401017 Promoting Mental Health: Mental Status Examination Report
VerifiedAdded on 2022/08/28
|12
|2224
|19
Report
AI Summary
This report presents a mental status examination of a patient exhibiting symptoms of potential schizophrenia. The student analyzes the patient's appearance, behavior, affect, mood, speech, thought processes, content, perception, and cognitive functions based on a video observation. The analysis reveals potential risks, identifies schizophrenia as the clinical issue, and provides a rationale for the diagnosis. The report outlines both short-term and long-term goals for treatment, proposing nursing interventions such as social skills training, medication monitoring (specifically clozapine), and reality-oriented approaches to manage hallucinations. The report also discusses positive and negative interactions observed during the examination, referencing relevant literature to support the chosen interventions and their expected outcomes. The student emphasizes the importance of confidentiality and therapeutic communication in mental health care.

Running Head: MENTAL HEALTH
MENTAL STATUS EXAMINATION
Name of the Student
Name of the University
Author’s Note
MENTAL STATUS EXAMINATION
Name of the Student
Name of the University
Author’s Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1MENTAL HEALTH
Activity 1
APPEARANCE
The woman in the video had a wide built, was a little over weight and she looked tall even
though she was sitting. Her hair color was blonde and she looked hygienic but her hair was
slightly messy as it was wrapped in a bun. Her poise looked that she was fidgety, nervous and
she was wearing a spectacle. She was a white woman.
BEHAVIOUR
Her behavior was friendly and it looked like she not hesitant about sharing her thoughts and
dilemma. She showed psychomotor activities such as rubbing her hand constantly and talking
rapidly. She was keenly engaged in her conversation with the therapist.
AFFECT
Her emotional response was appropriate that suggested that she was not secretive or felt
awkward about her condition. She looked compatible with her therapist because she was
extremely descriptive about herself and she was sometimes interrupting her therapist to explain
more about herself.
MOOD
Her mood was positive as she was freely talking to the therapist without any inhibitions but she
was becoming absent minded in between conversations leading to fluctuations. The intensity of
her mood was moderate as she did not look very much tensed but she expressed it that she was
worried about herself. She was changing the topic in very short intervals when the therapist was
asking her questions.
Activity 1
APPEARANCE
The woman in the video had a wide built, was a little over weight and she looked tall even
though she was sitting. Her hair color was blonde and she looked hygienic but her hair was
slightly messy as it was wrapped in a bun. Her poise looked that she was fidgety, nervous and
she was wearing a spectacle. She was a white woman.
BEHAVIOUR
Her behavior was friendly and it looked like she not hesitant about sharing her thoughts and
dilemma. She showed psychomotor activities such as rubbing her hand constantly and talking
rapidly. She was keenly engaged in her conversation with the therapist.
AFFECT
Her emotional response was appropriate that suggested that she was not secretive or felt
awkward about her condition. She looked compatible with her therapist because she was
extremely descriptive about herself and she was sometimes interrupting her therapist to explain
more about herself.
MOOD
Her mood was positive as she was freely talking to the therapist without any inhibitions but she
was becoming absent minded in between conversations leading to fluctuations. The intensity of
her mood was moderate as she did not look very much tensed but she expressed it that she was
worried about herself. She was changing the topic in very short intervals when the therapist was
asking her questions.
2MENTAL HEALTH
SPEECH
The quantity of her speech was on a higher scale as she was talking in a fast pace. Her volume
was moderately high and it looked like she was in a hurry to complete what she was talking
about. Her tone was changing according to what she was saying, which also indicated her change
of mood.
THOUGHT FORM
The process of her thought was all haywire because she was forgetting what she was talking
about in a moment because she was talking about another subject in the other moment. She was
erratic and it was becoming confusing for the therapist as there was no synchronization in her
story. Her thoughts also looked vague because she was thinking that she was heir to the throne of
England (Horga et al., 2014).
THOUGHT CONTENT
She was thinking and becoming paranoid about people around her because she thought that they
know that she is the daughter of King Charles. She said that even Diana knew and that is why
she was dead so even her life was in danger if come to know. She was delusional about the
reality as she said that her parents adopted her and her real parents were in England.
PERCEPTION
Her speech showed that she was hallucinating. One of its kind of kinaesthetic because she said
that she could ants in her brains, which means that she felt physical sensations that was not even
happening. She addressed the ants in her brains twice that suggested that it was something
constant.
SPEECH
The quantity of her speech was on a higher scale as she was talking in a fast pace. Her volume
was moderately high and it looked like she was in a hurry to complete what she was talking
about. Her tone was changing according to what she was saying, which also indicated her change
of mood.
THOUGHT FORM
The process of her thought was all haywire because she was forgetting what she was talking
about in a moment because she was talking about another subject in the other moment. She was
erratic and it was becoming confusing for the therapist as there was no synchronization in her
story. Her thoughts also looked vague because she was thinking that she was heir to the throne of
England (Horga et al., 2014).
THOUGHT CONTENT
She was thinking and becoming paranoid about people around her because she thought that they
know that she is the daughter of King Charles. She said that even Diana knew and that is why
she was dead so even her life was in danger if come to know. She was delusional about the
reality as she said that her parents adopted her and her real parents were in England.
PERCEPTION
Her speech showed that she was hallucinating. One of its kind of kinaesthetic because she said
that she could ants in her brains, which means that she felt physical sensations that was not even
happening. She addressed the ants in her brains twice that suggested that it was something
constant.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3MENTAL HEALTH
COGNITION & INTELLECTUAL FUNCTIONING
Her orientation was proper as she was correct about the time and date. She was also aware that
she was taking mental help and she was visiting a therapist for some previous condition. Her
concentration and attention span was weak as she was not answering all the questions.
INSIGHT & JUDGEMENT
She was unaware about her problem because she was not able to understand that what she is
saying is far away from reality. She was in a denial that she is mentally fine and she does not
need any help from the medical experts as she was not realizing the consequences of her
behavior (Hamm & Firmin, 2016).
Risks
The 4 risks identified in her case is major psychiatric illness, diagnosed personality disorder,
intellectual disability/cognitive deficits, and impulsive behavior. All these are risks factors that
were triggered during the interview as she was not aware about the reality and she thought she
was mentally fit (Fleischhacker & Uchida, 2014).
Activity 2
CLINICAL ISSUE
COGNITION & INTELLECTUAL FUNCTIONING
Her orientation was proper as she was correct about the time and date. She was also aware that
she was taking mental help and she was visiting a therapist for some previous condition. Her
concentration and attention span was weak as she was not answering all the questions.
INSIGHT & JUDGEMENT
She was unaware about her problem because she was not able to understand that what she is
saying is far away from reality. She was in a denial that she is mentally fine and she does not
need any help from the medical experts as she was not realizing the consequences of her
behavior (Hamm & Firmin, 2016).
Risks
The 4 risks identified in her case is major psychiatric illness, diagnosed personality disorder,
intellectual disability/cognitive deficits, and impulsive behavior. All these are risks factors that
were triggered during the interview as she was not aware about the reality and she thought she
was mentally fit (Fleischhacker & Uchida, 2014).
Activity 2
CLINICAL ISSUE
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4MENTAL HEALTH
According to the interactions and conversation in the video it is evident that she is having
hallucinations. She mentioned a medicine that she was consuming, which she stopped because
she felt it was causing her gain weight. The name of the medicine was clozapine, which is given
for psychotic issues such as schizophrenia (Siskind et al., 2018). The clinical issue she is
suffering from is schizophrenia.
RATIONALE FOR CHOSEN ISSUE
The reason for choosing this issue is because it is a severe mental disorder and it can influence
her life. If condition is not treated then it can elevate to a level where it will be difficult to control
her symptoms of hallucination. It can even lead to physically harming others who will not agree
with her delusions. It is a threat to her wellbeing if her symptoms continue. The information she
shared was that she was taking a medicine called clozapine and it is mostly used to treat
schizophrenia. She said that she was the daughter of King Charles and Camilla, which is not a
positive sign for her mental condition. She wants people to know about her lineage and
acknowledge it, and this thought can trigger behaviour that can harm other people as she thinks
that people might try to harm her if they come to know about this. This is the major reason for
choosing schizophrenia as an issue because it is root cause of all her inappropriate behaviour.
GOAL/S
A significant goal for treating this mental disorder is to reduce the symptoms that elevates if it is
not looked after because this condition has no cure. It can be only maintained with treatment and
medication. The long term goals are to prevent the elevation of the symptoms, improving quality
According to the interactions and conversation in the video it is evident that she is having
hallucinations. She mentioned a medicine that she was consuming, which she stopped because
she felt it was causing her gain weight. The name of the medicine was clozapine, which is given
for psychotic issues such as schizophrenia (Siskind et al., 2018). The clinical issue she is
suffering from is schizophrenia.
RATIONALE FOR CHOSEN ISSUE
The reason for choosing this issue is because it is a severe mental disorder and it can influence
her life. If condition is not treated then it can elevate to a level where it will be difficult to control
her symptoms of hallucination. It can even lead to physically harming others who will not agree
with her delusions. It is a threat to her wellbeing if her symptoms continue. The information she
shared was that she was taking a medicine called clozapine and it is mostly used to treat
schizophrenia. She said that she was the daughter of King Charles and Camilla, which is not a
positive sign for her mental condition. She wants people to know about her lineage and
acknowledge it, and this thought can trigger behaviour that can harm other people as she thinks
that people might try to harm her if they come to know about this. This is the major reason for
choosing schizophrenia as an issue because it is root cause of all her inappropriate behaviour.
GOAL/S
A significant goal for treating this mental disorder is to reduce the symptoms that elevates if it is
not looked after because this condition has no cure. It can be only maintained with treatment and
medication. The long term goals are to prevent the elevation of the symptoms, improving quality
5MENTAL HEALTH
of life and enhance the function of psychosocial aspect. Schizophrenia disrupts the cognition,
thought and motor performance, which has to be treated through certain interventions.
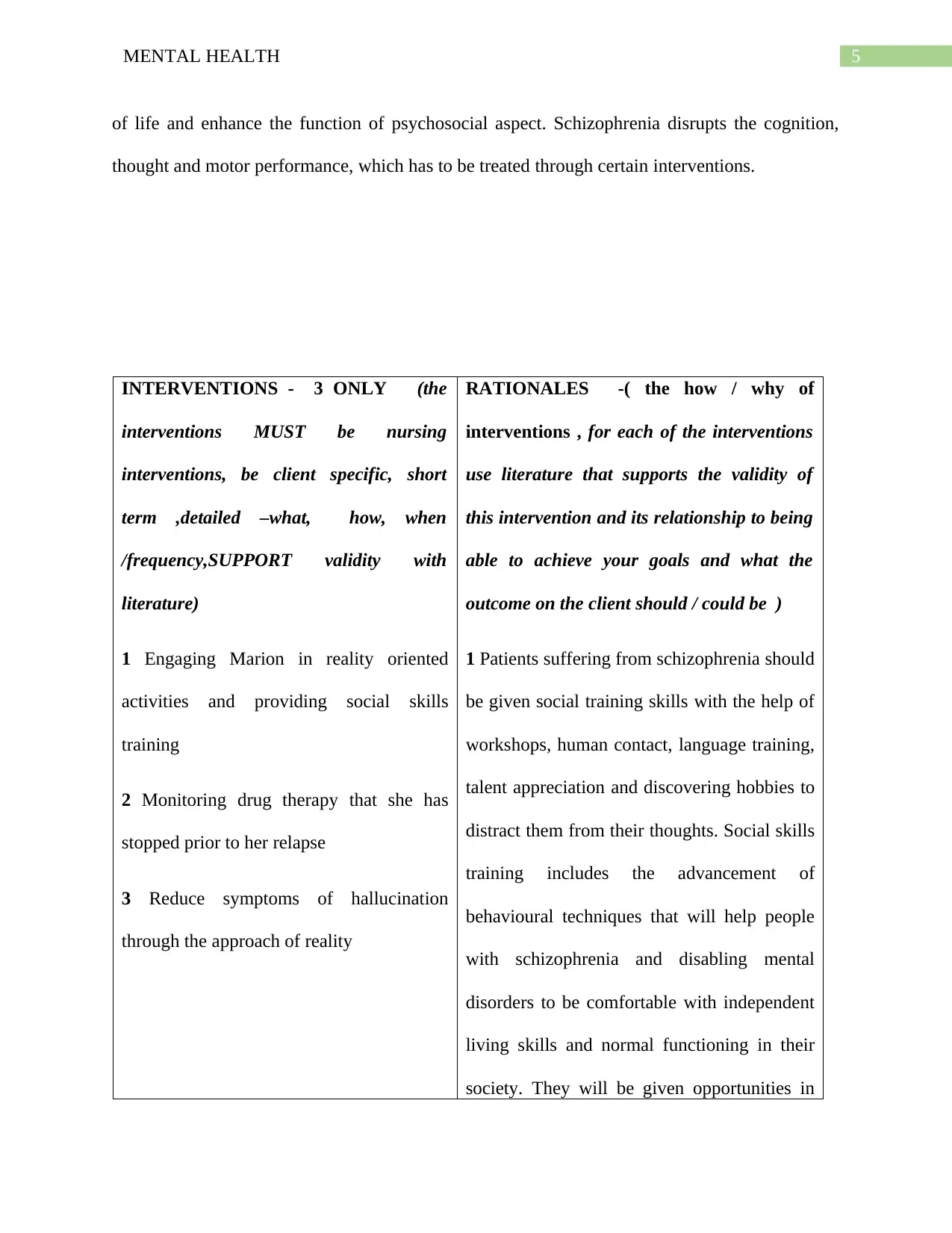
INTERVENTIONS - 3 ONLY (the
interventions MUST be nursing
interventions, be client specific, short
term ,detailed –what, how, when
/frequency,SUPPORT validity with
literature)
1 Engaging Marion in reality oriented
activities and providing social skills
training
2 Monitoring drug therapy that she has
stopped prior to her relapse
3 Reduce symptoms of hallucination
through the approach of reality
RATIONALES -( the how / why of
interventions , for each of the interventions
use literature that supports the validity of
this intervention and its relationship to being
able to achieve your goals and what the
outcome on the client should / could be )
1 Patients suffering from schizophrenia should
be given social training skills with the help of
workshops, human contact, language training,
talent appreciation and discovering hobbies to
distract them from their thoughts. Social skills
training includes the advancement of
behavioural techniques that will help people
with schizophrenia and disabling mental
disorders to be comfortable with independent
living skills and normal functioning in their
society. They will be given opportunities in
of life and enhance the function of psychosocial aspect. Schizophrenia disrupts the cognition,
thought and motor performance, which has to be treated through certain interventions.
INTERVENTIONS - 3 ONLY (the
interventions MUST be nursing
interventions, be client specific, short
term ,detailed –what, how, when
/frequency,SUPPORT validity with
literature)
1 Engaging Marion in reality oriented
activities and providing social skills
training
2 Monitoring drug therapy that she has
stopped prior to her relapse
3 Reduce symptoms of hallucination
through the approach of reality
RATIONALES -( the how / why of
interventions , for each of the interventions
use literature that supports the validity of
this intervention and its relationship to being
able to achieve your goals and what the
outcome on the client should / could be )
1 Patients suffering from schizophrenia should
be given social training skills with the help of
workshops, human contact, language training,
talent appreciation and discovering hobbies to
distract them from their thoughts. Social skills
training includes the advancement of
behavioural techniques that will help people
with schizophrenia and disabling mental
disorders to be comfortable with independent
living skills and normal functioning in their
society. They will be given opportunities in
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6MENTAL HEALTH
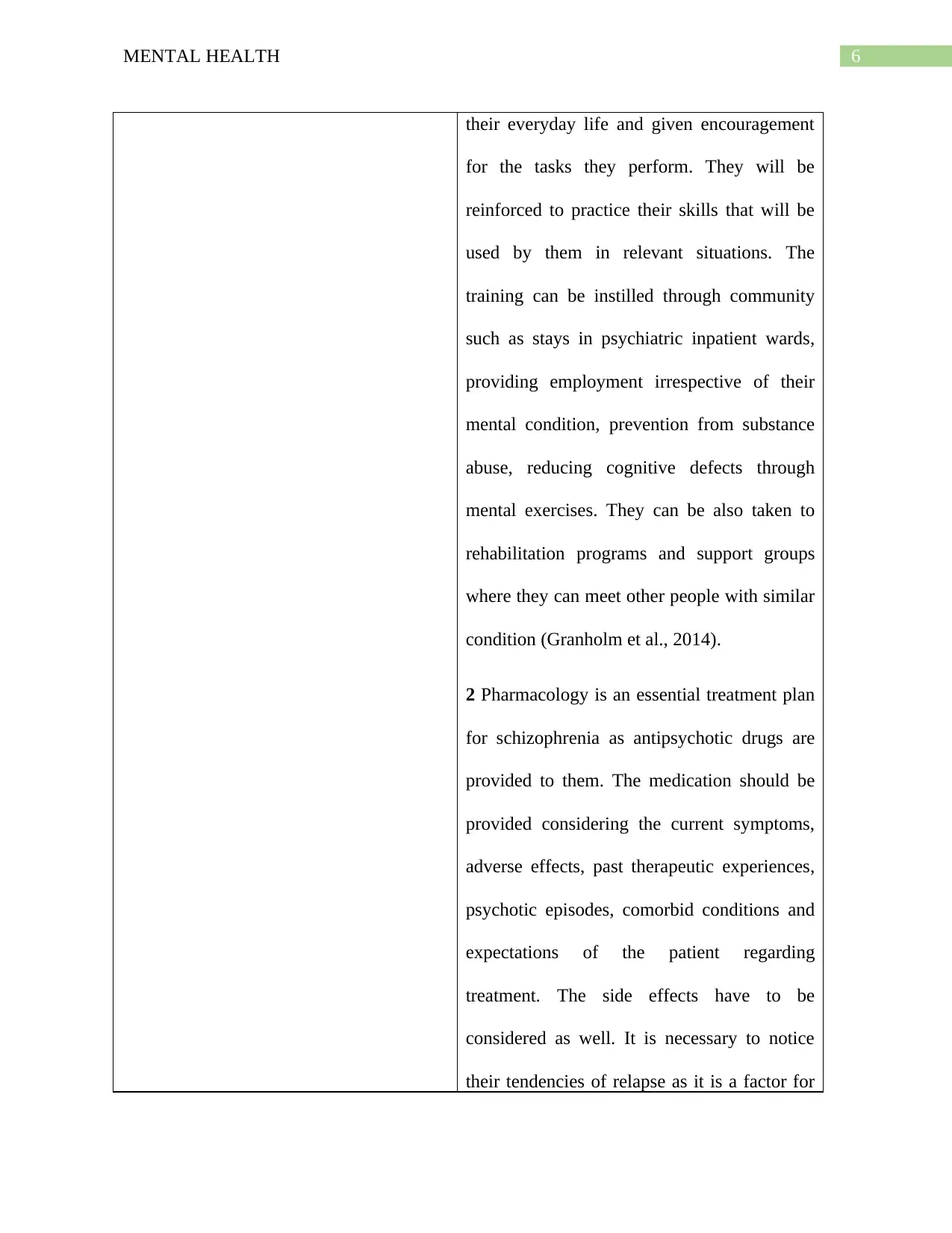
their everyday life and given encouragement
for the tasks they perform. They will be
reinforced to practice their skills that will be
used by them in relevant situations. The
training can be instilled through community
such as stays in psychiatric inpatient wards,
providing employment irrespective of their
mental condition, prevention from substance
abuse, reducing cognitive defects through
mental exercises. They can be also taken to
rehabilitation programs and support groups
where they can meet other people with similar
condition (Granholm et al., 2014).
2 Pharmacology is an essential treatment plan
for schizophrenia as antipsychotic drugs are
provided to them. The medication should be
provided considering the current symptoms,
adverse effects, past therapeutic experiences,
psychotic episodes, comorbid conditions and
expectations of the patient regarding
treatment. The side effects have to be
considered as well. It is necessary to notice
their tendencies of relapse as it is a factor for
their everyday life and given encouragement
for the tasks they perform. They will be
reinforced to practice their skills that will be
used by them in relevant situations. The
training can be instilled through community
such as stays in psychiatric inpatient wards,
providing employment irrespective of their
mental condition, prevention from substance
abuse, reducing cognitive defects through
mental exercises. They can be also taken to
rehabilitation programs and support groups
where they can meet other people with similar
condition (Granholm et al., 2014).
2 Pharmacology is an essential treatment plan
for schizophrenia as antipsychotic drugs are
provided to them. The medication should be
provided considering the current symptoms,
adverse effects, past therapeutic experiences,
psychotic episodes, comorbid conditions and
expectations of the patient regarding
treatment. The side effects have to be
considered as well. It is necessary to notice
their tendencies of relapse as it is a factor for
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7MENTAL HEALTH
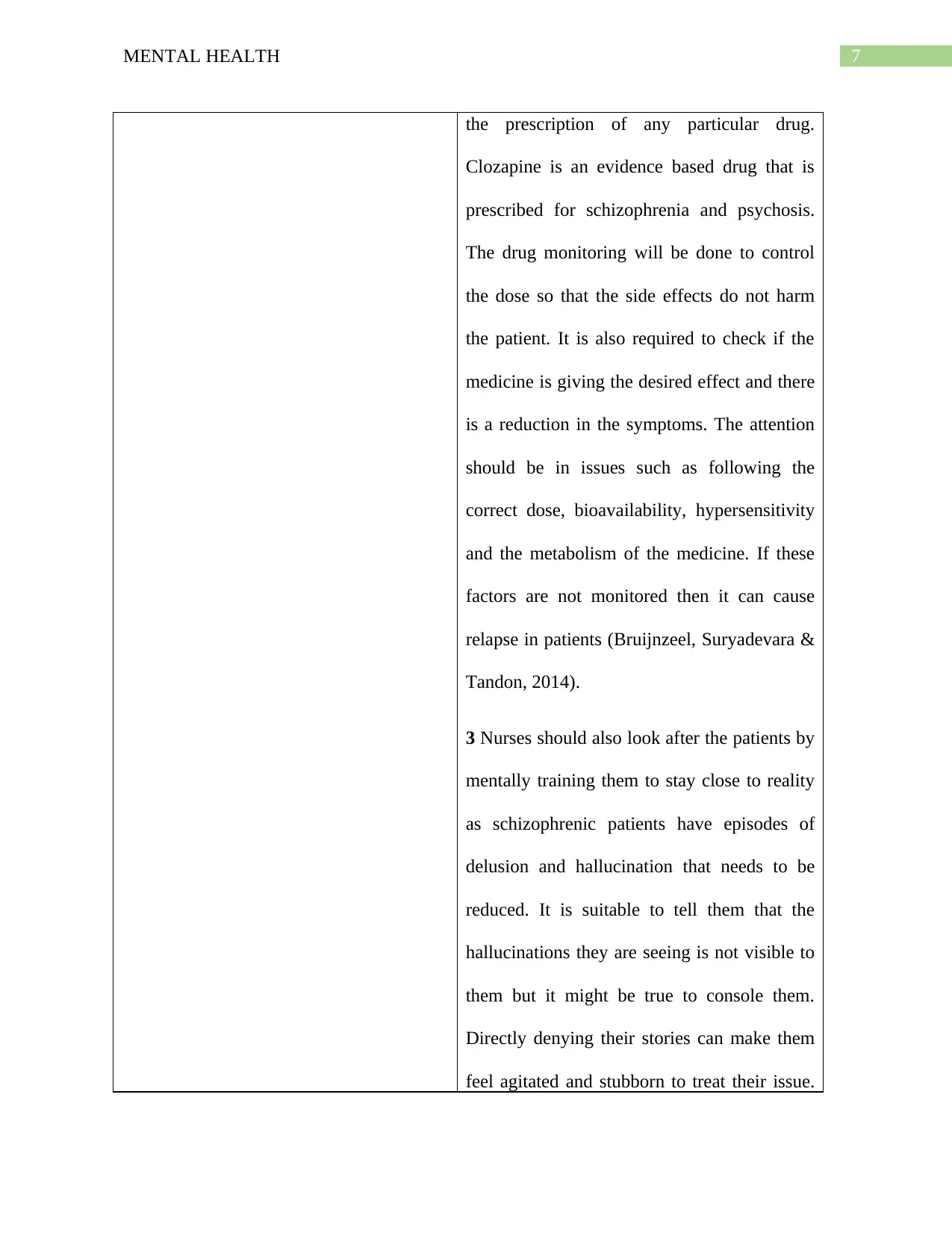
the prescription of any particular drug.
Clozapine is an evidence based drug that is
prescribed for schizophrenia and psychosis.
The drug monitoring will be done to control
the dose so that the side effects do not harm
the patient. It is also required to check if the
medicine is giving the desired effect and there
is a reduction in the symptoms. The attention
should be in issues such as following the
correct dose, bioavailability, hypersensitivity
and the metabolism of the medicine. If these
factors are not monitored then it can cause
relapse in patients (Bruijnzeel, Suryadevara &
Tandon, 2014).
3 Nurses should also look after the patients by
mentally training them to stay close to reality
as schizophrenic patients have episodes of
delusion and hallucination that needs to be
reduced. It is suitable to tell them that the
hallucinations they are seeing is not visible to
them but it might be true to console them.
Directly denying their stories can make them
feel agitated and stubborn to treat their issue.
the prescription of any particular drug.
Clozapine is an evidence based drug that is
prescribed for schizophrenia and psychosis.
The drug monitoring will be done to control
the dose so that the side effects do not harm
the patient. It is also required to check if the
medicine is giving the desired effect and there
is a reduction in the symptoms. The attention
should be in issues such as following the
correct dose, bioavailability, hypersensitivity
and the metabolism of the medicine. If these
factors are not monitored then it can cause
relapse in patients (Bruijnzeel, Suryadevara &
Tandon, 2014).
3 Nurses should also look after the patients by
mentally training them to stay close to reality
as schizophrenic patients have episodes of
delusion and hallucination that needs to be
reduced. It is suitable to tell them that the
hallucinations they are seeing is not visible to
them but it might be true to console them.
Directly denying their stories can make them
feel agitated and stubborn to treat their issue.
8MENTAL HEALTH
They should be given psychological education
about their condition so that precautionary
measures are taken by them to condition their
cognitive abilities (Cheng & Schepp, 2016).
Activity 3
Four positive interactions
The first positive interaction was when she explained to Marion that this session will be
confidential and the information will not be leaked to other parties, which is an essential
protocol for mental health care.
She was constantly questioning, which is an essential component of therapeutic
communication as it will give her more idea about her mental state. She kept asking
Marion about her hallucinations and if she was aware that of any voices in her ears.
The therapist indulged her into mental math exercise, which is a technique to know about
her cognitive abilities. This will also make Marion forget about her delusions and make
her come close to reality.
The therapist did not deny any of her delusions as it would increase her agitation and
symptoms of schizophrenia, which is not preferable during a counselling session
especially for a schizophrenic patient as they have strong opinions about their
hallucinations.
2 negative interactions
They should be given psychological education
about their condition so that precautionary
measures are taken by them to condition their
cognitive abilities (Cheng & Schepp, 2016).
Activity 3
Four positive interactions
The first positive interaction was when she explained to Marion that this session will be
confidential and the information will not be leaked to other parties, which is an essential
protocol for mental health care.
She was constantly questioning, which is an essential component of therapeutic
communication as it will give her more idea about her mental state. She kept asking
Marion about her hallucinations and if she was aware that of any voices in her ears.
The therapist indulged her into mental math exercise, which is a technique to know about
her cognitive abilities. This will also make Marion forget about her delusions and make
her come close to reality.
The therapist did not deny any of her delusions as it would increase her agitation and
symptoms of schizophrenia, which is not preferable during a counselling session
especially for a schizophrenic patient as they have strong opinions about their
hallucinations.
2 negative interactions
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9MENTAL HEALTH
She was constantly asking about the voices in her head, which should not have happened
because she has schizophrenia and it can trigger her to feel that she is mentally disabled.
She discussed with Marion about her further treatment that will be discussed with other
medical experts. This is not an appropriate behavior because Marion should not feel that
she is suffering from psychosis (Siskind et al., 2016).
She was constantly asking about the voices in her head, which should not have happened
because she has schizophrenia and it can trigger her to feel that she is mentally disabled.
She discussed with Marion about her further treatment that will be discussed with other
medical experts. This is not an appropriate behavior because Marion should not feel that
she is suffering from psychosis (Siskind et al., 2016).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10MENTAL HEALTH
References
Bruijnzeel, D., Suryadevara, U., & Tandon, R. (2014). Antipsychotic treatment of schizophrenia:
an update. Asian journal of psychiatry, 11, 3-7.
Cheng, S. C., & Schepp, K. G. (2016). Early intervention in schizophrenia: a literature
review. Archives of psychiatric nursing, 30(6), 774-781.
Fleischhacker, W. W., & Uchida, H. (2014). Critical review of antipsychotic polypharmacy in
the treatment of schizophrenia. International Journal of
Neuropsychopharmacology, 17(7), 1083-1093.
Granholm, E., Holden, J., Link, P. C., & McQuaid, J. R. (2014). Randomized clinical trial of
cognitive behavioral social skills training for schizophrenia: Improvement in functioning
and experiential negative symptoms. Journal of consulting and clinical
psychology, 82(6), 1173.
Hamm, J. A., & Firmin, R. L. (2016). Disorganization and individual psychotherapy for
schizophrenia: a case report of metacognitive reflection and insight therapy. Journal of
Contemporary Psychotherapy, 46(4), 227-234.
Horga, G., Schatz, K. C., Abi-Dargham, A., & Peterson, B. S. (2014). Deficits in predictive
coding underlie hallucinations in schizophrenia. Journal of Neuroscience, 34(24), 8072-
8082.
Siskind, D. J., Lee, M., Ravindran, A., Zhang, Q., Ma, E., Motamarri, B., & Kisely, S. (2018).
Augmentation strategies for clozapine refractory schizophrenia: a systematic review and
meta-analysis. Australian & New Zealand Journal of Psychiatry, 52(8), 751-767.
References
Bruijnzeel, D., Suryadevara, U., & Tandon, R. (2014). Antipsychotic treatment of schizophrenia:
an update. Asian journal of psychiatry, 11, 3-7.
Cheng, S. C., & Schepp, K. G. (2016). Early intervention in schizophrenia: a literature
review. Archives of psychiatric nursing, 30(6), 774-781.
Fleischhacker, W. W., & Uchida, H. (2014). Critical review of antipsychotic polypharmacy in
the treatment of schizophrenia. International Journal of
Neuropsychopharmacology, 17(7), 1083-1093.
Granholm, E., Holden, J., Link, P. C., & McQuaid, J. R. (2014). Randomized clinical trial of
cognitive behavioral social skills training for schizophrenia: Improvement in functioning
and experiential negative symptoms. Journal of consulting and clinical
psychology, 82(6), 1173.
Hamm, J. A., & Firmin, R. L. (2016). Disorganization and individual psychotherapy for
schizophrenia: a case report of metacognitive reflection and insight therapy. Journal of
Contemporary Psychotherapy, 46(4), 227-234.
Horga, G., Schatz, K. C., Abi-Dargham, A., & Peterson, B. S. (2014). Deficits in predictive
coding underlie hallucinations in schizophrenia. Journal of Neuroscience, 34(24), 8072-
8082.
Siskind, D. J., Lee, M., Ravindran, A., Zhang, Q., Ma, E., Motamarri, B., & Kisely, S. (2018).
Augmentation strategies for clozapine refractory schizophrenia: a systematic review and
meta-analysis. Australian & New Zealand Journal of Psychiatry, 52(8), 751-767.
11MENTAL HEALTH
Siskind, D., McCartney, L., Goldschlager, R., & Kisely, S. (2016). Clozapine v. first-and second-
generation antipsychotics in treatment-refractory schizophrenia: systematic review and
meta-analysis. The British Journal of Psychiatry, 209(5), 385-392.
Siskind, D., McCartney, L., Goldschlager, R., & Kisely, S. (2016). Clozapine v. first-and second-
generation antipsychotics in treatment-refractory schizophrenia: systematic review and
meta-analysis. The British Journal of Psychiatry, 209(5), 385-392.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.