Case Study Analysis: Mrs. Gwen Boren's Nursing Assessment Report
VerifiedAdded on 2022/08/21
|5
|2418
|31
Report
AI Summary
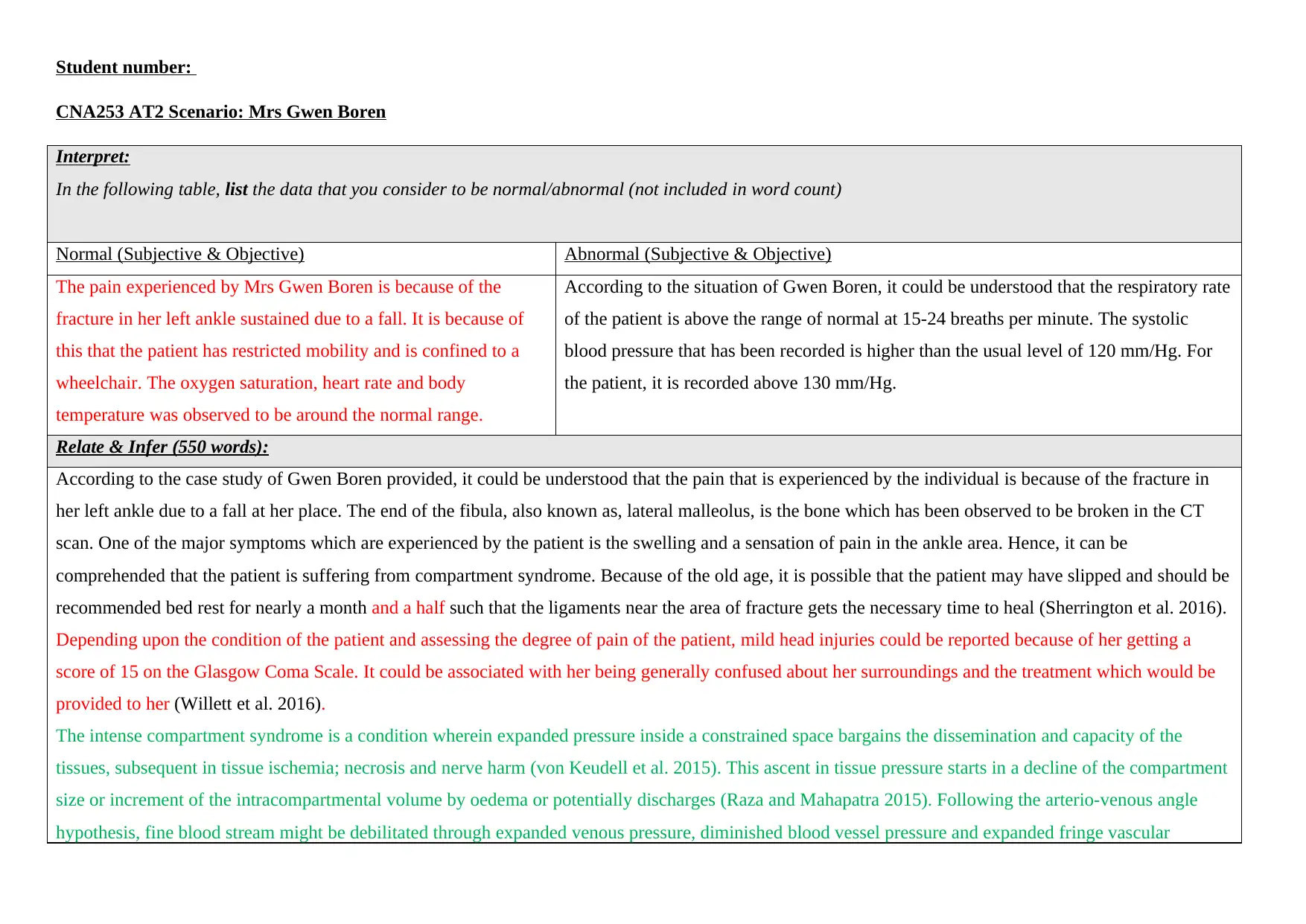
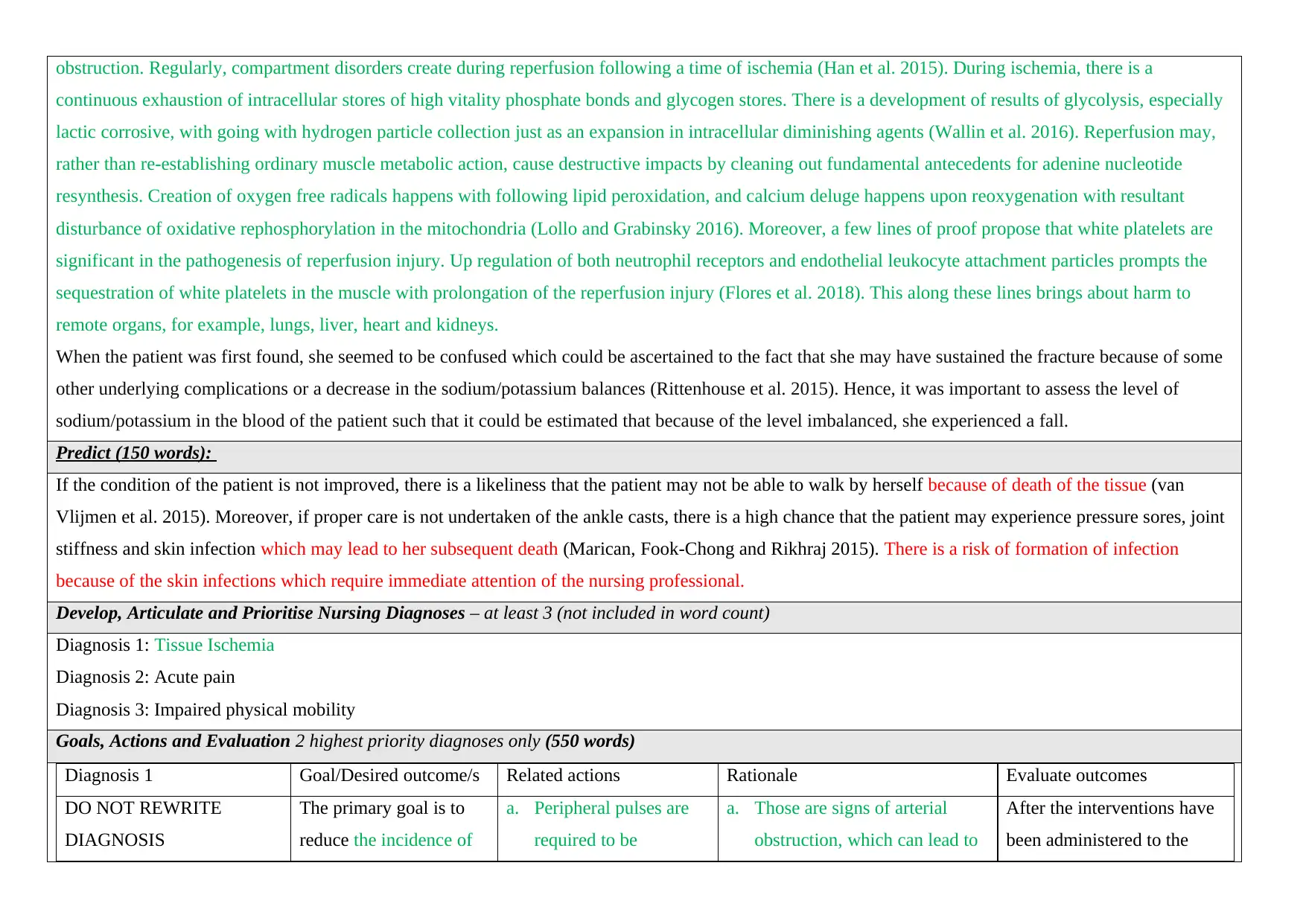
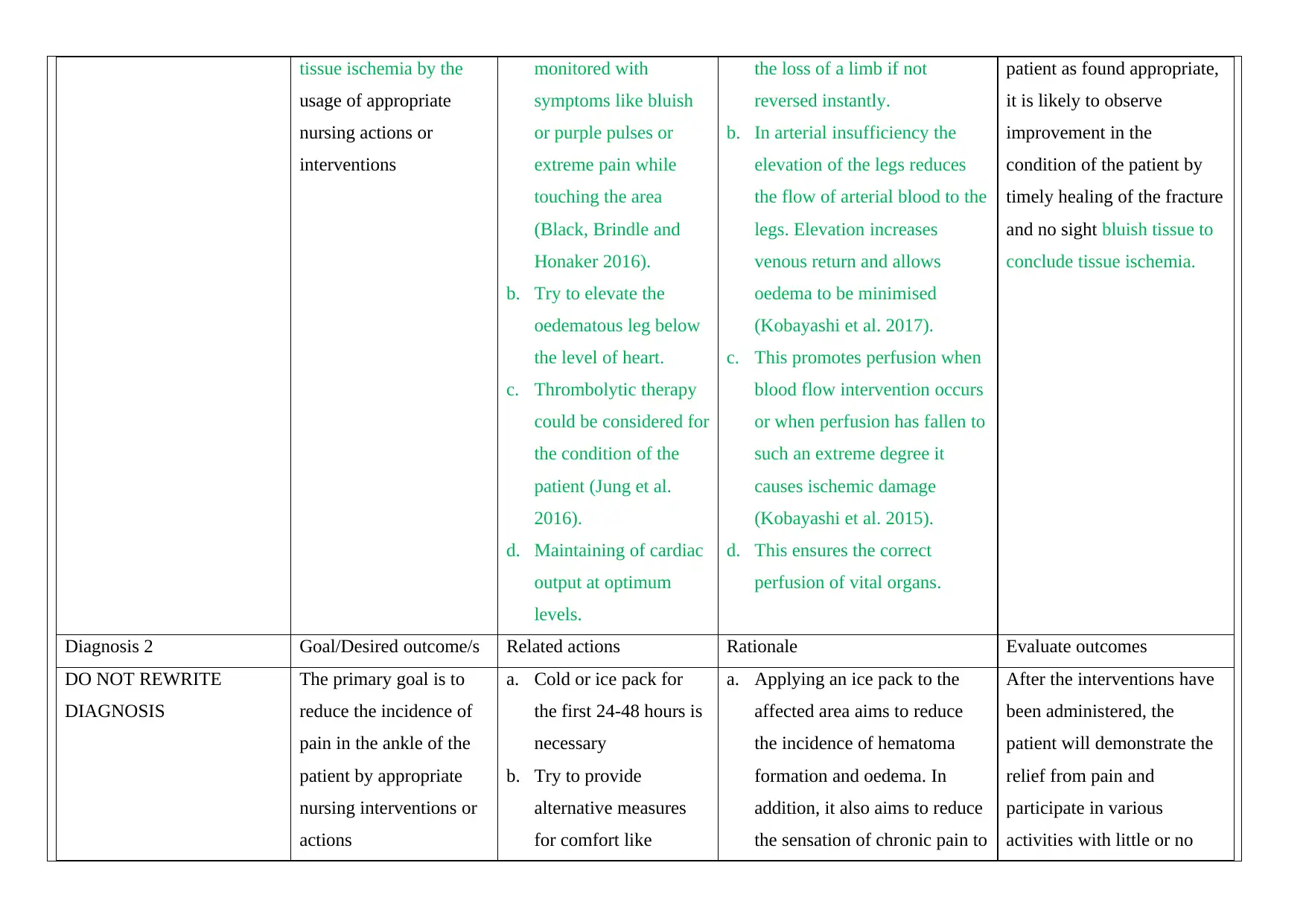
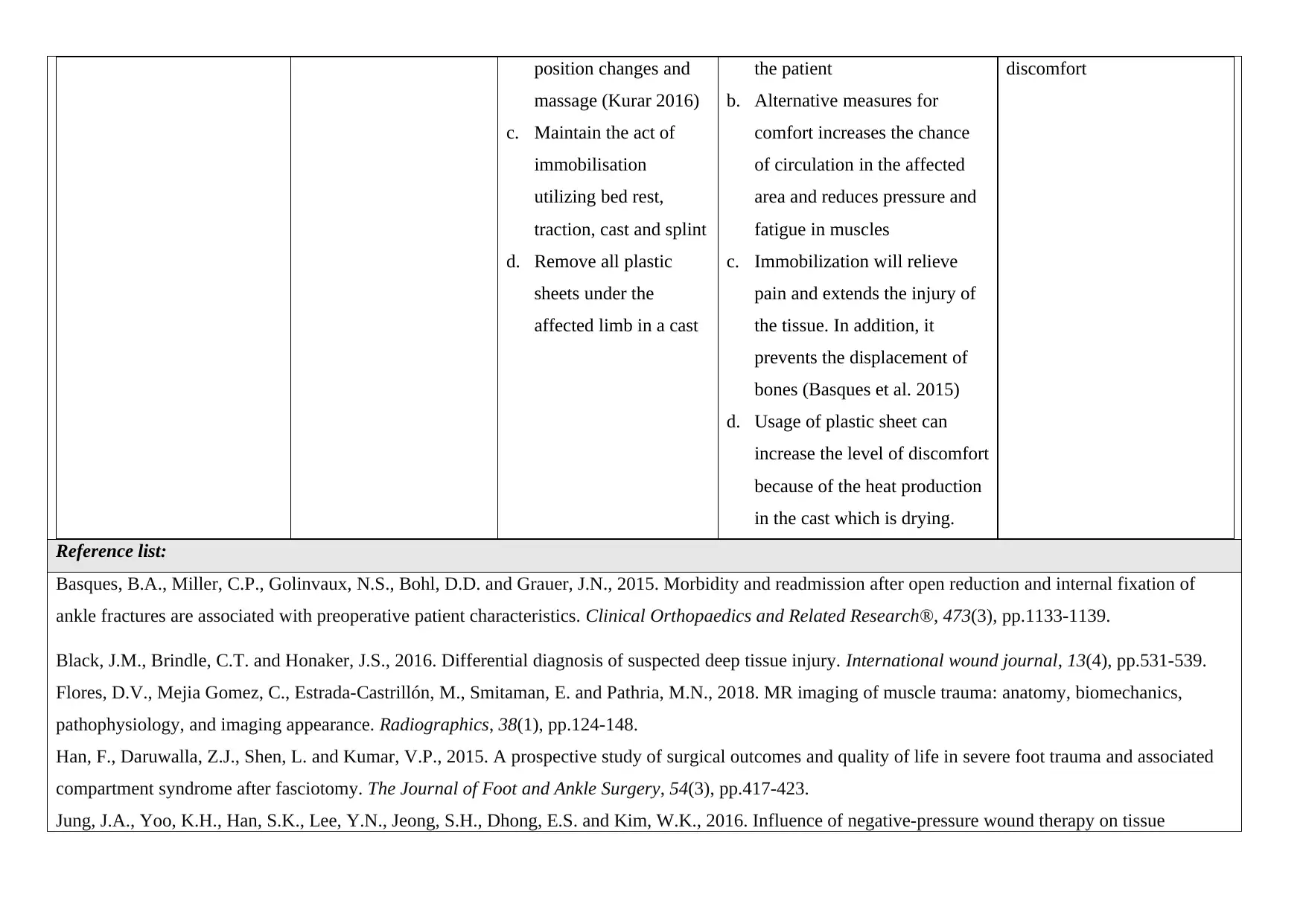
This report presents a comprehensive analysis of Mrs. Gwen Boren's nursing case study. The assignment begins with an interpretation of the patient's condition, identifying both normal and abnormal subjective and objective data based on the provided scenario. It then delves into a detailed relate and infer section, discussing the patient's fracture, potential compartment syndrome, and mild head injuries. The report also includes a prediction of potential complications if the patient's condition is not improved. Furthermore, it develops, articulates, and prioritizes nursing diagnoses, focusing on tissue ischemia, acute pain, and impaired physical mobility. The core of the report lies in the goals, actions, and evaluation sections for the two highest priority diagnoses, outlining related nursing interventions, rationales, and expected outcomes. The assignment is supported by a reference list of relevant academic sources.
1 out of 5
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.