Causes of Medication Errors and Practices to Minimize Errors: A Report
VerifiedAdded on 2022/11/16
|27
|7406
|466
Report
AI Summary
This report investigates the main causes of medication errors and explores evidence-based practices to minimize them. It begins with an abstract defining medication errors and their impact, citing prescribing faults, manufacturing errors, and administration issues as key contributors. The report highlights the significant number of medication errors occurring annually and their association with adverse drug reactions, leading to morbidity and mortality. A systematic literature review was conducted, including electronic database searches and quality appraisal of included articles. The findings suggest negligence, excessive workload, and poor staffing ratios as major contributors to medication errors. The report proposes solutions such as encouraging incident reporting, implementing adequate staffing levels, and fostering a blame-free work environment. The report delves into a comprehensive literature review process, detailing the search terms, inclusion/exclusion criteria, and relevance assessment. The analysis of the included articles reveals four notable themes related to medication errors and their prevention. The assignment is a valuable resource for healthcare professionals, students, and researchers interested in improving patient safety and reducing medication-related harm.

Running head: REPORT
What are the main causes of medication errors and what practices can be used to minimize
errors?
Name of the Student
Name of the University
Author Note
What are the main causes of medication errors and what practices can be used to minimize
errors?
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1REPORT
Abstract:
According to Aronson (2009), medication error can be defined as a treatment failure
process that harms the patient and leads to a fatal outcome. Research reports further reveal
that medication errors can take place while planning the medication dose, preparation of the
medication or while administering the medication (Cloete 2015). In this regard it has been
mentioned that medication error is associated with prescribing faults, manufacturing of the
formulation, dispensing the formulation, monitoring and administering the medication
(Berger et al. 2014). Prescribing faults refer to the errors related to irrational, ineffective and
inappropriate prescribing which could potentially be equivalent to under prescribing or
overprescribing (Cesarz et al. 2013). Further, manufacturing error could be a resultant of
incorrect dose preparation of the drug or addition of contaminants. Further, administering
error is associated with incorrect dose and incorrect mode of drug delivery. In addition to
this, failure to alter the devised therapy when required can be counted as monitoring error.
Epidemiological research studies suggest that on an average approximately 237 million
medication errors take place within the healthcare organizations of England annually
(Valentin et al. 2013). The medication errors can potentially trigger adverse drug reactions
which subsequently leads to high rate of morbidity and mortality across UK. Research studies
in this regard state that adverse drug reactions lead to approximately 1700 to 2300 deaths per
year across UK (Valentin et al. 2013).
In light of the research background, the formulated research question for this research
study is: What are the main causes of medication errors and what practices can be used to
minimize errors?
A systematic review of literatures was conducted in order to scan the evidence base
and retrieve relevant solution to the research question. A thorough search was conducted on
the electronic databases of Medline, CINAHL and EBSCOHOST. Research articles were
Abstract:
According to Aronson (2009), medication error can be defined as a treatment failure
process that harms the patient and leads to a fatal outcome. Research reports further reveal
that medication errors can take place while planning the medication dose, preparation of the
medication or while administering the medication (Cloete 2015). In this regard it has been
mentioned that medication error is associated with prescribing faults, manufacturing of the
formulation, dispensing the formulation, monitoring and administering the medication
(Berger et al. 2014). Prescribing faults refer to the errors related to irrational, ineffective and
inappropriate prescribing which could potentially be equivalent to under prescribing or
overprescribing (Cesarz et al. 2013). Further, manufacturing error could be a resultant of
incorrect dose preparation of the drug or addition of contaminants. Further, administering
error is associated with incorrect dose and incorrect mode of drug delivery. In addition to
this, failure to alter the devised therapy when required can be counted as monitoring error.
Epidemiological research studies suggest that on an average approximately 237 million
medication errors take place within the healthcare organizations of England annually
(Valentin et al. 2013). The medication errors can potentially trigger adverse drug reactions
which subsequently leads to high rate of morbidity and mortality across UK. Research studies
in this regard state that adverse drug reactions lead to approximately 1700 to 2300 deaths per
year across UK (Valentin et al. 2013).
In light of the research background, the formulated research question for this research
study is: What are the main causes of medication errors and what practices can be used to
minimize errors?
A systematic review of literatures was conducted in order to scan the evidence base
and retrieve relevant solution to the research question. A thorough search was conducted on
the electronic databases of Medline, CINAHL and EBSCOHOST. Research articles were
2REPORT
search using appropriate key terms and papers that satisfied the inclusion criteria were
considered for the review. The papers integrated within the review were critically appraised
for the quality using the quality analysis matrix.
The overall findings suggest that negligence and excessive work load and poor
staffing ratio contributes to medication error. The potential evidence based solutions
included, encouraging reporting, integrating adequate staffing to balance patient load and
fostering a blame free work environment for care professionals.
search using appropriate key terms and papers that satisfied the inclusion criteria were
considered for the review. The papers integrated within the review were critically appraised
for the quality using the quality analysis matrix.
The overall findings suggest that negligence and excessive work load and poor
staffing ratio contributes to medication error. The potential evidence based solutions
included, encouraging reporting, integrating adequate staffing to balance patient load and
fostering a blame free work environment for care professionals.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3REPORT
Chapter 1
Background
A medication error refers to any wrongful or incorrect administration of a particular
medication, such as, an error in the route or dosage of administration, problem in prescribing
or administering the appropriate medication or formulation, in relation to a specific condition
or disease, problem in observing the accurate time for administration of the medicine,
administration of outdated drugs, or absence of awareness of side effects of particular drug
combinations (Feleke, Mulatu and Yesmaw 2015). According to Blignaut et al. (2017) the
deaths that occur due to medication error can be cited as a condition that occurs when the
treatment providers display lack of proficiency in executing administration of medications
accurately, and also fail to show compliance to the established safety standards for drug
administration. Reports suggest that globally, an estimated 142,000 individuals died in 2013
due to adverse impacts of medical treatment, which was much more than 94,000 deaths that
occurred in 1990 (Abubakar, Tillmann and Banerjee 2015).
According to reports published by the World Health Organization (2016) it has been
assessed that in certain nations roughly 6-7% instances of hospital admissions were
considered to be related to medication, with more than two-thirds of these measured as
avoidable and preventable events, thus possibly occurring due to errors. The condition is
possibly more noticeable amid the elderly, owing to several risk factors, which include
polypharmacy. Results from a study has also revealed that an estimated 237 million incidents
of medication errors have been found to occur in the NHS every year, in England, and these
preventable adverse drug reactions (ADRs) are responsible for an increase in mortality and
morbidity (Elliott et al. 2018). In addition, taking into consideration the total number of
Chapter 1
Background
A medication error refers to any wrongful or incorrect administration of a particular
medication, such as, an error in the route or dosage of administration, problem in prescribing
or administering the appropriate medication or formulation, in relation to a specific condition
or disease, problem in observing the accurate time for administration of the medicine,
administration of outdated drugs, or absence of awareness of side effects of particular drug
combinations (Feleke, Mulatu and Yesmaw 2015). According to Blignaut et al. (2017) the
deaths that occur due to medication error can be cited as a condition that occurs when the
treatment providers display lack of proficiency in executing administration of medications
accurately, and also fail to show compliance to the established safety standards for drug
administration. Reports suggest that globally, an estimated 142,000 individuals died in 2013
due to adverse impacts of medical treatment, which was much more than 94,000 deaths that
occurred in 1990 (Abubakar, Tillmann and Banerjee 2015).
According to reports published by the World Health Organization (2016) it has been
assessed that in certain nations roughly 6-7% instances of hospital admissions were
considered to be related to medication, with more than two-thirds of these measured as
avoidable and preventable events, thus possibly occurring due to errors. The condition is
possibly more noticeable amid the elderly, owing to several risk factors, which include
polypharmacy. Results from a study has also revealed that an estimated 237 million incidents
of medication errors have been found to occur in the NHS every year, in England, and these
preventable adverse drug reactions (ADRs) are responsible for an increase in mortality and
morbidity (Elliott et al. 2018). In addition, taking into consideration the total number of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4REPORT
medication errors that took place, it was found that roughly three in four such cases display
unlikelihood of leading to any potential harm to patients.
Rationale
Owing to the fact that medication administration has been identified as one of the
most significant, multifaceted, yet most vital procedures of nursing care, it requires necessary
amount of expertise and clinical knowledge among the nurses. Medication errors have been
found responsible for the onset of a plethora of undesirable health consequences for all
patients such as, (i) an increase in the length of hospitalization, (ii) increase in costs of
hospitalization, (iii) incapacity and disbelief in the healthcare system, and (iv) damage, injury
or even patient death (Bifftu et al. 2016). Time and again it has been proved that correct
implementation of medication orders that have been prescribed by a general practitioner
forms an essential component of the delivery of health care, and is considered one of the core
competencies of a nurse (Cooper, Tupper and Holm 2016). Initial reports of medication
errors had been reported in 1940, and they gained considerable attention. Research evidences
have also provided evidence for the fact that a significant proportion of healthcare providers
employed in the United States are from foreign republics, and frequently prescribe orders for
different medications that are not even obtainable locally (Gorgich et al. 2016). It has also
been found that an estimated 44 to 98 thousand deaths were attributed to medical errors, of
which 7000 were due to medication errors.
Under circumstances when a drug is questioned by a practitioner, the pharmacist or
nurse is often asked by the physicians for substituting the prescribed medication for an
identical medication. This kind of distortion has also been correlated with major medication
errors owing to the fact that neither the pharmacist nor the non-prescribing practitioner are
able to substitute a medication (Pournamdar and Zare 2016). Some other reasons that have
been associated with medication errors are namely, absence of pharmacological information,
medication errors that took place, it was found that roughly three in four such cases display
unlikelihood of leading to any potential harm to patients.
Rationale
Owing to the fact that medication administration has been identified as one of the
most significant, multifaceted, yet most vital procedures of nursing care, it requires necessary
amount of expertise and clinical knowledge among the nurses. Medication errors have been
found responsible for the onset of a plethora of undesirable health consequences for all
patients such as, (i) an increase in the length of hospitalization, (ii) increase in costs of
hospitalization, (iii) incapacity and disbelief in the healthcare system, and (iv) damage, injury
or even patient death (Bifftu et al. 2016). Time and again it has been proved that correct
implementation of medication orders that have been prescribed by a general practitioner
forms an essential component of the delivery of health care, and is considered one of the core
competencies of a nurse (Cooper, Tupper and Holm 2016). Initial reports of medication
errors had been reported in 1940, and they gained considerable attention. Research evidences
have also provided evidence for the fact that a significant proportion of healthcare providers
employed in the United States are from foreign republics, and frequently prescribe orders for
different medications that are not even obtainable locally (Gorgich et al. 2016). It has also
been found that an estimated 44 to 98 thousand deaths were attributed to medical errors, of
which 7000 were due to medication errors.
Under circumstances when a drug is questioned by a practitioner, the pharmacist or
nurse is often asked by the physicians for substituting the prescribed medication for an
identical medication. This kind of distortion has also been correlated with major medication
errors owing to the fact that neither the pharmacist nor the non-prescribing practitioner are
able to substitute a medication (Pournamdar and Zare 2016). Some other reasons that have
been associated with medication errors are namely, absence of pharmacological information,
5REPORT
incorrect calculation of medication, not showing compliance to the defined protocols,
resemblance in colour and shapes of drugs, resemblance in names of drug, and bad hand
writing of physicians in prescriptions. Medication errors have been identified as a
multidimensional problem, and the prevalence of medication errors can he reduced through
the implementation of appropriate risk management strategies, in the form of a continuous
process for intervention and diagnosis.
Research question
What are the main causes of medication errors and what practices can be used to
minimize errors?
Research aim
To explore the factors that contribute to an increase in the rates of medication errors
all across the globe.
Research objectives
To explore the causes of medication errors
To determine the strategies that can be implemented for reducing medication errors
incorrect calculation of medication, not showing compliance to the defined protocols,
resemblance in colour and shapes of drugs, resemblance in names of drug, and bad hand
writing of physicians in prescriptions. Medication errors have been identified as a
multidimensional problem, and the prevalence of medication errors can he reduced through
the implementation of appropriate risk management strategies, in the form of a continuous
process for intervention and diagnosis.
Research question
What are the main causes of medication errors and what practices can be used to
minimize errors?
Research aim
To explore the factors that contribute to an increase in the rates of medication errors
all across the globe.
Research objectives
To explore the causes of medication errors
To determine the strategies that can be implemented for reducing medication errors
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6REPORT
Chapter 2
Conducting comprehensive literature reviews offer the potential benefit of providing
impartial and unprejudiced summaries of evidence that has previously been printed in
written, focused on a range of research topics. This benefit is mainly appreciated in extensive
research areas, where there numerous publications are existent, each of which place an
emphasis on a particular aspect of the phenomenon that is currently under exploration (Hart
2018). A literature review was carried out with the use of rigorous methodological
techniques, for recognising and collecting scholarly articles that comprise of adequate
information on the underlying factors that are responsible for occurrence of medication errors
and the strategies that can help in preventing them.
In order to conduct an all-inclusive literature review on the phenomenon of
medication error, a three-stage process was framed that comprised of steps namely, (i)
preparation, (ii) conduction, and (iii) making a report. The phase of preparation comprised of
development of a review panel where there were two experts having specialisation in the
domain of medicine and pharmacy. The organized method that was followed at the time of
conducting the literature review was primarily dependent on a 12-step outline that had been
planned by Kable, Pich and Maslin-Prothero (2012). A complete and all-inclusive
documentation of the strategy that had been adopted for searching the articles included in the
literature review facilitated providing a detailed clarification for the rationale and focus of the
review. The aforementioned framework also helped in providing direction all through
development of the strategy, which in turn facilitated ensuring that no indispensable aspects
of the research were eliminated.
Chapter 2
Conducting comprehensive literature reviews offer the potential benefit of providing
impartial and unprejudiced summaries of evidence that has previously been printed in
written, focused on a range of research topics. This benefit is mainly appreciated in extensive
research areas, where there numerous publications are existent, each of which place an
emphasis on a particular aspect of the phenomenon that is currently under exploration (Hart
2018). A literature review was carried out with the use of rigorous methodological
techniques, for recognising and collecting scholarly articles that comprise of adequate
information on the underlying factors that are responsible for occurrence of medication errors
and the strategies that can help in preventing them.
In order to conduct an all-inclusive literature review on the phenomenon of
medication error, a three-stage process was framed that comprised of steps namely, (i)
preparation, (ii) conduction, and (iii) making a report. The phase of preparation comprised of
development of a review panel where there were two experts having specialisation in the
domain of medicine and pharmacy. The organized method that was followed at the time of
conducting the literature review was primarily dependent on a 12-step outline that had been
planned by Kable, Pich and Maslin-Prothero (2012). A complete and all-inclusive
documentation of the strategy that had been adopted for searching the articles included in the
literature review facilitated providing a detailed clarification for the rationale and focus of the
review. The aforementioned framework also helped in providing direction all through
development of the strategy, which in turn facilitated ensuring that no indispensable aspects
of the research were eliminated.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7REPORT
Purpose statement
The objective of the methodology was framed under the leadership and direction of
the project supervisor. The purpose was specified as discovering the problems that make
nursing professionals display an increased likelihood of causing medication error, in addition
to the strategies that can be adopted to prevent them.
Selection criteria
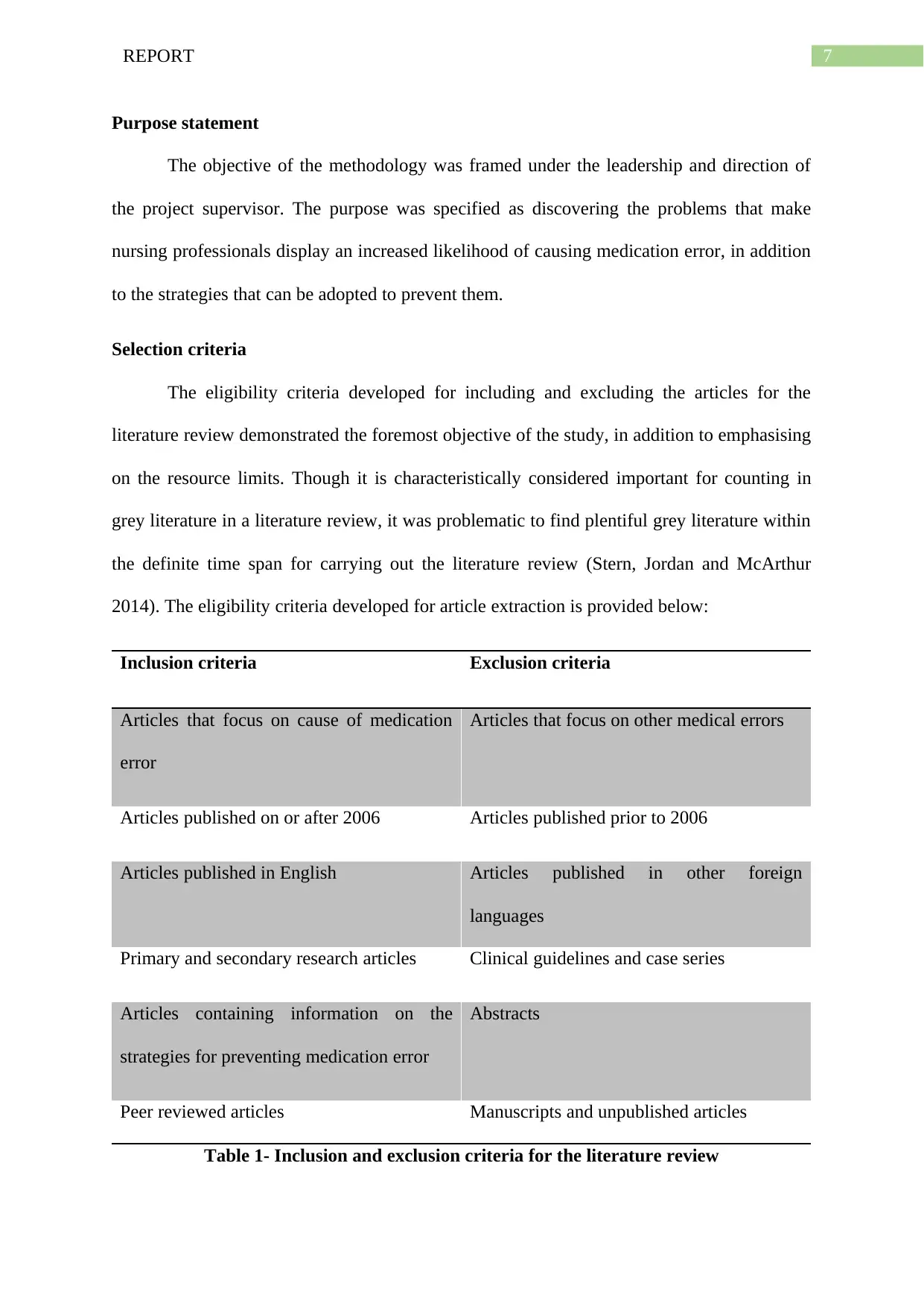
The eligibility criteria developed for including and excluding the articles for the
literature review demonstrated the foremost objective of the study, in addition to emphasising
on the resource limits. Though it is characteristically considered important for counting in
grey literature in a literature review, it was problematic to find plentiful grey literature within
the definite time span for carrying out the literature review (Stern, Jordan and McArthur
2014). The eligibility criteria developed for article extraction is provided below:
Inclusion criteria Exclusion criteria
Articles that focus on cause of medication
error
Articles that focus on other medical errors
Articles published on or after 2006 Articles published prior to 2006
Articles published in English Articles published in other foreign
languages
Primary and secondary research articles Clinical guidelines and case series
Articles containing information on the
strategies for preventing medication error
Abstracts
Peer reviewed articles Manuscripts and unpublished articles
Table 1- Inclusion and exclusion criteria for the literature review
Purpose statement
The objective of the methodology was framed under the leadership and direction of
the project supervisor. The purpose was specified as discovering the problems that make
nursing professionals display an increased likelihood of causing medication error, in addition
to the strategies that can be adopted to prevent them.
Selection criteria
The eligibility criteria developed for including and excluding the articles for the
literature review demonstrated the foremost objective of the study, in addition to emphasising
on the resource limits. Though it is characteristically considered important for counting in
grey literature in a literature review, it was problematic to find plentiful grey literature within
the definite time span for carrying out the literature review (Stern, Jordan and McArthur
2014). The eligibility criteria developed for article extraction is provided below:
Inclusion criteria Exclusion criteria
Articles that focus on cause of medication
error
Articles that focus on other medical errors
Articles published on or after 2006 Articles published prior to 2006
Articles published in English Articles published in other foreign
languages
Primary and secondary research articles Clinical guidelines and case series
Articles containing information on the
strategies for preventing medication error
Abstracts
Peer reviewed articles Manuscripts and unpublished articles
Table 1- Inclusion and exclusion criteria for the literature review
8REPORT
Search terms
The second phase of the literature review encompassed devising search terms, based
on the discussions within the panel. At the time of developing appropriate search terms that
would facilitate taking out articles, pertinent to the research question, the Centre for Reviews
and Dissemination’s (CRD) guideline, framed in 2009 was considered (Zeng et al. 2015).
Based on the guideline, spelling discrepancy, acronyms, and synonyms were also noted.
CINAHL, MEDLINE, and EBSCOHOST electronic databases were comprehensively
searched for recovering the articles, in addition to conducting a manual search of the
bibliography of the extracted scholarly evidences, based on snowballing procedure. The
search terms used were “medication errors”, “drug errors”, “medication administration
errors”, “drug administration errors”, “factors”, “causes”, “influences”, “reasons”,
“determinants”, “strategies”, “methods”, “techniques”, and “interventions”. The
aforementioned search terms were joined with boolean operators ‘AND’, and ‘OR’ in order
to broaden or narrow the search hits (McGowan et al. 2016).
Relevance assessment
After retrieving the evidences from the electronic databases, the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses (PRISMA) helped in determining
significance of the recovered scholarly literature to the research question of interest (Moher
et al. 2015). A three-step procedure was followed for evaluating the articles against a
predetermined criteria. The first stage encompassed assessing the titles of the articles,
following which those that were not relevant to the research were eliminated. Duplicate
articles were also removed at this particular stage. This reduced the initial hits of 111 articles
to 59. The second step comprised of assessing and reading the abstracts of all the articles, in
relation the inclusion and exclusion criteria. This resulted in 22 articles at the end of the
stage. The final stage was conducted in order to assess the full text eligibility of the
Search terms
The second phase of the literature review encompassed devising search terms, based
on the discussions within the panel. At the time of developing appropriate search terms that
would facilitate taking out articles, pertinent to the research question, the Centre for Reviews
and Dissemination’s (CRD) guideline, framed in 2009 was considered (Zeng et al. 2015).
Based on the guideline, spelling discrepancy, acronyms, and synonyms were also noted.
CINAHL, MEDLINE, and EBSCOHOST electronic databases were comprehensively
searched for recovering the articles, in addition to conducting a manual search of the
bibliography of the extracted scholarly evidences, based on snowballing procedure. The
search terms used were “medication errors”, “drug errors”, “medication administration
errors”, “drug administration errors”, “factors”, “causes”, “influences”, “reasons”,
“determinants”, “strategies”, “methods”, “techniques”, and “interventions”. The
aforementioned search terms were joined with boolean operators ‘AND’, and ‘OR’ in order
to broaden or narrow the search hits (McGowan et al. 2016).
Relevance assessment
After retrieving the evidences from the electronic databases, the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses (PRISMA) helped in determining
significance of the recovered scholarly literature to the research question of interest (Moher
et al. 2015). A three-step procedure was followed for evaluating the articles against a
predetermined criteria. The first stage encompassed assessing the titles of the articles,
following which those that were not relevant to the research were eliminated. Duplicate
articles were also removed at this particular stage. This reduced the initial hits of 111 articles
to 59. The second step comprised of assessing and reading the abstracts of all the articles, in
relation the inclusion and exclusion criteria. This resulted in 22 articles at the end of the
stage. The final stage was conducted in order to assess the full text eligibility of the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9REPORT
evidences. Following the exclusion of 14 articles from the 22 evidences, only 8 remained,
which were included in the review.
Quality appraisal
Following determination of the relevance of all evidences incorporated in the review,
all 9 literatures were methodically examined and assessed, for guaranteeing consistency of
the results that they reported. Their findings, validity, and significance to the present
investigation were also assessed.
evidences. Following the exclusion of 14 articles from the 22 evidences, only 8 remained,
which were included in the review.
Quality appraisal
Following determination of the relevance of all evidences incorporated in the review,
all 9 literatures were methodically examined and assessed, for guaranteeing consistency of
the results that they reported. Their findings, validity, and significance to the present
investigation were also assessed.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10REPORT
Chapter 3
A comprehensive and thorough analysis of the 9 articles included in the review lead to
the development of four notable themes namely, (i) incomplete and illegible prescription, (ii)
error provoking work environment, (iii) work load and stress, and (iv) standards for
preventing medication error.
Incomplete and illegible prescription
Fry and Dacey (2007) stated that lack of availability of medications during
administration, often made it necessary for the nurses to go out of their work place and search
the drugs at other locations, thereby acting as a major type of distraction. Furthermore, more
than 50% the respondents suggested that names of drugs (69%) and medication packaging
(57%) or were responsible for medication errors. 59% nursing professionals provided
response that highlighted incomplete prescriptions as the primary reason behind medication
error, while taking care of patients. Impact of incomplete prescriptions were more significant
in infectious disease ward, HDU/CCU ward, and observation ward. The factor that was
identified responsible for hindering effective drug administration was illegible medication
(96%), in addition to medication charts that need to be re-written (53%).
According to Garfield et al. (2016) it was often not possible by healthcare
professionals to provide their patients the necessary access to their medication record, on an
unsupervised basis. In addition, it was also found that absence of any patient friendly
interface often made the medication records incomprehensible, thus leading to medication
errors. Agyemang and While (2010) also stated that presence of illegible handwriting,
inappropriate decimal points, misinterpreted acronyms, misunderstanding and misconstruing
medical prescriptions were considered responsible for majority of medication administration
Chapter 3
A comprehensive and thorough analysis of the 9 articles included in the review lead to
the development of four notable themes namely, (i) incomplete and illegible prescription, (ii)
error provoking work environment, (iii) work load and stress, and (iv) standards for
preventing medication error.
Incomplete and illegible prescription
Fry and Dacey (2007) stated that lack of availability of medications during
administration, often made it necessary for the nurses to go out of their work place and search
the drugs at other locations, thereby acting as a major type of distraction. Furthermore, more
than 50% the respondents suggested that names of drugs (69%) and medication packaging
(57%) or were responsible for medication errors. 59% nursing professionals provided
response that highlighted incomplete prescriptions as the primary reason behind medication
error, while taking care of patients. Impact of incomplete prescriptions were more significant
in infectious disease ward, HDU/CCU ward, and observation ward. The factor that was
identified responsible for hindering effective drug administration was illegible medication
(96%), in addition to medication charts that need to be re-written (53%).
According to Garfield et al. (2016) it was often not possible by healthcare
professionals to provide their patients the necessary access to their medication record, on an
unsupervised basis. In addition, it was also found that absence of any patient friendly
interface often made the medication records incomprehensible, thus leading to medication
errors. Agyemang and While (2010) also stated that presence of illegible handwriting,
inappropriate decimal points, misinterpreted acronyms, misunderstanding and misconstruing
medical prescriptions were considered responsible for majority of medication administration
11REPORT
errors. It was also found that designing of technology comprised of several factors like
labelling and packaging of medication products and significantly contributed to errors.
Error provoking work environment
An analysis of the findings presented by Fry and Dacey (2007) also suggested that
those nursing professionals who were accountable for delivering care to elderly patients
admitted to HDU/CCU wards encountered frequent interruptions from their colleagues that
often made them make mistakes during drug administration. This was also attributed to the
fact that the elderly patients are generally more dependent, in relation to their caregiving
procedure. The same was confirmed by Agyemang and While (2010) interruptions and
distractions were the significant organisational factors that lead to interruption of the nurses,
thus making them feel distracted. This generally made the nurses perform errors in the dosage
and route of drug administration. This was affirmed by the findings presented by Keers et al.
(2018) who elaborated on the fact that nursing knowledge and guideline based mistakes made
by healthcare professionals generally involved flawed planning and under several
circumstances made them incapable of understanding what medicine has been recommended,
by looking at the prescription. The researchers also confirmed the previous findings and
stated that nurses were frequently subjected to problems in written communication associated
with prescriptions. Prescriptions given by practitioners were often ambiguous owing to the
fact that they contained portions that were unclearly written or crossed out, besides presence
of previous drug administration that had not been omitted. They also found that family
members of patients talking outside the clinics and busy shifts in the healthcare wards were
directly responsible for interrupting the nurses in the process of medication administration,
thus acting as barriers.
Garfield et al. (2016) also highlighted that several healthcare settings reported
presence of an institutional culture that expected the patients to adorn their role as a sick
errors. It was also found that designing of technology comprised of several factors like
labelling and packaging of medication products and significantly contributed to errors.
Error provoking work environment
An analysis of the findings presented by Fry and Dacey (2007) also suggested that
those nursing professionals who were accountable for delivering care to elderly patients
admitted to HDU/CCU wards encountered frequent interruptions from their colleagues that
often made them make mistakes during drug administration. This was also attributed to the
fact that the elderly patients are generally more dependent, in relation to their caregiving
procedure. The same was confirmed by Agyemang and While (2010) interruptions and
distractions were the significant organisational factors that lead to interruption of the nurses,
thus making them feel distracted. This generally made the nurses perform errors in the dosage
and route of drug administration. This was affirmed by the findings presented by Keers et al.
(2018) who elaborated on the fact that nursing knowledge and guideline based mistakes made
by healthcare professionals generally involved flawed planning and under several
circumstances made them incapable of understanding what medicine has been recommended,
by looking at the prescription. The researchers also confirmed the previous findings and
stated that nurses were frequently subjected to problems in written communication associated
with prescriptions. Prescriptions given by practitioners were often ambiguous owing to the
fact that they contained portions that were unclearly written or crossed out, besides presence
of previous drug administration that had not been omitted. They also found that family
members of patients talking outside the clinics and busy shifts in the healthcare wards were
directly responsible for interrupting the nurses in the process of medication administration,
thus acting as barriers.
Garfield et al. (2016) also highlighted that several healthcare settings reported
presence of an institutional culture that expected the patients to adorn their role as a sick
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 27
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.