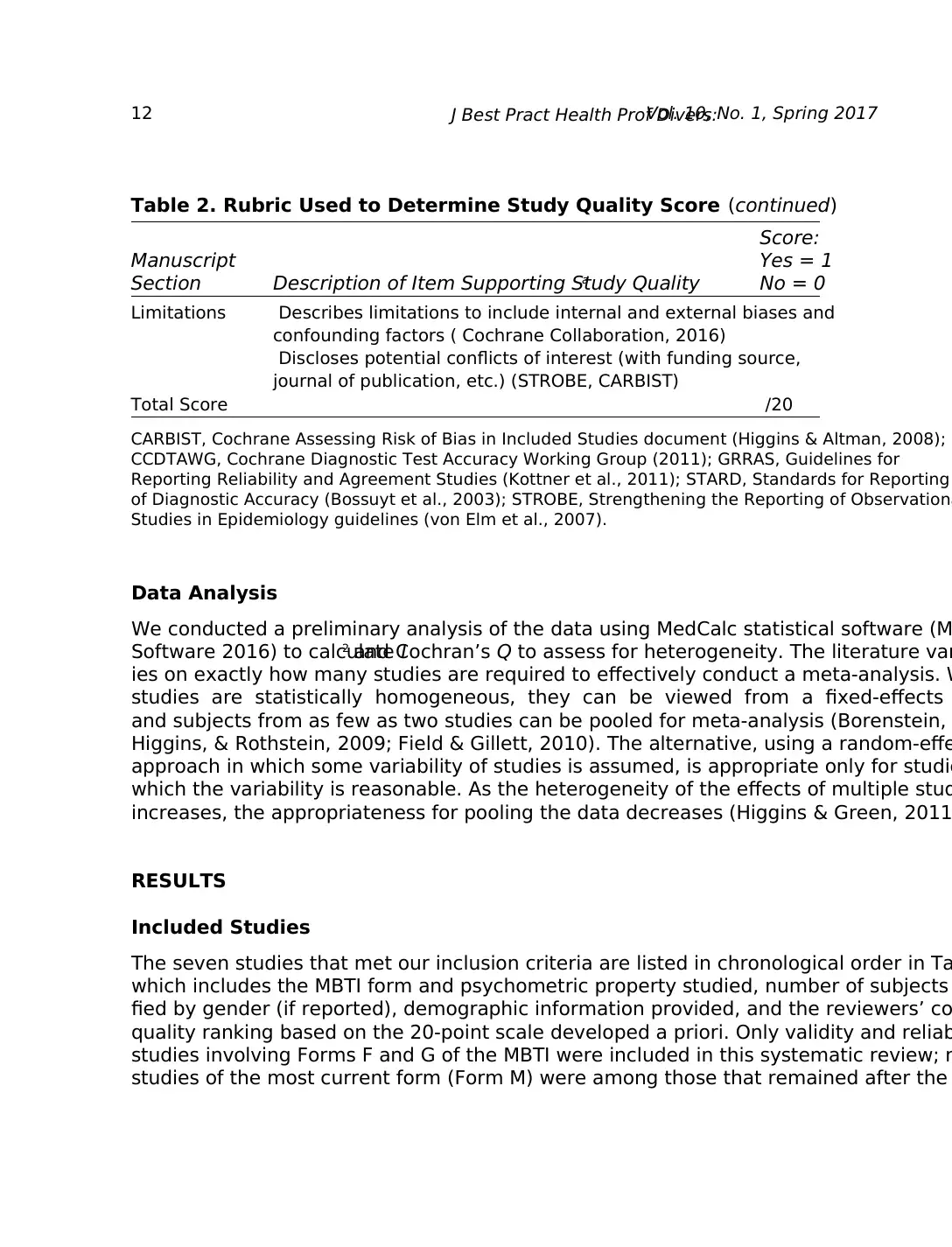
Data Analysis
We conducted a preliminary analysis of the data using MedCalc statistical software (M
Software 2016) to calculate I2 and Cochran’s Q to assess for heterogeneity. The literature var
ies on exactly how many studies are required to effectively conduct a meta-analysis. W
studies are statistically homogeneous, they can be viewed from a fixed-effects
and subjects from as few as two studies can be pooled for meta-analysis (Borenstein,
Higgins, & Rothstein, 2009; Field & Gillett, 2010). The alternative, using a random-effe
approach in which some variability of studies is assumed, is appropriate only for studie
which the variability is reasonable. As the heterogeneity of the effects of multiple stud
increases, the appropriateness for pooling the data decreases (Higgins & Green, 2011
RESULTS
Included Studies
The seven studies that met our inclusion criteria are listed in chronological order in Ta
which includes the MBTI form and psychometric property studied, number of subjects
fied by gender (if reported), demographic information provided, and the reviewers’ co
quality ranking based on the 20-point scale developed a priori. Only validity and reliab
studies involving Forms F and G of the MBTI were included in this systematic review; n
studies of the most current form (Form M) were among those that remained after the
Table 2. Rubric Used to Determine Study Quality Score (continued)
Score:
Manuscript Yes = 1
Section Description of Item Supporting Study Qualitya No = 0
Limitations Describes limitations to include internal and external biases and
confounding factors ( Cochrane Collaboration, 2016)
Discloses potential conflicts of interest (with funding source,
journal of publication, etc.) (STROBE, CARBIST)
Total Score /20
CARBIST, Cochrane Assessing Risk of Bias in Included Studies document (Higgins & Altman, 2008);
CCDTAWG, Cochrane Diagnostic Test Accuracy Working Group (2011); GRRAS, Guidelines for
Reporting Reliability and Agreement Studies (Kottner et al., 2011); STARD, Standards for Reporting
of Diagnostic Accuracy (Bossuyt et al., 2003); STROBE, Strengthening the Reporting of Observationa
Studies in Epidemiology guidelines (von Elm et al., 2007).
Data Analysis
We conducted a preliminary analysis of the data using MedCalc statistical software (M
Software 2016) to calculate I2 and Cochran’s Q to assess for heterogeneity. The literature var
ies on exactly how many studies are required to effectively conduct a meta-analysis. W
studies are statistically homogeneous, they can be viewed from a fixed-effects
and subjects from as few as two studies can be pooled for meta-analysis (Borenstein,
Higgins, & Rothstein, 2009; Field & Gillett, 2010). The alternative, using a random-effe
approach in which some variability of studies is assumed, is appropriate only for studie
which the variability is reasonable. As the heterogeneity of the effects of multiple stud
increases, the appropriateness for pooling the data decreases (Higgins & Green, 2011
RESULTS
Included Studies
The seven studies that met our inclusion criteria are listed in chronological order in Ta
which includes the MBTI form and psychometric property studied, number of subjects
fied by gender (if reported), demographic information provided, and the reviewers’ co
quality ranking based on the 20-point scale developed a priori. Only validity and reliab
studies involving Forms F and G of the MBTI were included in this systematic review; n
studies of the most current form (Form M) were among those that remained after the
Table 2. Rubric Used to Determine Study Quality Score (continued)
Score:
Manuscript Yes = 1
Section Description of Item Supporting Study Qualitya No = 0
Limitations Describes limitations to include internal and external biases and
confounding factors ( Cochrane Collaboration, 2016)
Discloses potential conflicts of interest (with funding source,
journal of publication, etc.) (STROBE, CARBIST)
Total Score /20
CARBIST, Cochrane Assessing Risk of Bias in Included Studies document (Higgins & Altman, 2008);
CCDTAWG, Cochrane Diagnostic Test Accuracy Working Group (2011); GRRAS, Guidelines for
Reporting Reliability and Agreement Studies (Kottner et al., 2011); STARD, Standards for Reporting
of Diagnostic Accuracy (Bossuyt et al., 2003); STROBE, Strengthening the Reporting of Observationa
Studies in Epidemiology guidelines (von Elm et al., 2007).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 28
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.