Investigating Mental Health Literacy Affecting Healthcare Access
VerifiedAdded on 2023/03/31
|11
|2083
|409
Report
AI Summary
This research proposal investigates the impact of mental health literacy on access to mental healthcare in Australia. It addresses research questions concerning how health literacy affects healthcare access, the influence of social and cultural inequalities, and strategies for improving public health awareness. The study employs a qualitative research design involving semi-structured interviews with participants aged 20-70, followed by thematic analysis of the collected data. Ethical considerations, including informed consent and participant confidentiality, are prioritized. The expected outcome is to identify significant psychological factors that hinder health awareness and mental health literacy, contributing to a better understanding of barriers to healthcare access. Desklib provides students with access to a wide range of past papers and solved assignments.

RUNNING HEAD: RESEARCH PROPOSAL
RESEARCH PROPOSAL
Name of Student
Name of University
Author note
RESEARCH PROPOSAL
Name of Student
Name of University
Author note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1RESEARCH PROPOSAL
Table of Contents
1) INTRODUCTION..............................................................................................................2
1.1 INTRODUCTION.......................................................................................................2
1.2 BACKGROUND.........................................................................................................3
1.3 RESEARCH AIM.......................................................................................................4
1.4 RESEARCH QUESTIONS..............................................................................................4
2) LITERATURE REVIEW...................................................................................................4
3) LITERATURE GAP...........................................................................................................6
4) RESEARCH DESIGN........................................................................................................6
4.1 DATA COLLECTION................................................................................................6
4.2 DATA ANALYSIS.....................................................................................................7
5. ETHICAL CONSIDERATIONS...........................................................................................7
6. GANTT CHART: required time frame for this research.......................................................7
7. EXPECTED OUTCOME.......................................................................................................8
Table of Contents
1) INTRODUCTION..............................................................................................................2
1.1 INTRODUCTION.......................................................................................................2
1.2 BACKGROUND.........................................................................................................3
1.3 RESEARCH AIM.......................................................................................................4
1.4 RESEARCH QUESTIONS..............................................................................................4
2) LITERATURE REVIEW...................................................................................................4
3) LITERATURE GAP...........................................................................................................6
4) RESEARCH DESIGN........................................................................................................6
4.1 DATA COLLECTION................................................................................................6
4.2 DATA ANALYSIS.....................................................................................................7
5. ETHICAL CONSIDERATIONS...........................................................................................7
6. GANTT CHART: required time frame for this research.......................................................7
7. EXPECTED OUTCOME.......................................................................................................8
2RESEARCH PROPOSAL
1) INTRODUCTION
1.1 INTRODUCTION
The healthcare performance in Australia is underpinned by health literacy and extent
of health access, which determines to what extent an individual can assess a particular form
of health care according to his specified needs. There are various conceptions surrounding the
healthcare access in literatures of health policies [1]. Measuring the level of this access is a
very difficult task because it involves different dimensions of analysis like that of physical
and financial accessibility [2], the demand of that health treatment, the enablers [3] and the
barriers [4], the quality indicators and the availability. General practice in Australia [5] is
often described and projected as the cornerstone in primary Australian health care. It has been
reported to perform specific cardinal roles in healthcare system, including the first point of
medical contact, maintenance of an ongoing health intervention and coordinating the clinical
care between various primary and tertiary level health providers. Very importantly a clinical
practice does a security’s role for the tertiary healthcare structures for a general practitioner
send the patients to tertiary care. But as a matter of fact, this process is quite slow and time
taking as the disease- unaware Australian patients has to pass through this GP buffer to reach
the tertiary where his actual treatment will be done and by then, the severity of the pathology
has already increased.
Australian patients with anxiety disorders [6], dysthymia [7], neurotic syndromes is
has least knowledge about the disease, condition or the nature of mental parameter affected in
a certain physiological or psychological pathology. All these subjects with even severe cases
of depression, schizophrenia and bipolar disorders take up a very chaotic and complex route
to reach and receive the expert level treatments for their condition. This results from below
average or below basic level of health literacy and mental health literacy amongst general
population and their limited access to proper healthcare.
1) INTRODUCTION
1.1 INTRODUCTION
The healthcare performance in Australia is underpinned by health literacy and extent
of health access, which determines to what extent an individual can assess a particular form
of health care according to his specified needs. There are various conceptions surrounding the
healthcare access in literatures of health policies [1]. Measuring the level of this access is a
very difficult task because it involves different dimensions of analysis like that of physical
and financial accessibility [2], the demand of that health treatment, the enablers [3] and the
barriers [4], the quality indicators and the availability. General practice in Australia [5] is
often described and projected as the cornerstone in primary Australian health care. It has been
reported to perform specific cardinal roles in healthcare system, including the first point of
medical contact, maintenance of an ongoing health intervention and coordinating the clinical
care between various primary and tertiary level health providers. Very importantly a clinical
practice does a security’s role for the tertiary healthcare structures for a general practitioner
send the patients to tertiary care. But as a matter of fact, this process is quite slow and time
taking as the disease- unaware Australian patients has to pass through this GP buffer to reach
the tertiary where his actual treatment will be done and by then, the severity of the pathology
has already increased.
Australian patients with anxiety disorders [6], dysthymia [7], neurotic syndromes is
has least knowledge about the disease, condition or the nature of mental parameter affected in
a certain physiological or psychological pathology. All these subjects with even severe cases
of depression, schizophrenia and bipolar disorders take up a very chaotic and complex route
to reach and receive the expert level treatments for their condition. This results from below
average or below basic level of health literacy and mental health literacy amongst general
population and their limited access to proper healthcare.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3RESEARCH PROPOSAL
1.2 BACKGROUND
Mental health severity is a direct outcome of mental health literacy [8]. Globally, it
has been proved and shown by many researchers on science and healthcare that unaware and
health illiterate subjects are more prone to develop severe, irreversible cases of health and
mental condition. Health literacy can be defined as one’s awareness about the healthcare’s
clinical environment and HL focusses on people’s ability to comprehend their own condition,
the resources and make right use of the medically relevant information, particularly to
develop self-care and adherence to his medications.
Health Literacy requires an understanding of a broader construct which is considered
as basic and fundamental in improvement of an individual’s health outcome, decreasing the
healthcare access inequities amongst the populations and finally enhancing operational
processes of healthcare framework. The first step in health literacy is self-motivated person
willing to know about his own health and physical condition and correlate that to his right to
health and access to the most apt form of healthcare in spite of all social and cultural
inequalities.
People’s access to general practitioners for their mental health conditions at specific
points, repetitively and time and time again is clear indicator of a person’s illiteracy about a
disease and his or her bestowing of a blind faith on a medical practitioner who is not being
able to treat him in spite of repeated visits. This increases the anxiety and depression levels in
a patient which worsens his mental or physical condition. Hence lack of clinical skills in
treating a mental health patients, reduced accessibility to secondary and tertiary care
hospitals, lack of relevant knowledge about a mental health and decreased or complete
absence of self-care attitudes and depending blinding on a medical practitioner to get cured
1.2 BACKGROUND
Mental health severity is a direct outcome of mental health literacy [8]. Globally, it
has been proved and shown by many researchers on science and healthcare that unaware and
health illiterate subjects are more prone to develop severe, irreversible cases of health and
mental condition. Health literacy can be defined as one’s awareness about the healthcare’s
clinical environment and HL focusses on people’s ability to comprehend their own condition,
the resources and make right use of the medically relevant information, particularly to
develop self-care and adherence to his medications.
Health Literacy requires an understanding of a broader construct which is considered
as basic and fundamental in improvement of an individual’s health outcome, decreasing the
healthcare access inequities amongst the populations and finally enhancing operational
processes of healthcare framework. The first step in health literacy is self-motivated person
willing to know about his own health and physical condition and correlate that to his right to
health and access to the most apt form of healthcare in spite of all social and cultural
inequalities.
People’s access to general practitioners for their mental health conditions at specific
points, repetitively and time and time again is clear indicator of a person’s illiteracy about a
disease and his or her bestowing of a blind faith on a medical practitioner who is not being
able to treat him in spite of repeated visits. This increases the anxiety and depression levels in
a patient which worsens his mental or physical condition. Hence lack of clinical skills in
treating a mental health patients, reduced accessibility to secondary and tertiary care
hospitals, lack of relevant knowledge about a mental health and decreased or complete
absence of self-care attitudes and depending blinding on a medical practitioner to get cured
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4RESEARCH PROPOSAL
without any therapeutic application or precautionary measure from one’s own side are been
the major barriers to the sustenance of a best practice based healthcare delivery.
1.3 RESEARCH AIM
The aim of this proposed research is to understand the mental health care literacy
affecting the access to mental healthcare in Australia.
1.4 RESEARCH QUESTIONS
The proposed study will address the following research questions:-
1. How do health literacy affect healthcare access?
2. How do social and cultural inequality affect obtaining of mental health care?
3. What are the different strategies to improve public health awareness and health
literacy?
2) LITERATURE REVIEW
According to Kutcher, Wei and Coniglio 2016 [9] -The concept of mental health
literacy arises from health literacy and is continually evolving. According to the study –
Mental health study can be explained as beliefs and knowledge about the mental disorders
which hampers the life processes and even recognition and self-management. The study does
a literature review to understand that to identify the deficient areas of health and mental
health literacy amongst the Australian population and how they can be ‘changed’ with
effective methods to help an individual prevent his own mental disorder or get a quality
health service at one go without running through the hierarchy of different medical
disciplines. The study implies that the impairment recognition can impact patient knowledge
and assist him to receive effective forms of self-help strategies to intervene the ‘problems’
correctly. This research study puts a special emphasis on cognition and behavioral
development of an individual so that he can care for himself.
without any therapeutic application or precautionary measure from one’s own side are been
the major barriers to the sustenance of a best practice based healthcare delivery.
1.3 RESEARCH AIM
The aim of this proposed research is to understand the mental health care literacy
affecting the access to mental healthcare in Australia.
1.4 RESEARCH QUESTIONS
The proposed study will address the following research questions:-
1. How do health literacy affect healthcare access?
2. How do social and cultural inequality affect obtaining of mental health care?
3. What are the different strategies to improve public health awareness and health
literacy?
2) LITERATURE REVIEW
According to Kutcher, Wei and Coniglio 2016 [9] -The concept of mental health
literacy arises from health literacy and is continually evolving. According to the study –
Mental health study can be explained as beliefs and knowledge about the mental disorders
which hampers the life processes and even recognition and self-management. The study does
a literature review to understand that to identify the deficient areas of health and mental
health literacy amongst the Australian population and how they can be ‘changed’ with
effective methods to help an individual prevent his own mental disorder or get a quality
health service at one go without running through the hierarchy of different medical
disciplines. The study implies that the impairment recognition can impact patient knowledge
and assist him to receive effective forms of self-help strategies to intervene the ‘problems’
correctly. This research study puts a special emphasis on cognition and behavioral
development of an individual so that he can care for himself.
5RESEARCH PROPOSAL
Pearson and Saunders 2009 [10], aimed to understand different measurements of the
health literacy in both Australian and international literature and also discuss about the
distinction between broader conceptualizations of ‘health and mental health literacy’ in a
daily life manner and how does it differs from ‘medical literacy’. The study sees health
literacy as a plane in which medical information can be accessed at ease, comprehended and
can be used to better self-care techniques. However, the study focus on the literacy problem
by doing a literature review and it identifies that - despite World Health Organization's
initiatives to empower patients and layman with medical knowledge – the term ‘health
literary’ persists to be a very confusing thing. The study highlights health literacy importance
with respect to health promotion and preventive measures. The study analyses the collected
data and runs a coding to segregate the different ideas and finally, they conclude that health
literacy needs motivation, knowledge and activation to affect an attitude change in public
health awareness. Health policies, treatment patterns and an internal quest to understand and
take care of one’s own well-being are the major action areas. The health literacy concepts
needs to find a consensus amongst Australian population and global population as a whole
and this research article implies the use of ‘educational strategies’ to address the same.
Ashfield et al., 2017 aimed to focus on a very different problem all together that has
passed unnoticed from the eyes of many and that is the ‘media’ problem associated with
health literacy[11]. Although, because of media – the common mass has come to know about
the treatments, protocols and treatment guideline much more which has certainly contributed
to awareness but it also creates a perception that one can receive different types of treatments
for a single disease and this often astray a person from the central intervention that has to be
used for a specific condition. The media disarrays a subject from the specific effective care he
might want to receive for his condition as he has been provided with a number of options.
Most consultations focusing on people’s ‘mental health’ occur first in general medical
Pearson and Saunders 2009 [10], aimed to understand different measurements of the
health literacy in both Australian and international literature and also discuss about the
distinction between broader conceptualizations of ‘health and mental health literacy’ in a
daily life manner and how does it differs from ‘medical literacy’. The study sees health
literacy as a plane in which medical information can be accessed at ease, comprehended and
can be used to better self-care techniques. However, the study focus on the literacy problem
by doing a literature review and it identifies that - despite World Health Organization's
initiatives to empower patients and layman with medical knowledge – the term ‘health
literary’ persists to be a very confusing thing. The study highlights health literacy importance
with respect to health promotion and preventive measures. The study analyses the collected
data and runs a coding to segregate the different ideas and finally, they conclude that health
literacy needs motivation, knowledge and activation to affect an attitude change in public
health awareness. Health policies, treatment patterns and an internal quest to understand and
take care of one’s own well-being are the major action areas. The health literacy concepts
needs to find a consensus amongst Australian population and global population as a whole
and this research article implies the use of ‘educational strategies’ to address the same.
Ashfield et al., 2017 aimed to focus on a very different problem all together that has
passed unnoticed from the eyes of many and that is the ‘media’ problem associated with
health literacy[11]. Although, because of media – the common mass has come to know about
the treatments, protocols and treatment guideline much more which has certainly contributed
to awareness but it also creates a perception that one can receive different types of treatments
for a single disease and this often astray a person from the central intervention that has to be
used for a specific condition. The media disarrays a subject from the specific effective care he
might want to receive for his condition as he has been provided with a number of options.
Most consultations focusing on people’s ‘mental health’ occur first in general medical
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6RESEARCH PROPOSAL
practice. The study takes a situational approach to understand mental health literacy and
categorizes the collective data on different psychopathological sections and tries to analyze a
particular population with respect to a particular mental health. Then, the researchers
correlate the analyzed information with their awareness level (stimulated by media). The
study concludes by providing implication on psychological support, suicide prevention
campaigns, enhanced- quality of life as important mental health literacy improvement
strategy. This approaches, according to the study –can remove service demand and cost
problem related burdens the healthcare infrastructures and enhance mental health literary.
3) LITERATURE GAP
There has been many researches on the perception of public about severe mental
illnesses like multiple personality disorder [12], schizophrenia and how social, economic,
cultural factors have impacted their health literacy. But no researches have studied internal
factors like individual behaviors and group behaviors that has been a barrier to medical
learning and healthcare awareness. This proposed study will fill the research gap by studying
the intrinsic human factors related to deficient health and mental health care literacy.
4) RESEARCH DESIGN
4.1 DATA COLLECTION
A semi structured interview will be done with the selected candidates. The
candidates to be interviewed will include participants of both genders, of age group from
20 to 70 years. Open ended questions will be used and the interviews with audio recorded
for analysis.
practice. The study takes a situational approach to understand mental health literacy and
categorizes the collective data on different psychopathological sections and tries to analyze a
particular population with respect to a particular mental health. Then, the researchers
correlate the analyzed information with their awareness level (stimulated by media). The
study concludes by providing implication on psychological support, suicide prevention
campaigns, enhanced- quality of life as important mental health literacy improvement
strategy. This approaches, according to the study –can remove service demand and cost
problem related burdens the healthcare infrastructures and enhance mental health literary.
3) LITERATURE GAP
There has been many researches on the perception of public about severe mental
illnesses like multiple personality disorder [12], schizophrenia and how social, economic,
cultural factors have impacted their health literacy. But no researches have studied internal
factors like individual behaviors and group behaviors that has been a barrier to medical
learning and healthcare awareness. This proposed study will fill the research gap by studying
the intrinsic human factors related to deficient health and mental health care literacy.
4) RESEARCH DESIGN
4.1 DATA COLLECTION
A semi structured interview will be done with the selected candidates. The
candidates to be interviewed will include participants of both genders, of age group from
20 to 70 years. Open ended questions will be used and the interviews with audio recorded
for analysis.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7RESEARCH PROPOSAL
4.2 DATA ANALYSIS
Codes will be applied to interviews and then analyzed till a consensus is reached on
coding tree. Then, a thematic analysis will be done to determine the relevant themes.
5. ETHICAL CONSIDERATIONS
A written consent will be taken from all the participant to assure their voluntary
participation. The participant will have the full right to withdraw from the study as per their
wish. The research resources will be distributed equally to all participants and there will no
bias from the perspectives of researchers.
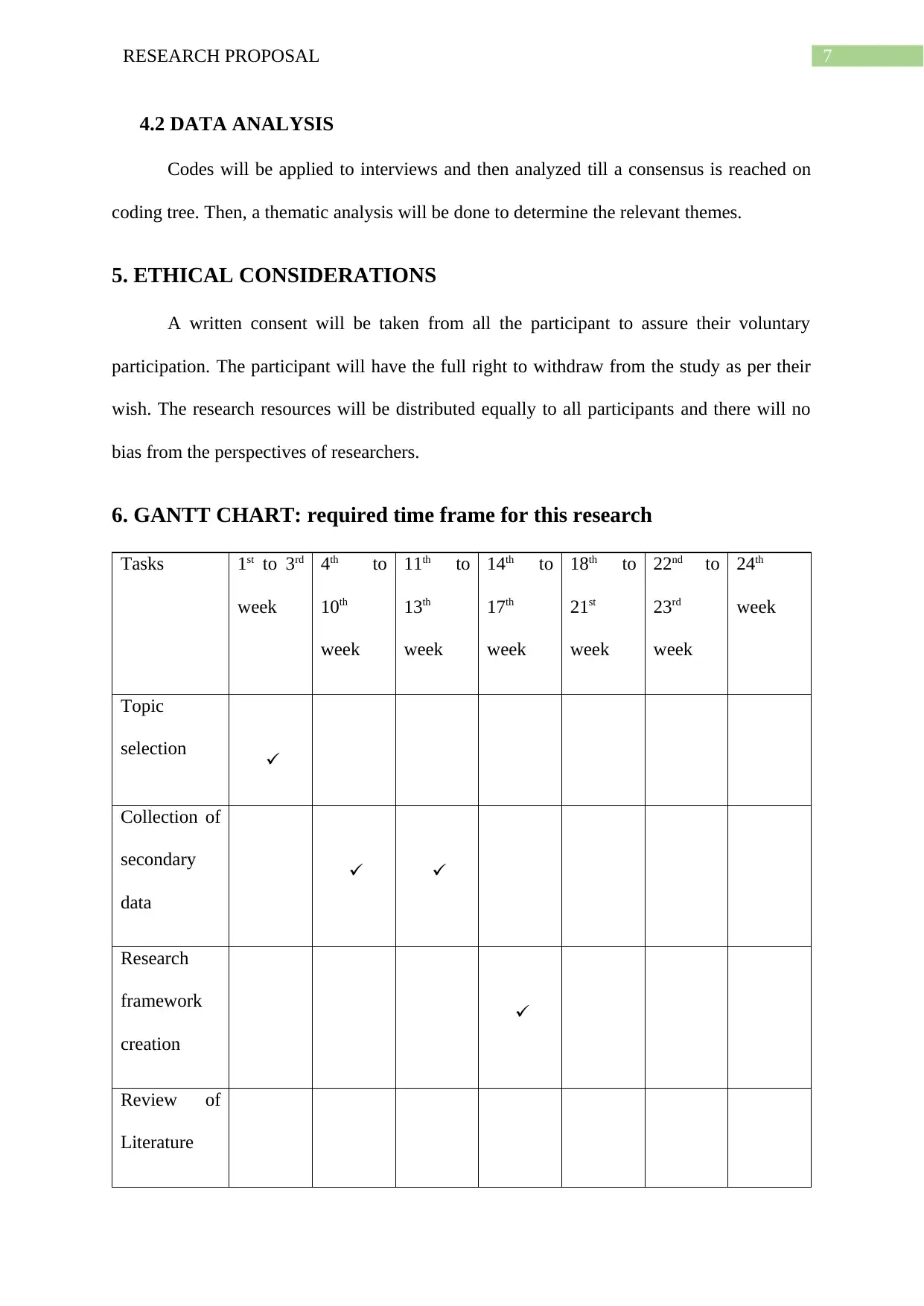
6. GANTT CHART: required time frame for this research
Tasks 1st to 3rd
week
4th to
10th
week
11th to
13th
week
14th to
17th
week
18th to
21st
week
22nd to
23rd
week
24th
week
Topic
selection
Collection of
secondary
data
Research
framework
creation
Review of
Literature
4.2 DATA ANALYSIS
Codes will be applied to interviews and then analyzed till a consensus is reached on
coding tree. Then, a thematic analysis will be done to determine the relevant themes.
5. ETHICAL CONSIDERATIONS
A written consent will be taken from all the participant to assure their voluntary
participation. The participant will have the full right to withdraw from the study as per their
wish. The research resources will be distributed equally to all participants and there will no
bias from the perspectives of researchers.
6. GANTT CHART: required time frame for this research
Tasks 1st to 3rd
week
4th to
10th
week
11th to
13th
week
14th to
17th
week
18th to
21st
week
22nd to
23rd
week
24th
week
Topic
selection
Collection of
secondary
data
Research
framework
creation
Review of
Literature
8RESEARCH PROPOSAL
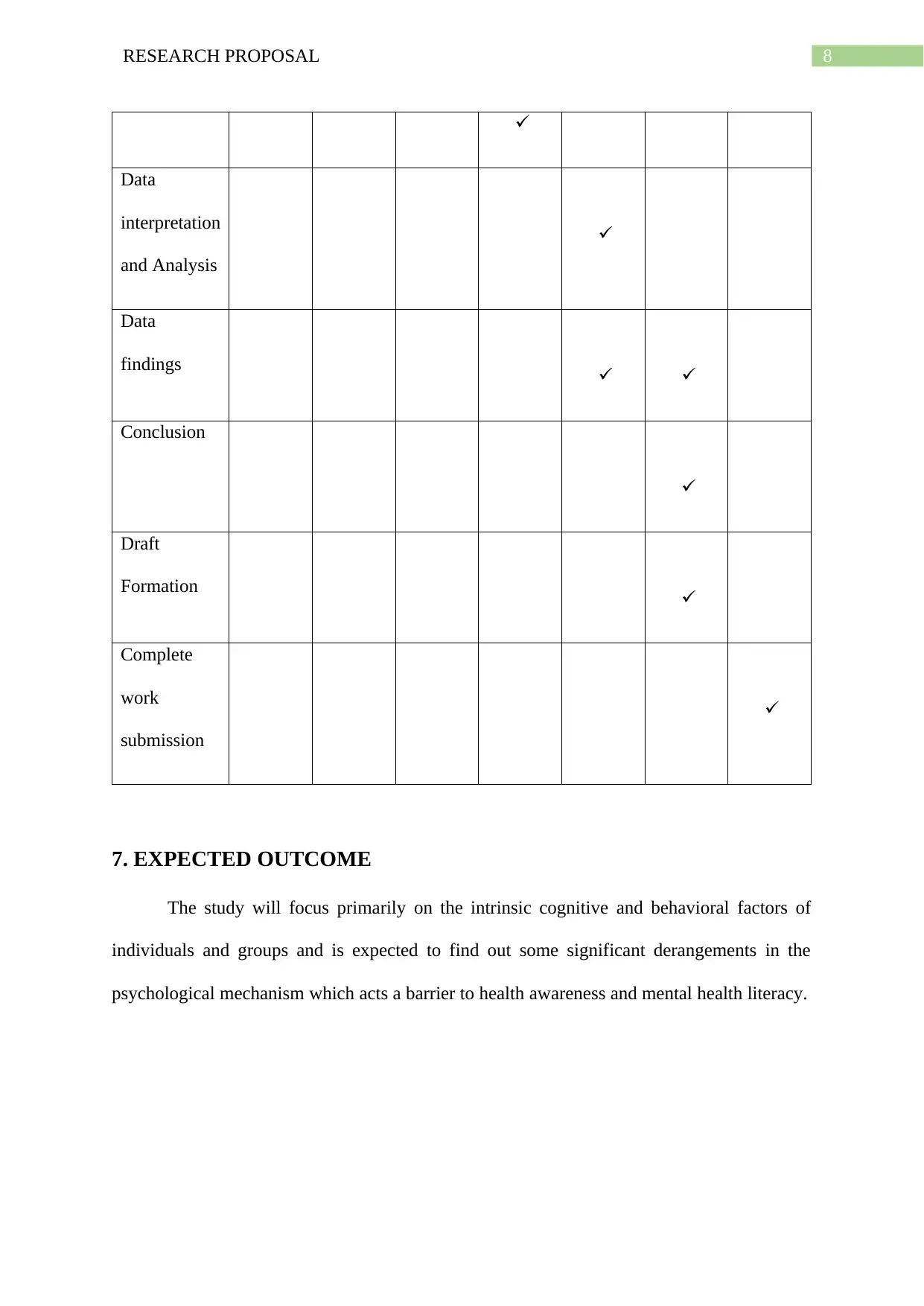
Data
interpretation
and Analysis
Data
findings
Conclusion
Draft
Formation
Complete
work
submission
7. EXPECTED OUTCOME
The study will focus primarily on the intrinsic cognitive and behavioral factors of
individuals and groups and is expected to find out some significant derangements in the
psychological mechanism which acts a barrier to health awareness and mental health literacy.
Data
interpretation
and Analysis
Data
findings
Conclusion
Draft
Formation
Complete
work
submission
7. EXPECTED OUTCOME
The study will focus primarily on the intrinsic cognitive and behavioral factors of
individuals and groups and is expected to find out some significant derangements in the
psychological mechanism which acts a barrier to health awareness and mental health literacy.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9RESEARCH PROPOSAL
References
1. Sinclair S, Norris JM, McConnell SJ, Chochinov HM, Hack TF, Hagen NA,
McClement S, Bouchal SR. Compassion: a scoping review of the healthcare literature.
BMC palliative care. 2016 Dec;15(1):6.
2. Whitty JA, Littlejohns P. Social values and health priority setting in Australia: an
analysis applied to the context of health technology assessment. Health Policy. 2015
Feb 1;119(2):127-36.
3. Olds J, Reilly R, Yerrell P, Stajic J, Micklem J, Morey K, Brown A. Exploring
barriers to and enablers of adequate healthcare for Indigenous Australian prisoners
with cancer: a scoping review drawing on evidence from Australia, Canada and the
United States. Health & justice. 2016 Dec;4(1):5.
4. Bastos JL, Harnois CE, Paradies YC. Health care barriers, racism, and
intersectionality in Australia. Social Science & Medicine. 2018 Feb 1;199:209-18.
5. Idel I, Choy SW, Marnoch C, McMahon LP. A review of the structure and training
pathways for obstetric medicine physicians in Australia and New Zealand. Obstetric
medicine. 2017 Dec;10(4):161-4.
6. Perales F, Johnson SE, Baxter J, Lawrence D, Zubrick SR. Family structure and
childhood mental disorders: new findings from Australia. Social psychiatry and
psychiatric epidemiology. 2017 Apr 1;52(4):423-33.
7. Wilson T, Allen KA. Mixed psychological interventions for Persistent Depressive
Disorder (Dysthymia). InThe Elements of Psychological Case Report Writing in
Australia 2018 (pp. 235-243). Routledge.
References
1. Sinclair S, Norris JM, McConnell SJ, Chochinov HM, Hack TF, Hagen NA,
McClement S, Bouchal SR. Compassion: a scoping review of the healthcare literature.
BMC palliative care. 2016 Dec;15(1):6.
2. Whitty JA, Littlejohns P. Social values and health priority setting in Australia: an
analysis applied to the context of health technology assessment. Health Policy. 2015
Feb 1;119(2):127-36.
3. Olds J, Reilly R, Yerrell P, Stajic J, Micklem J, Morey K, Brown A. Exploring
barriers to and enablers of adequate healthcare for Indigenous Australian prisoners
with cancer: a scoping review drawing on evidence from Australia, Canada and the
United States. Health & justice. 2016 Dec;4(1):5.
4. Bastos JL, Harnois CE, Paradies YC. Health care barriers, racism, and
intersectionality in Australia. Social Science & Medicine. 2018 Feb 1;199:209-18.
5. Idel I, Choy SW, Marnoch C, McMahon LP. A review of the structure and training
pathways for obstetric medicine physicians in Australia and New Zealand. Obstetric
medicine. 2017 Dec;10(4):161-4.
6. Perales F, Johnson SE, Baxter J, Lawrence D, Zubrick SR. Family structure and
childhood mental disorders: new findings from Australia. Social psychiatry and
psychiatric epidemiology. 2017 Apr 1;52(4):423-33.
7. Wilson T, Allen KA. Mixed psychological interventions for Persistent Depressive
Disorder (Dysthymia). InThe Elements of Psychological Case Report Writing in
Australia 2018 (pp. 235-243). Routledge.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10RESEARCH PROPOSAL
8. Guajardo MG, Slewa-Younan S, Kitchener BA, Mannan H, Mohammad Y, Jorm AF.
Improving the capacity of community-based workers in Australia to provide initial
assistance to Iraqi refugees with mental health problems: an uncontrolled evaluation
of a Mental Health Literacy Course. International journal of mental health systems.
2018 Dec;12(1):2.
9. Kutcher S, Wei Y, Coniglio C. Mental health literacy: past, present, and future. The
Canadian Journal of Psychiatry. 2016 Mar;61(3):154-8.
10. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it
matter?. Health promotion international. 2009 Apr 16;24(3):285-96.
11. Ashfield J, Macdonald J, Francis A, Smith A. A ‘situational approach’to mental
health literacy in Australia. malesuicidepreventionaustralia. com.
au/resources/resource. 2017:1-30.
12. Ringrose, J. L. (2018). Understanding and Treating Dissociative Identity Disorder
(or Multiple Personality Disorder). Routledge.
8. Guajardo MG, Slewa-Younan S, Kitchener BA, Mannan H, Mohammad Y, Jorm AF.
Improving the capacity of community-based workers in Australia to provide initial
assistance to Iraqi refugees with mental health problems: an uncontrolled evaluation
of a Mental Health Literacy Course. International journal of mental health systems.
2018 Dec;12(1):2.
9. Kutcher S, Wei Y, Coniglio C. Mental health literacy: past, present, and future. The
Canadian Journal of Psychiatry. 2016 Mar;61(3):154-8.
10. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it
matter?. Health promotion international. 2009 Apr 16;24(3):285-96.
11. Ashfield J, Macdonald J, Francis A, Smith A. A ‘situational approach’to mental
health literacy in Australia. malesuicidepreventionaustralia. com.
au/resources/resource. 2017:1-30.
12. Ringrose, J. L. (2018). Understanding and Treating Dissociative Identity Disorder
(or Multiple Personality Disorder). Routledge.
1 out of 11
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.