HLTH 1037: Mental Health Supplementary Assessment - ISBAR Handover
VerifiedAdded on 2022/08/20
|6
|2079
|10
Practical Assignment
AI Summary
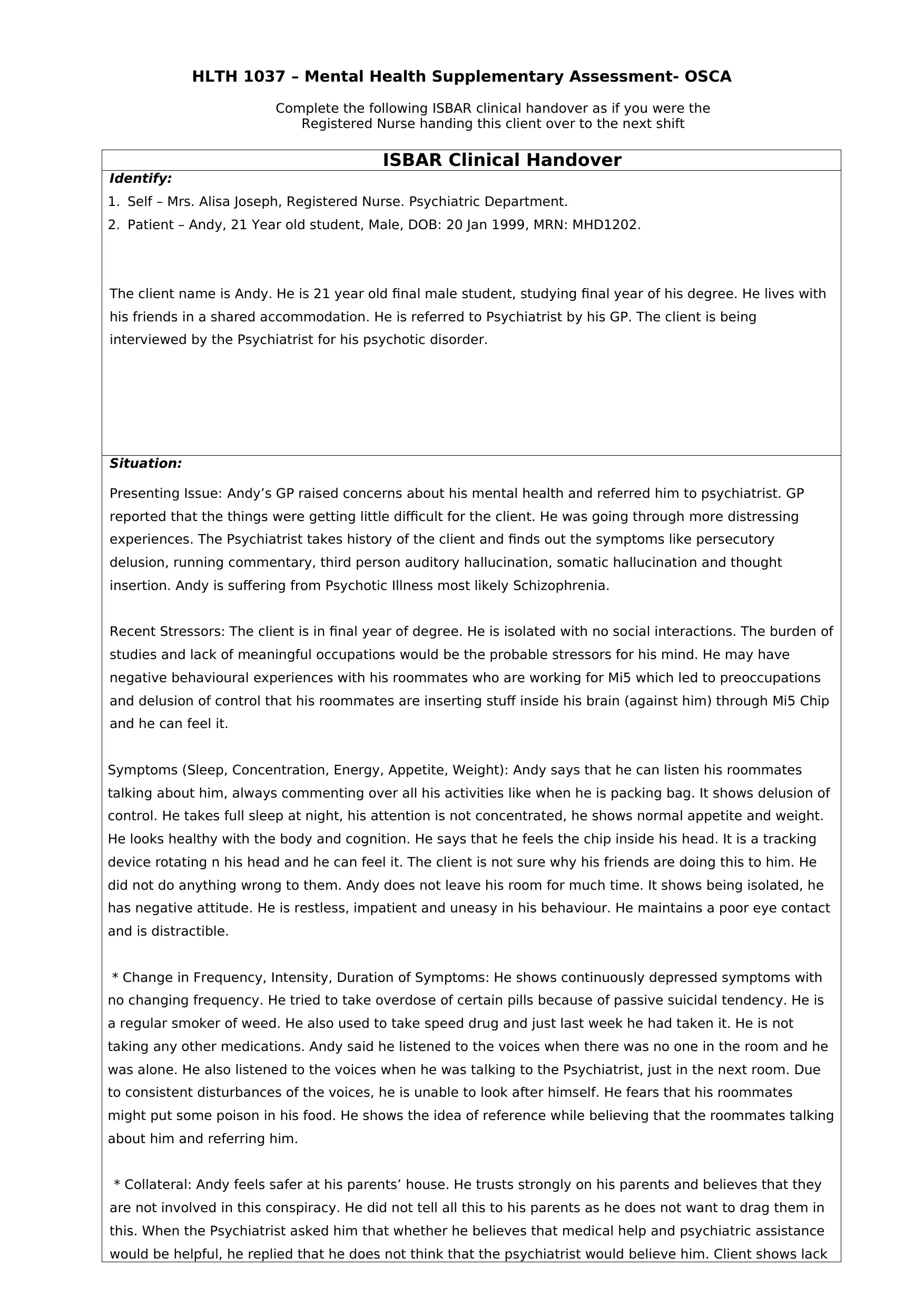
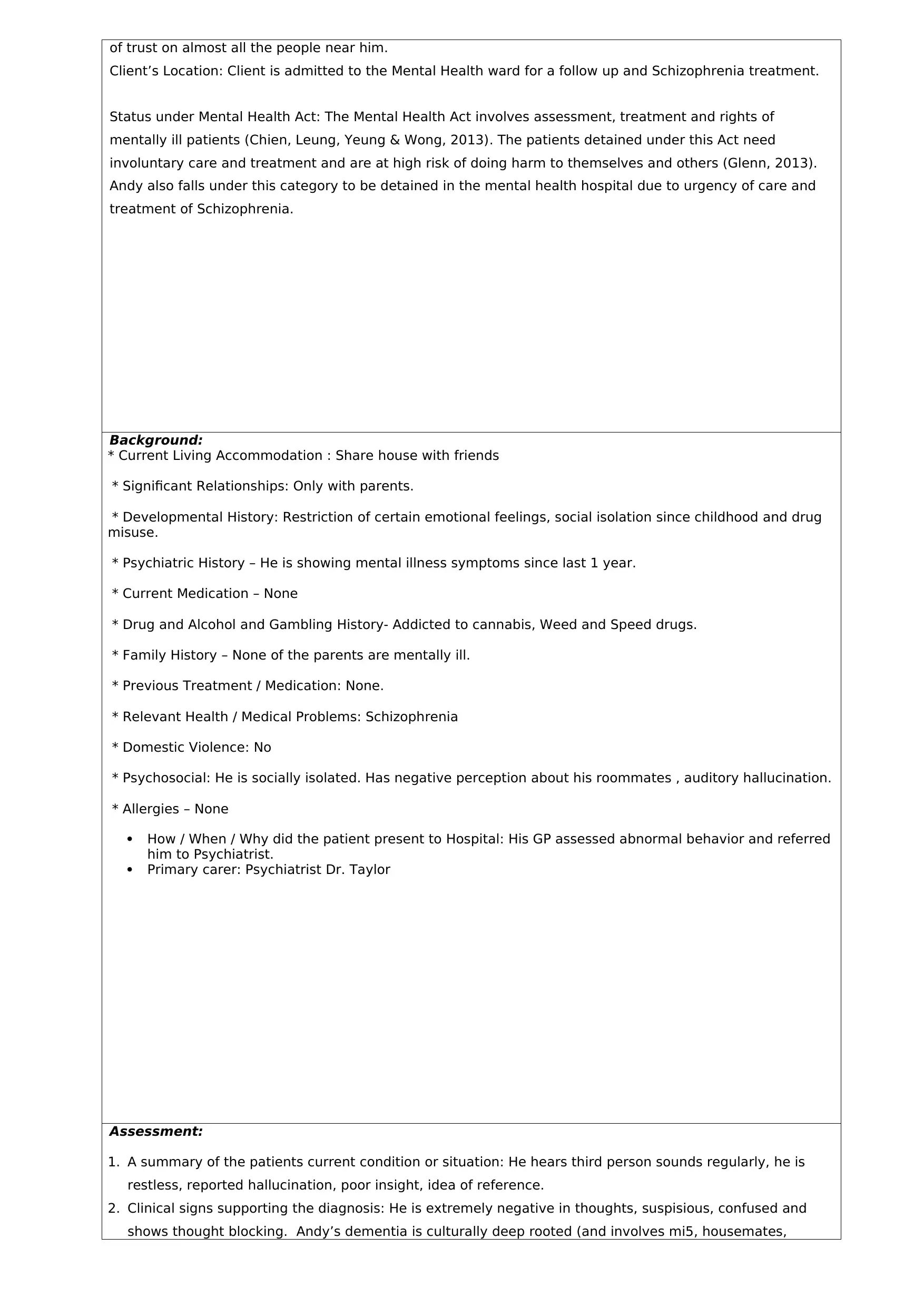
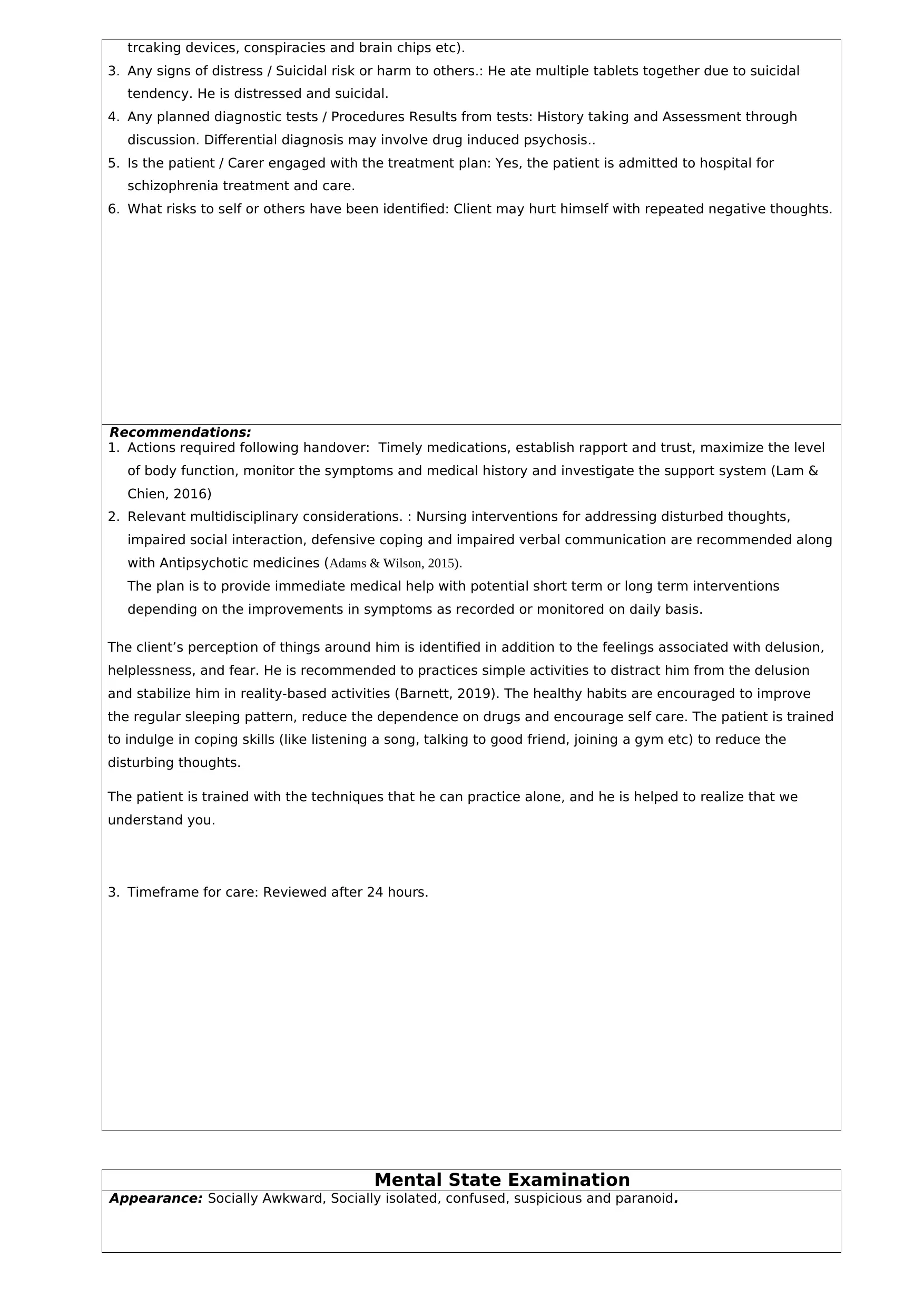
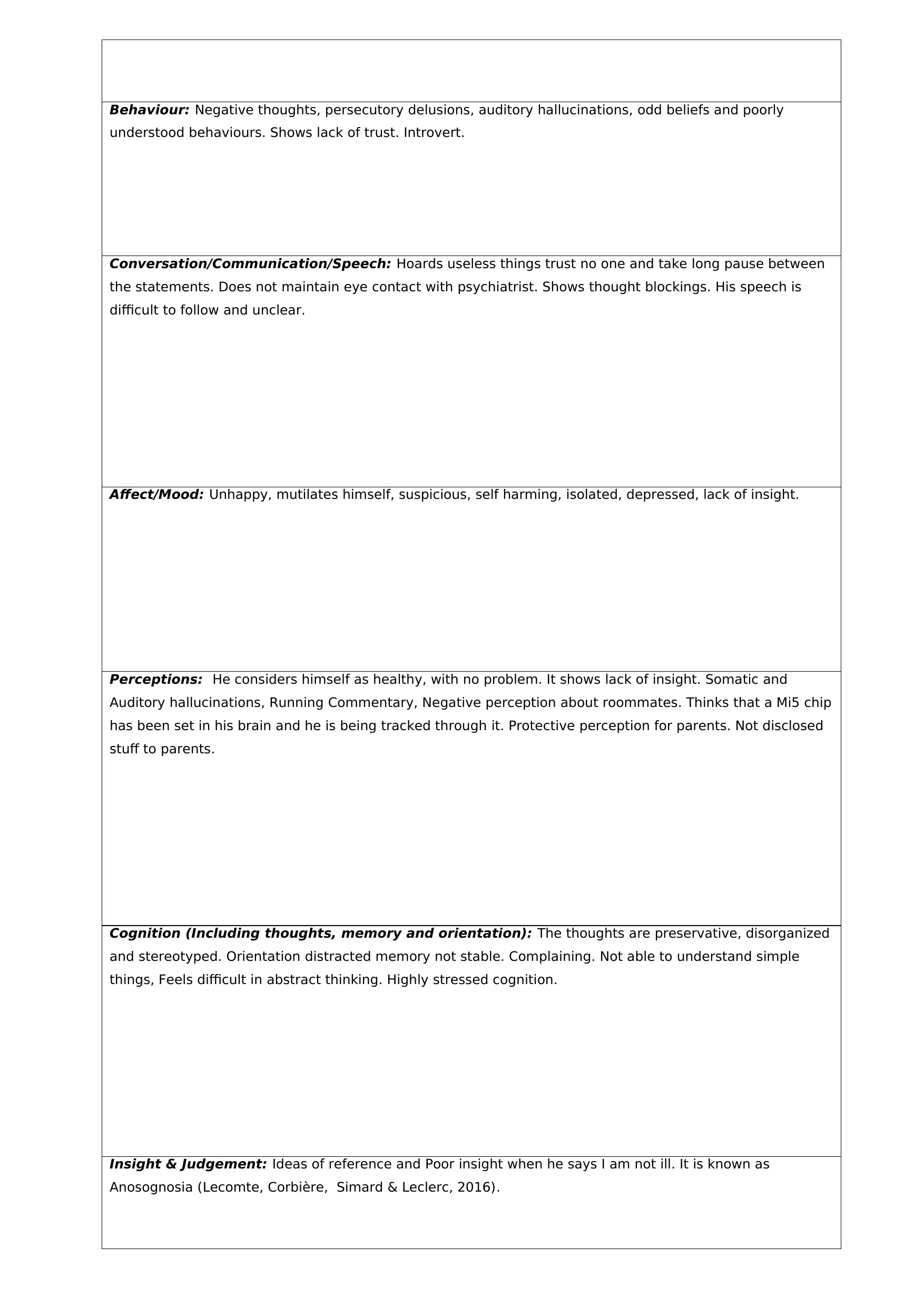
This document presents a comprehensive ISBAR (Identify, Situation, Background, Assessment, Recommendation) clinical handover scenario for a 21-year-old male student, Andy, diagnosed with schizophrenia. The handover, written from the perspective of a Registered Nurse, details the patient's presentation, including symptoms like persecutory delusions, auditory hallucinations, and thought insertion, alongside his history, current living situation, and medication use. The situation highlights the referral from his GP due to mental health concerns, with stressors including academic pressure and social isolation. The background provides developmental, psychiatric, drug use, and family history. The assessment includes a mental state examination and risk issues like suicidal ideation and self-harm. Recommendations involve timely medication, establishing trust, monitoring symptoms, and implementing multidisciplinary interventions. The document also references relevant research and nursing care guidelines to support the provided information. This is a detailed account of a patient's condition and the nursing care plan, designed to facilitate a smooth transition of care between shifts.

1 out of 6
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.