MEDI6295: Managing Aggression with Psychotherapeutic Interventions
VerifiedAdded on 2023/04/10
|6
|1736
|361
Report
AI Summary
This report discusses the effectiveness of counseling and psychotherapeutic treatments for aggressive intervention, focusing on a male perpetrator of child maltreatment. It examines psychotherapeutic interventions derived from psychiatry and human psychology, using a real-world clinical example to emphasize the effectiveness of cognitive behavioral counseling therapy. The intervention involves a four-week therapy program, incorporating elements of randomized control trials (RCT) and addressing the patient's mental and emotional state. The process includes identifying triggers, managing arousal sequences, and employing Rational Emotive Behavior Therapy (REBT) and Dialectical Behavior Therapy (DBT) to promote emotional balance and realistic thought processes. The report concludes by highlighting the potential positive outcomes of such interventions, emphasizing the importance of family support, and acknowledging the limitations of the study, while suggesting further research dimensions. Desklib provides a platform to access similar solved assignments and study resources.
Running Head: PSYCHOLOGY
Background
When it comes to abuse and assault, children and women are the most victimised ones in
the families Frazier and Vela (2). In most cases both the male and female perpetrators abuse their
children and physical violence is the ultimate result of their aggressive personalities. According
to Franzini, Broggi, Cordella, Dones and Messina (1) family violence prevention has been one of
the major health priorities in recent times and is being prioritised globally. Domestic violence is
the abuse by one person on the other in a domestic setting like marriage, family and co-
habitation Franzini, Broggi, Cordella, Dones and Messina (1). Scientific evidence suggests that
symptoms like anxiety, depression, chronic pain, substance abuse and post- traumatic stress
disorder are all linked to family violence and efficacy and effectiveness play major roles in its
intervention. Efficacy is the quality of being effective, here it is the ability of the intervention to
produce the intended results. Effectiveness is a measure of the degree to which the targeted
problems are solved Frazier and Vela (2).
Aggressive Intervention
In this paper the counselling psychotherapeutic treatment for aggressive intervention and
its effectiveness is considered for the offender. Here necessary intervention of the male
perpetrator for child-maltreatment is discussed. In this type of intervention, it is assumed that
family violence is a result of personal dysfunction and target groups are independent of age and
includes both men, women and children. Frazier and Vela (2) opined that psychotherapeutic
treatments intervention are mainly derived from disciplines of psychiatry and human psychology.
The randomised control trial (RCT) is used to test both efficacy and effectiveness of clinical
interventions but here effectiveness of a real-world clinical setting is emphasised and cause-
effect relationship is evaluated in consideration of the case. In RCT people in the trial process are
randomly allocated to groups of either treatment under investigation or standard treatment
groups. The psychotherapeutic intervention of counselling aims at treating the mental and
emotional state of the offender. According to Hillis, Mercy and Saul (3) the counselling
programs are ‘person-centred’ focusing on individual interaction between the perpetrator and the
specialised trained psychologist. The ultimate goal is to rectify the aggressive behavioural
approach of the offender in a slow and steady manner.
Research and description of the intervention
Background
When it comes to abuse and assault, children and women are the most victimised ones in
the families Frazier and Vela (2). In most cases both the male and female perpetrators abuse their
children and physical violence is the ultimate result of their aggressive personalities. According
to Franzini, Broggi, Cordella, Dones and Messina (1) family violence prevention has been one of
the major health priorities in recent times and is being prioritised globally. Domestic violence is
the abuse by one person on the other in a domestic setting like marriage, family and co-
habitation Franzini, Broggi, Cordella, Dones and Messina (1). Scientific evidence suggests that
symptoms like anxiety, depression, chronic pain, substance abuse and post- traumatic stress
disorder are all linked to family violence and efficacy and effectiveness play major roles in its
intervention. Efficacy is the quality of being effective, here it is the ability of the intervention to
produce the intended results. Effectiveness is a measure of the degree to which the targeted
problems are solved Frazier and Vela (2).
Aggressive Intervention
In this paper the counselling psychotherapeutic treatment for aggressive intervention and
its effectiveness is considered for the offender. Here necessary intervention of the male
perpetrator for child-maltreatment is discussed. In this type of intervention, it is assumed that
family violence is a result of personal dysfunction and target groups are independent of age and
includes both men, women and children. Frazier and Vela (2) opined that psychotherapeutic
treatments intervention are mainly derived from disciplines of psychiatry and human psychology.
The randomised control trial (RCT) is used to test both efficacy and effectiveness of clinical
interventions but here effectiveness of a real-world clinical setting is emphasised and cause-
effect relationship is evaluated in consideration of the case. In RCT people in the trial process are
randomly allocated to groups of either treatment under investigation or standard treatment
groups. The psychotherapeutic intervention of counselling aims at treating the mental and
emotional state of the offender. According to Hillis, Mercy and Saul (3) the counselling
programs are ‘person-centred’ focusing on individual interaction between the perpetrator and the
specialised trained psychologist. The ultimate goal is to rectify the aggressive behavioural
approach of the offender in a slow and steady manner.
Research and description of the intervention
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2PSYCHOLOGY: AGGRESSIVE PERSONALITY
The intervention is based on a real-world example in clinical setting where effectiveness
of the intervention is focused upon. Mr. Jane is a financial consultant in ABS consultancy. He
has been married for almost 7 years and has 5 years son. In recent times his wife has seen his
behavioural changes and is surprised to notice that his aggression has increased tremendously.
He rebukes his son for petty reasons and even bit him up. In extreme cases he throws objects on
his son as well and has caused him several physical injuries. He is also an alcoholic. When his
wife and mother try to stop him, he thrashes them as well. In these circumstances, the family
physician recommended him to go for a counselling session and have psychotherapeutic
interventions. Ideally, for preliminary mental issues, first, medications are prescribed by the
psychotherapist and then the talk therapy or the positive activity intervention is provided
afterwards. But when the medications have no long-term effect then counselling sessions is
recommended. In this case a 4-week cognitive behavioural counselling therapy is recommended
for Mr. Jane. The four phases of RCT namely enrolment, intervention allocation, follow-up and
data analysis are used in the clinical trial process. Also, a contract agreement is being signed
before the therapy session.
In the first session of the cognitive behavioural counselling therapy, Mr. Jane was interacted with
a general conversation. In recent times he is under tremendous work pressure and is suffering
from depression. He is also been socially isolated. The unresolved and unconscious conflicts
from within is causing him some unwanted behavioural changes and when he cannot control his
stress and anxiety, he became aggressive. The psychotherapist also interacted with his family
members and friends to know about his current behavioural patterns. Deeper research on the case
provided the facts that he had childhood problem of stress management. The stress conditions
remained suppressed for long because his work life was good and balanced. But after joining
ABS Consultancy he again faced the stress burden and his behavioural changes were
predominant. His childhood trauma is reflected back and his son has become the victim of his
aggressive personality.
The process of de-escalating aggressive behaviour is focused upon in the next session.
Four incident simulation elements for violence are arranged that includes the target (the client), a
weapon (an object), a trigger (initiating stimuli) and an arousal state (the emotional and
psychological state that precede violence). The escalation and de-escalation of the violent
The intervention is based on a real-world example in clinical setting where effectiveness
of the intervention is focused upon. Mr. Jane is a financial consultant in ABS consultancy. He
has been married for almost 7 years and has 5 years son. In recent times his wife has seen his
behavioural changes and is surprised to notice that his aggression has increased tremendously.
He rebukes his son for petty reasons and even bit him up. In extreme cases he throws objects on
his son as well and has caused him several physical injuries. He is also an alcoholic. When his
wife and mother try to stop him, he thrashes them as well. In these circumstances, the family
physician recommended him to go for a counselling session and have psychotherapeutic
interventions. Ideally, for preliminary mental issues, first, medications are prescribed by the
psychotherapist and then the talk therapy or the positive activity intervention is provided
afterwards. But when the medications have no long-term effect then counselling sessions is
recommended. In this case a 4-week cognitive behavioural counselling therapy is recommended
for Mr. Jane. The four phases of RCT namely enrolment, intervention allocation, follow-up and
data analysis are used in the clinical trial process. Also, a contract agreement is being signed
before the therapy session.
In the first session of the cognitive behavioural counselling therapy, Mr. Jane was interacted with
a general conversation. In recent times he is under tremendous work pressure and is suffering
from depression. He is also been socially isolated. The unresolved and unconscious conflicts
from within is causing him some unwanted behavioural changes and when he cannot control his
stress and anxiety, he became aggressive. The psychotherapist also interacted with his family
members and friends to know about his current behavioural patterns. Deeper research on the case
provided the facts that he had childhood problem of stress management. The stress conditions
remained suppressed for long because his work life was good and balanced. But after joining
ABS Consultancy he again faced the stress burden and his behavioural changes were
predominant. His childhood trauma is reflected back and his son has become the victim of his
aggressive personality.
The process of de-escalating aggressive behaviour is focused upon in the next session.
Four incident simulation elements for violence are arranged that includes the target (the client), a
weapon (an object), a trigger (initiating stimuli) and an arousal state (the emotional and
psychological state that precede violence). The escalation and de-escalation of the violent
3PSYCHOLOGY: AGGRESSIVE PERSONALITY
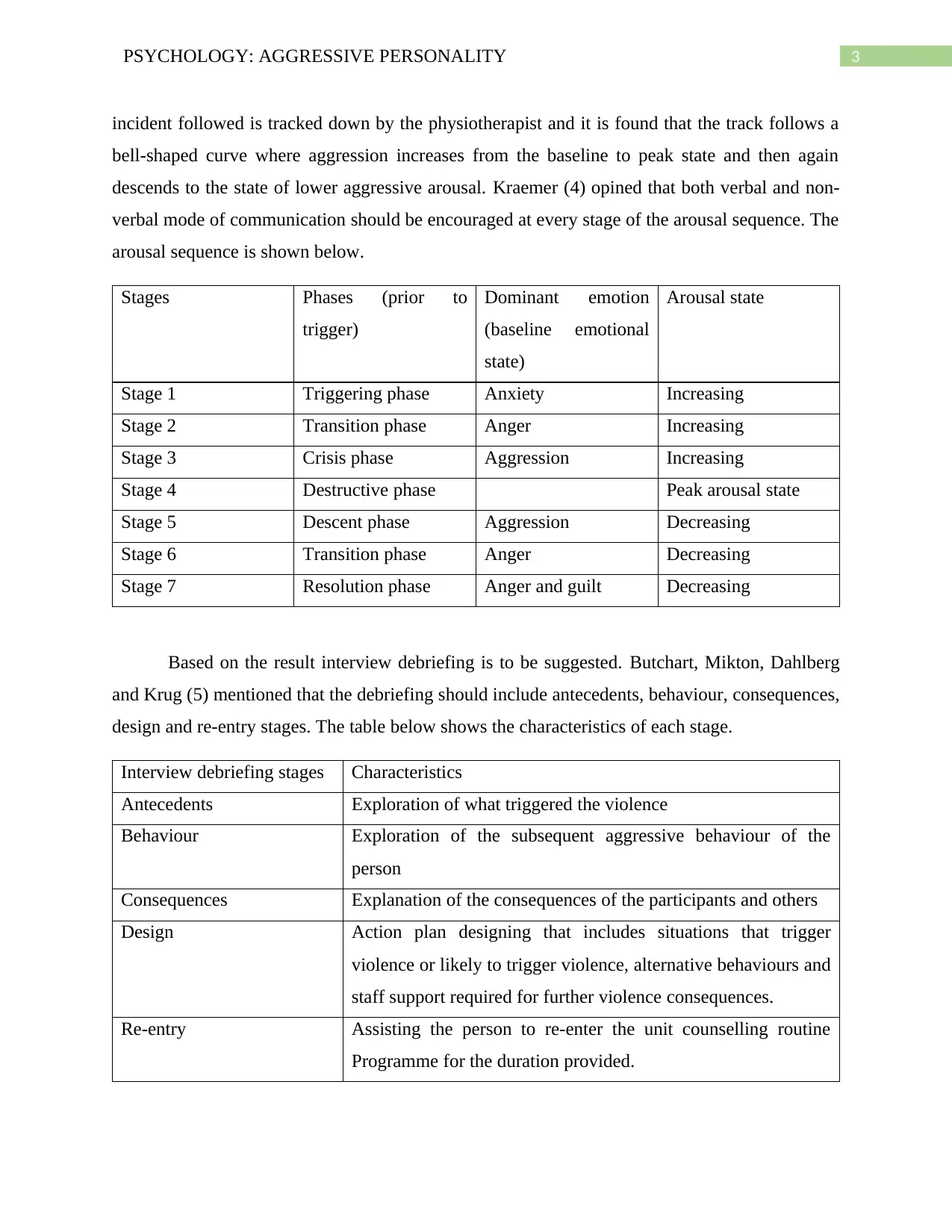
incident followed is tracked down by the physiotherapist and it is found that the track follows a
bell-shaped curve where aggression increases from the baseline to peak state and then again
descends to the state of lower aggressive arousal. Kraemer (4) opined that both verbal and non-
verbal mode of communication should be encouraged at every stage of the arousal sequence. The
arousal sequence is shown below.
Stages Phases (prior to
trigger)
Dominant emotion
(baseline emotional
state)
Arousal state
Stage 1 Triggering phase Anxiety Increasing
Stage 2 Transition phase Anger Increasing
Stage 3 Crisis phase Aggression Increasing
Stage 4 Destructive phase Peak arousal state
Stage 5 Descent phase Aggression Decreasing
Stage 6 Transition phase Anger Decreasing
Stage 7 Resolution phase Anger and guilt Decreasing
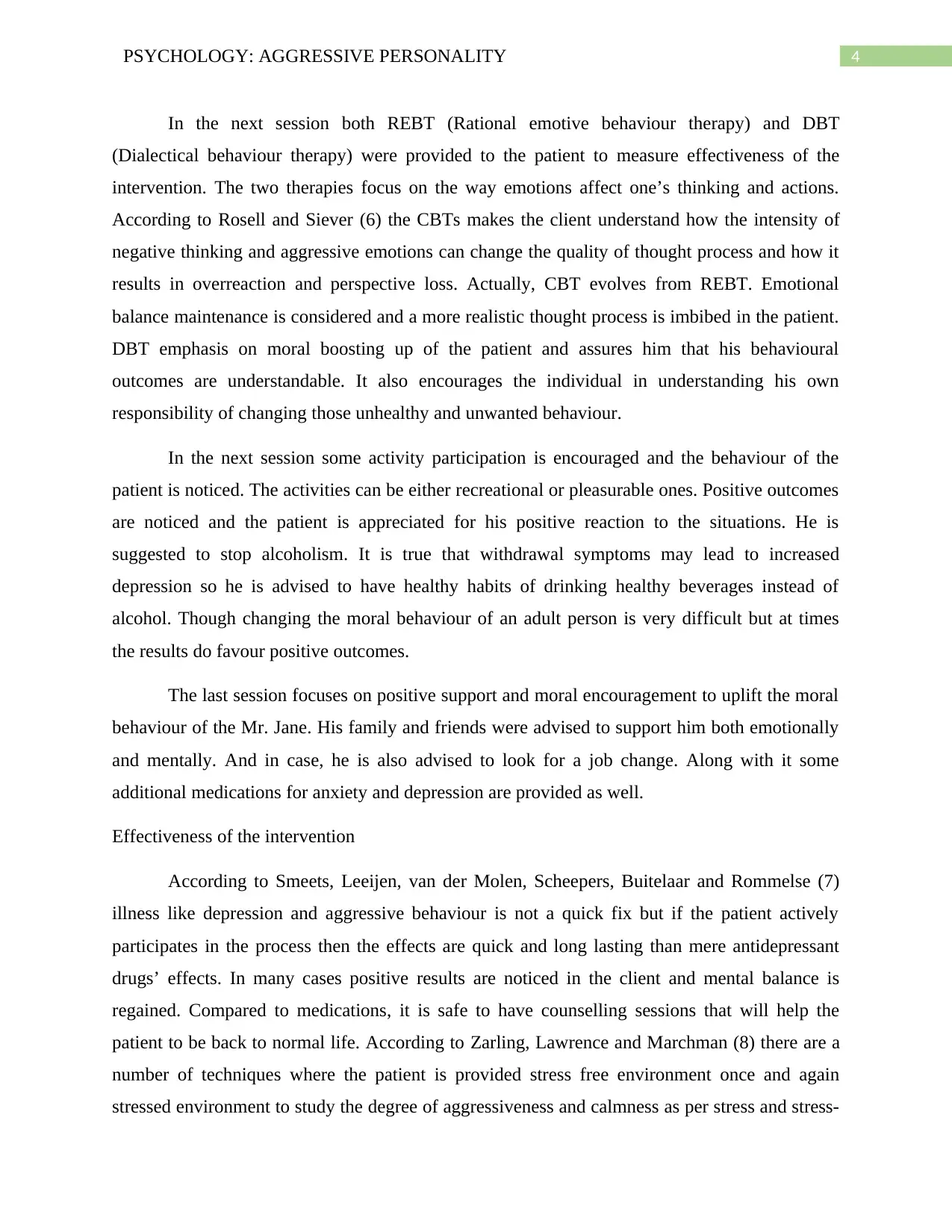
Based on the result interview debriefing is to be suggested. Butchart, Mikton, Dahlberg
and Krug (5) mentioned that the debriefing should include antecedents, behaviour, consequences,
design and re-entry stages. The table below shows the characteristics of each stage.
Interview debriefing stages Characteristics
Antecedents Exploration of what triggered the violence
Behaviour Exploration of the subsequent aggressive behaviour of the
person
Consequences Explanation of the consequences of the participants and others
Design Action plan designing that includes situations that trigger
violence or likely to trigger violence, alternative behaviours and
staff support required for further violence consequences.
Re-entry Assisting the person to re-enter the unit counselling routine
Programme for the duration provided.
incident followed is tracked down by the physiotherapist and it is found that the track follows a
bell-shaped curve where aggression increases from the baseline to peak state and then again
descends to the state of lower aggressive arousal. Kraemer (4) opined that both verbal and non-
verbal mode of communication should be encouraged at every stage of the arousal sequence. The
arousal sequence is shown below.
Stages Phases (prior to
trigger)
Dominant emotion
(baseline emotional
state)
Arousal state
Stage 1 Triggering phase Anxiety Increasing
Stage 2 Transition phase Anger Increasing
Stage 3 Crisis phase Aggression Increasing
Stage 4 Destructive phase Peak arousal state
Stage 5 Descent phase Aggression Decreasing
Stage 6 Transition phase Anger Decreasing
Stage 7 Resolution phase Anger and guilt Decreasing
Based on the result interview debriefing is to be suggested. Butchart, Mikton, Dahlberg
and Krug (5) mentioned that the debriefing should include antecedents, behaviour, consequences,
design and re-entry stages. The table below shows the characteristics of each stage.
Interview debriefing stages Characteristics
Antecedents Exploration of what triggered the violence
Behaviour Exploration of the subsequent aggressive behaviour of the
person
Consequences Explanation of the consequences of the participants and others
Design Action plan designing that includes situations that trigger
violence or likely to trigger violence, alternative behaviours and
staff support required for further violence consequences.
Re-entry Assisting the person to re-enter the unit counselling routine
Programme for the duration provided.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4PSYCHOLOGY: AGGRESSIVE PERSONALITY
In the next session both REBT (Rational emotive behaviour therapy) and DBT
(Dialectical behaviour therapy) were provided to the patient to measure effectiveness of the
intervention. The two therapies focus on the way emotions affect one’s thinking and actions.
According to Rosell and Siever (6) the CBTs makes the client understand how the intensity of
negative thinking and aggressive emotions can change the quality of thought process and how it
results in overreaction and perspective loss. Actually, CBT evolves from REBT. Emotional
balance maintenance is considered and a more realistic thought process is imbibed in the patient.
DBT emphasis on moral boosting up of the patient and assures him that his behavioural
outcomes are understandable. It also encourages the individual in understanding his own
responsibility of changing those unhealthy and unwanted behaviour.
In the next session some activity participation is encouraged and the behaviour of the
patient is noticed. The activities can be either recreational or pleasurable ones. Positive outcomes
are noticed and the patient is appreciated for his positive reaction to the situations. He is
suggested to stop alcoholism. It is true that withdrawal symptoms may lead to increased
depression so he is advised to have healthy habits of drinking healthy beverages instead of
alcohol. Though changing the moral behaviour of an adult person is very difficult but at times
the results do favour positive outcomes.
The last session focuses on positive support and moral encouragement to uplift the moral
behaviour of the Mr. Jane. His family and friends were advised to support him both emotionally
and mentally. And in case, he is also advised to look for a job change. Along with it some
additional medications for anxiety and depression are provided as well.
Effectiveness of the intervention
According to Smeets, Leeijen, van der Molen, Scheepers, Buitelaar and Rommelse (7)
illness like depression and aggressive behaviour is not a quick fix but if the patient actively
participates in the process then the effects are quick and long lasting than mere antidepressant
drugs’ effects. In many cases positive results are noticed in the client and mental balance is
regained. Compared to medications, it is safe to have counselling sessions that will help the
patient to be back to normal life. According to Zarling, Lawrence and Marchman (8) there are a
number of techniques where the patient is provided stress free environment once and again
stressed environment to study the degree of aggressiveness and calmness as per stress and stress-
In the next session both REBT (Rational emotive behaviour therapy) and DBT
(Dialectical behaviour therapy) were provided to the patient to measure effectiveness of the
intervention. The two therapies focus on the way emotions affect one’s thinking and actions.
According to Rosell and Siever (6) the CBTs makes the client understand how the intensity of
negative thinking and aggressive emotions can change the quality of thought process and how it
results in overreaction and perspective loss. Actually, CBT evolves from REBT. Emotional
balance maintenance is considered and a more realistic thought process is imbibed in the patient.
DBT emphasis on moral boosting up of the patient and assures him that his behavioural
outcomes are understandable. It also encourages the individual in understanding his own
responsibility of changing those unhealthy and unwanted behaviour.
In the next session some activity participation is encouraged and the behaviour of the
patient is noticed. The activities can be either recreational or pleasurable ones. Positive outcomes
are noticed and the patient is appreciated for his positive reaction to the situations. He is
suggested to stop alcoholism. It is true that withdrawal symptoms may lead to increased
depression so he is advised to have healthy habits of drinking healthy beverages instead of
alcohol. Though changing the moral behaviour of an adult person is very difficult but at times
the results do favour positive outcomes.
The last session focuses on positive support and moral encouragement to uplift the moral
behaviour of the Mr. Jane. His family and friends were advised to support him both emotionally
and mentally. And in case, he is also advised to look for a job change. Along with it some
additional medications for anxiety and depression are provided as well.
Effectiveness of the intervention
According to Smeets, Leeijen, van der Molen, Scheepers, Buitelaar and Rommelse (7)
illness like depression and aggressive behaviour is not a quick fix but if the patient actively
participates in the process then the effects are quick and long lasting than mere antidepressant
drugs’ effects. In many cases positive results are noticed in the client and mental balance is
regained. Compared to medications, it is safe to have counselling sessions that will help the
patient to be back to normal life. According to Zarling, Lawrence and Marchman (8) there are a
number of techniques where the patient is provided stress free environment once and again
stressed environment to study the degree of aggressiveness and calmness as per stress and stress-
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5PSYCHOLOGY: AGGRESSIVE PERSONALITY
free situations. A lot of unknown areas are discovered during the intervention sessions which
may provide new dimensions for future treatment. Thus, therapeutic interventions like
counselling is very effective for persons having psychological issues like stress, depression and
aggressive personalities.
Limitations
Therapies varies as per requirement and includes psychoanalysis, humanistic therapy and
behavioural therapy. Other forms of psychotherapeutic intervention remained out of discussion
as the psychologists are reluctant to categorise clients differently and assume that preceptor
programs are based on the criminal justice contextual system. This is a major drawback of the
intervention. Also, the research is carried out in a standard group clinical setting so the practical
accuracy is somewhat affected.
free situations. A lot of unknown areas are discovered during the intervention sessions which
may provide new dimensions for future treatment. Thus, therapeutic interventions like
counselling is very effective for persons having psychological issues like stress, depression and
aggressive personalities.
Limitations
Therapies varies as per requirement and includes psychoanalysis, humanistic therapy and
behavioural therapy. Other forms of psychotherapeutic intervention remained out of discussion
as the psychologists are reluctant to categorise clients differently and assume that preceptor
programs are based on the criminal justice contextual system. This is a major drawback of the
intervention. Also, the research is carried out in a standard group clinical setting so the practical
accuracy is somewhat affected.
6PSYCHOLOGY: AGGRESSIVE PERSONALITY
References
1. Franzini A, Broggi G, Cordella R, Dones I, Messina G. Deep-Brain Stimulation for
Aggressive and Disruptive Behavior. World Neurosurgery. 2013;80(3-4):S29.e11-
S29.e14.
2. Frazier S, Vela J. Dialectical behavior therapy for the treatment of anger and aggressive
behavior: A review. Aggression and Violent Behavior. 2014;19(2):156-163.
3. Hillis S, Mercy J, Saul J. The enduring impact of violence against children. Psychology,
Health & Medicine. 2016;22(4):393-405.
4. Kraemer H. Pitfalls of Multisite Randomized Clinical Trials of Efficacy and
Effectiveness. Schizophrenia Bulletin. 2000;26(3):533-541.
5. Butchart A, Mikton C, Dahlberg L, Krug E. Global status report on violence prevention
2014. Injury Prevention. 2015;21(3):213-213.
6. Rosell D, Siever L. The neurobiology of aggression and violence. CNS Spectrums.
2015;20(03):254-279.
7. Smeets K, Leeijen A, van der Molen M, Scheepers F, Buitelaar J, Rommelse N.
Treatment moderators of cognitive behavior therapy to reduce aggressive behavior: a
meta-analysis. European Child & Adolescent Psychiatry. 2014;24(3):255-264.
8. Zarling A, Lawrence E, Marchman J. A randomized controlled trial of acceptance and
commitment therapy for aggressive behavior. Journal of Consulting and Clinical
Psychology. 2015;83(1):199-212.
References
1. Franzini A, Broggi G, Cordella R, Dones I, Messina G. Deep-Brain Stimulation for
Aggressive and Disruptive Behavior. World Neurosurgery. 2013;80(3-4):S29.e11-
S29.e14.
2. Frazier S, Vela J. Dialectical behavior therapy for the treatment of anger and aggressive
behavior: A review. Aggression and Violent Behavior. 2014;19(2):156-163.
3. Hillis S, Mercy J, Saul J. The enduring impact of violence against children. Psychology,
Health & Medicine. 2016;22(4):393-405.
4. Kraemer H. Pitfalls of Multisite Randomized Clinical Trials of Efficacy and
Effectiveness. Schizophrenia Bulletin. 2000;26(3):533-541.
5. Butchart A, Mikton C, Dahlberg L, Krug E. Global status report on violence prevention
2014. Injury Prevention. 2015;21(3):213-213.
6. Rosell D, Siever L. The neurobiology of aggression and violence. CNS Spectrums.
2015;20(03):254-279.
7. Smeets K, Leeijen A, van der Molen M, Scheepers F, Buitelaar J, Rommelse N.
Treatment moderators of cognitive behavior therapy to reduce aggressive behavior: a
meta-analysis. European Child & Adolescent Psychiatry. 2014;24(3):255-264.
8. Zarling A, Lawrence E, Marchman J. A randomized controlled trial of acceptance and
commitment therapy for aggressive behavior. Journal of Consulting and Clinical
Psychology. 2015;83(1):199-212.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 6

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.