Integrative Review: Exercise, Education, Rehabilitation & MS Impact
VerifiedAdded on 2023/04/21
|20
|6812
|61
Literature Review
AI Summary
This literature review investigates the role of exercise, rehabilitation, education, and consultation in managing Multiple Sclerosis (MS). Chapter one introduces MS, its global context, and the importance of exercise and education in rehabilitation. It highlights that MS is a chronic autoimmune disorder affecting the central nervous system, impacting movement, sensation, and bodily functions, with a significant prevalence in young adults. Chapter two reviews existing literature on the impact of exercise, rehabilitation, education, and consultation on people with MS, noting the benefits and barriers to exercise participation, the importance of rehabilitation programs, and the effectiveness of clinical consultations. The review identifies gaps in understanding the determinants of physical exercise engagement among MS patients and emphasizes the need for further research to clarify the effects of regular physical exercise on psychological variables and quality of life. The review aims to determine the impact of these interventions on people with MS and to justify barriers to exercise engagement, as well as the effectiveness of rehabilitation and consultative programs.
CHAPTER ONE: INTRODUCTION
1.0 Introduction
This chapter will cover a general introduction to the research topic. The importance of
exercise and education would be explained in the context of rehabilitation. A definition of
Multiple Sclerosis will be provided and the international context of MS will be covered in
this chapter with some statistics and interventions available for people with MS. This chapter
will also provide a summary of the three key issues related to this research which are
Exercise, Rehabilitation, Education, Consultation, and Multiple Sclerosis.
1.1 Overview
Multiple Sclerosis (MS) can be defined as a chronic disorder affecting movement, the
feeling of sensation along with bodily functions (MS-UK, 2019). It is an autoimmune
inflammatory disorder that affects the central nervous system (Comi, Filippi, Wolinsky, &
Group, 2001; Matute-Blanch, Montalban, & Comabella, 2018). The vital organs that can be
affected by multiple sclerosis include myelin which helps to send and pass electrical signals
quickly between the brain and the other body organs (Podbielska, Banik, Kurowska, &
Hogan, 2013). Therefore, the moment myelin is destroyed, the neuronal messages start to be
processed slower and even less efficiently (Alizadeh, Dyck, & Karimi-Abdolrezaee, 2015).
Both spinal cord nerves and brain stop to communicate effectively with other organs of the
body (Dendrou, Fugger, & Friese, 2015). The symptoms can affect one's balance, vision,
strength, sensation, coordination, and other critical body functions (Gass et al., 2015).
Neurological disability is commonly caused by MS in young people affecting
approximately 0.1% of the population in Northern Europe (Kingwell et al., 2013). MS affects
the majority of people within the age bracket of 20 to 40 years making the condition to be a
significant threat to social and economic development to the affected population (O’Gorman,
1 | Page
1.0 Introduction
This chapter will cover a general introduction to the research topic. The importance of
exercise and education would be explained in the context of rehabilitation. A definition of
Multiple Sclerosis will be provided and the international context of MS will be covered in
this chapter with some statistics and interventions available for people with MS. This chapter
will also provide a summary of the three key issues related to this research which are
Exercise, Rehabilitation, Education, Consultation, and Multiple Sclerosis.
1.1 Overview
Multiple Sclerosis (MS) can be defined as a chronic disorder affecting movement, the
feeling of sensation along with bodily functions (MS-UK, 2019). It is an autoimmune
inflammatory disorder that affects the central nervous system (Comi, Filippi, Wolinsky, &
Group, 2001; Matute-Blanch, Montalban, & Comabella, 2018). The vital organs that can be
affected by multiple sclerosis include myelin which helps to send and pass electrical signals
quickly between the brain and the other body organs (Podbielska, Banik, Kurowska, &
Hogan, 2013). Therefore, the moment myelin is destroyed, the neuronal messages start to be
processed slower and even less efficiently (Alizadeh, Dyck, & Karimi-Abdolrezaee, 2015).
Both spinal cord nerves and brain stop to communicate effectively with other organs of the
body (Dendrou, Fugger, & Friese, 2015). The symptoms can affect one's balance, vision,
strength, sensation, coordination, and other critical body functions (Gass et al., 2015).
Neurological disability is commonly caused by MS in young people affecting
approximately 0.1% of the population in Northern Europe (Kingwell et al., 2013). MS affects
the majority of people within the age bracket of 20 to 40 years making the condition to be a
significant threat to social and economic development to the affected population (O’Gorman,
1 | Page
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Lucas, & Taylor, 2012). The Multiple Sclerosis International Federation (2013) states that
about 60% of patients with MS will lose their motor function in about twenty years after
their diagnosis. The most common cognitive symptoms related to MS are complex attention
(Achiron & Barak, 2003), discrepancies in information processing (Macniven et al., 2008),
deficit in long-term memory (das Nair, Martin, & Lincoln, 2016; Litvan et al., 1988),
processing speed (Chiaravalloti & DeLuca, 2008; Costa, Genova, DeLuca, & Chiaravalloti,
2017).
The prevalence of MS in the UK (between 1990–2010) was estimated with about
126,669 people in 2010 (203.4 per 100 000 population) (Mackenzie, Morant, Bloomfield,
MacDonald, & O'riordan, 2014). The study reported that 6003 new cases were diagnosed in
the same year, moreover, there was an increasing population living longer with MS. The
writer also stated that this may have important implications for resource allocation for MS in
the UK (Mackenzie et al., 2014). Other studies confirm that there is continued existence of a
latitude gradient for MS in England which has a huge financial cost on the NHS in the UK
exceed £1 million per case (Ramagopalan et al., 2011).
In the Arab world and the Middle East, there is limited data and surveillance on MS
epidemiological data (Deleu et al., 2013). However, limited information is available on MS
from this part of the world. The research by Shaby (1958) reported that 0.2% of neurological
hospital admissions are patients with MS. Afterwards, the prevalence of MS in the Middle
East and North Africa is estimated with about 51.5/100,000 (Heydarpour, Khoshkish, Abtahi,
Moradi-Lakeh, & Sahraian, 2015). Several studies reported that MS prevalence is higher in
the Arab Gulf countries comparing to other Arab counties (Bohlega et al., 2013; Inshasi &
Thakre, 2011). For instance, the overall crude prevalence of MS in Qatar is 64.6/100,000
(Akhtar et al., 2013; Deleu et al., 2013), 85.0/100,000 in Kuwait (Alshubaili, Alramzy, Ayyad,
2 | Page
about 60% of patients with MS will lose their motor function in about twenty years after
their diagnosis. The most common cognitive symptoms related to MS are complex attention
(Achiron & Barak, 2003), discrepancies in information processing (Macniven et al., 2008),
deficit in long-term memory (das Nair, Martin, & Lincoln, 2016; Litvan et al., 1988),
processing speed (Chiaravalloti & DeLuca, 2008; Costa, Genova, DeLuca, & Chiaravalloti,
2017).
The prevalence of MS in the UK (between 1990–2010) was estimated with about
126,669 people in 2010 (203.4 per 100 000 population) (Mackenzie, Morant, Bloomfield,
MacDonald, & O'riordan, 2014). The study reported that 6003 new cases were diagnosed in
the same year, moreover, there was an increasing population living longer with MS. The
writer also stated that this may have important implications for resource allocation for MS in
the UK (Mackenzie et al., 2014). Other studies confirm that there is continued existence of a
latitude gradient for MS in England which has a huge financial cost on the NHS in the UK
exceed £1 million per case (Ramagopalan et al., 2011).
In the Arab world and the Middle East, there is limited data and surveillance on MS
epidemiological data (Deleu et al., 2013). However, limited information is available on MS
from this part of the world. The research by Shaby (1958) reported that 0.2% of neurological
hospital admissions are patients with MS. Afterwards, the prevalence of MS in the Middle
East and North Africa is estimated with about 51.5/100,000 (Heydarpour, Khoshkish, Abtahi,
Moradi-Lakeh, & Sahraian, 2015). Several studies reported that MS prevalence is higher in
the Arab Gulf countries comparing to other Arab counties (Bohlega et al., 2013; Inshasi &
Thakre, 2011). For instance, the overall crude prevalence of MS in Qatar is 64.6/100,000
(Akhtar et al., 2013; Deleu et al., 2013), 85.0/100,000 in Kuwait (Alshubaili, Alramzy, Ayyad,
2 | Page
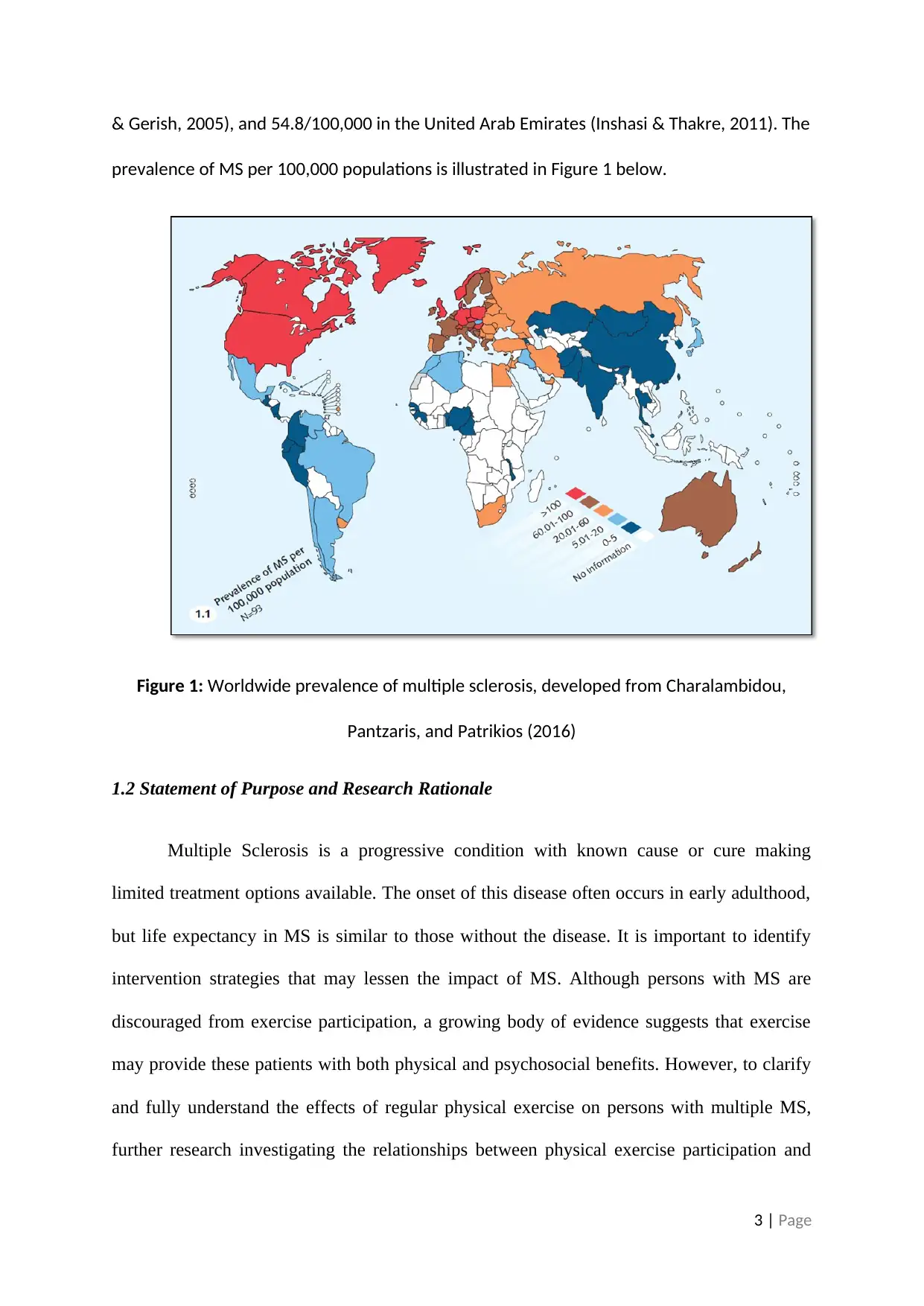
& Gerish, 2005), and 54.8/100,000 in the United Arab Emirates (Inshasi & Thakre, 2011). The
prevalence of MS per 100,000 populations is illustrated in Figure 1 below.
Figure 1: Worldwide prevalence of multiple sclerosis, developed from Charalambidou,
Pantzaris, and Patrikios (2016)
1.2 Statement of Purpose and Research Rationale
Multiple Sclerosis is a progressive condition with known cause or cure making
limited treatment options available. The onset of this disease often occurs in early adulthood,
but life expectancy in MS is similar to those without the disease. It is important to identify
intervention strategies that may lessen the impact of MS. Although persons with MS are
discouraged from exercise participation, a growing body of evidence suggests that exercise
may provide these patients with both physical and psychosocial benefits. However, to clarify
and fully understand the effects of regular physical exercise on persons with multiple MS,
further research investigating the relationships between physical exercise participation and
3 | Page
prevalence of MS per 100,000 populations is illustrated in Figure 1 below.
Figure 1: Worldwide prevalence of multiple sclerosis, developed from Charalambidou,
Pantzaris, and Patrikios (2016)
1.2 Statement of Purpose and Research Rationale
Multiple Sclerosis is a progressive condition with known cause or cure making
limited treatment options available. The onset of this disease often occurs in early adulthood,
but life expectancy in MS is similar to those without the disease. It is important to identify
intervention strategies that may lessen the impact of MS. Although persons with MS are
discouraged from exercise participation, a growing body of evidence suggests that exercise
may provide these patients with both physical and psychosocial benefits. However, to clarify
and fully understand the effects of regular physical exercise on persons with multiple MS,
further research investigating the relationships between physical exercise participation and
3 | Page
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
psychological variables is required. Results of this review can help to suggest the relationship
between exercise participation improvements in the quality of life. If physical activity is a
possible intervention or a strategy that can be used by patients with MS? The aim of this
review is to answer the research question: how do we increase exercise participation rates in
persons with MS?
1.3 Study Objectives
The broad objective of this study is to determine the impact of exercise, education,
rehabilitation and consultation on the people with multiple sclerosis.
1.4 Justification of the study
The study aims to justify the impact of exercise, education, rehabilitation and
consultation on the people with MS. The study also ought to justify barriers to exercise
engagement among people with MS. Finally, this study will focus on the effectiveness of
rehabilitation and consultative programs on the prevalence of MS (Bonavita et al., 2015).
CHAPTER TWO: BACKGROUND
2.0 Introduction
This chapter will provide a broad review of the current body of literature available on the
impact of exercise rehabilitation education and consultation on people with multiple sclerosis.
Therefore, this chapter aims to review the broad aspect of what does the literature report on
the usefulness of exercise rehabilitation education and consultation on people with multiple
sclerosis in its international context. Consequently, a gap in the literature will be identified
and the need to undertake this review will be reported. Finally, the aim of this research is to
4 | Page
between exercise participation improvements in the quality of life. If physical activity is a
possible intervention or a strategy that can be used by patients with MS? The aim of this
review is to answer the research question: how do we increase exercise participation rates in
persons with MS?
1.3 Study Objectives
The broad objective of this study is to determine the impact of exercise, education,
rehabilitation and consultation on the people with multiple sclerosis.
1.4 Justification of the study
The study aims to justify the impact of exercise, education, rehabilitation and
consultation on the people with MS. The study also ought to justify barriers to exercise
engagement among people with MS. Finally, this study will focus on the effectiveness of
rehabilitation and consultative programs on the prevalence of MS (Bonavita et al., 2015).
CHAPTER TWO: BACKGROUND
2.0 Introduction
This chapter will provide a broad review of the current body of literature available on the
impact of exercise rehabilitation education and consultation on people with multiple sclerosis.
Therefore, this chapter aims to review the broad aspect of what does the literature report on
the usefulness of exercise rehabilitation education and consultation on people with multiple
sclerosis in its international context. Consequently, a gap in the literature will be identified
and the need to undertake this review will be reported. Finally, the aim of this research is to
4 | Page
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
answer the research question: What are the impact of exercise rehabilitation education and
consultation on people with multiple sclerosis?
2.1 Exercise, Rehabilitation, Education and Consultation for people with MS
Exercise for patients with MS is essential and can enhance their quality of life, but
there are perceived barriers and benefits among MS patients (Barak, Hutzler, Dubnov-Raz, &
Achiron, 2016; Brown, Kitchen, & Nicoll, 2012). The American College of Sports Medicine
recommends that persons with MS complete three endurance-, and two resistance- exercise
training sessions per week, in addition to stretching once or twice daily (Motl et al., 2017).
According to other studies on people with MS, there is a lack of high-quality evidence as
resistance to doing exercises has benefits to these people (Khan & Amatya, 2017).
The aim of education and rehabilitative services for patients with multiple sclerosis is
to increase their level in participating in exercises and other activities as well as increasing
their independence through adequate knowledge about the benefits in participating in
activities (Döring, Pfueller, Paul, & Dörr, 2012). Different studies reported that low
socioeconomic status is related to higher risk factors are associated with MS risk (Bjørnevik
et al., 2016). Low level of education is associated with increased cases of MS (Bjørnevik et
al., 2017; Bjørnevik et al., 2016).
Rehabilitation programmes are useful in controlling existing cases of MS (Khan,
Amatya, Ytterberg, Johansson, & Kesselring, 2013; Khan, Turner‐Stokes, Ng, Kilpatrick, &
Amatya, 2007; Thompson, 1998). It has been argued that rehabilitation is more than an
‘extra’ service related to medical therapies, but an integral part of management throughout
the course the MS (Burks, Bigley, & Hill, 2009). Rehabilitation includes an interdisciplinary
team of physicians, nurses, physical therapists, occupational therapists, speech and language
pathologists, psychotherapists, social workers, recreational therapists, vocational
5 | Page
consultation on people with multiple sclerosis?
2.1 Exercise, Rehabilitation, Education and Consultation for people with MS
Exercise for patients with MS is essential and can enhance their quality of life, but
there are perceived barriers and benefits among MS patients (Barak, Hutzler, Dubnov-Raz, &
Achiron, 2016; Brown, Kitchen, & Nicoll, 2012). The American College of Sports Medicine
recommends that persons with MS complete three endurance-, and two resistance- exercise
training sessions per week, in addition to stretching once or twice daily (Motl et al., 2017).
According to other studies on people with MS, there is a lack of high-quality evidence as
resistance to doing exercises has benefits to these people (Khan & Amatya, 2017).
The aim of education and rehabilitative services for patients with multiple sclerosis is
to increase their level in participating in exercises and other activities as well as increasing
their independence through adequate knowledge about the benefits in participating in
activities (Döring, Pfueller, Paul, & Dörr, 2012). Different studies reported that low
socioeconomic status is related to higher risk factors are associated with MS risk (Bjørnevik
et al., 2016). Low level of education is associated with increased cases of MS (Bjørnevik et
al., 2017; Bjørnevik et al., 2016).
Rehabilitation programmes are useful in controlling existing cases of MS (Khan,
Amatya, Ytterberg, Johansson, & Kesselring, 2013; Khan, Turner‐Stokes, Ng, Kilpatrick, &
Amatya, 2007; Thompson, 1998). It has been argued that rehabilitation is more than an
‘extra’ service related to medical therapies, but an integral part of management throughout
the course the MS (Burks, Bigley, & Hill, 2009). Rehabilitation includes an interdisciplinary
team of physicians, nurses, physical therapists, occupational therapists, speech and language
pathologists, psychotherapists, social workers, recreational therapists, vocational
5 | Page
rehabilitation therapists, patients, families, and other caregivers (Burks et al., 2009).
A rehabilitation programme used energy conservation course to measure the impact of
this intervention on fatigue, self-efficacy, and quality of life (QOL) for patients with MS
(Mathiowetz, Matuska, & Murphy, 2001). The role of the program is to educate patients
about time management, efficient body mechanics, conservation techniques, and task
improvement independently. The study concluded that effective rehabilitation interventions
can help to reduce the impact of MS on affected persons reducing disabilities and enhance
their QOL (Mathiowetz et al., 2001). However, there is a conflicting finding from different
studies about the effectiveness of various forms of cognitive rehabilitation techniques used
with MS patients (Mitolo, Venneri, Wilkinson, & Sharrack, 2015).
Clinical consultations are effective in reducing the impacts of MS as well as the
occurrence of any correlated disease symptoms or complication (Koriem, 2016; Siegert &
Abernethy, 2005). The utilisation of effective interventions such as proactive management
can result in decreased hospital admissions and emergency presentations of people with
multiple sclerosis (Leary, Quinn, & Bowen, 2015; McLean et al., 2013).
2.2 Determinants of Physical Exercises for Patients with Multiple Sclerosis
Participation in physical exercises among healthy adults within the population is
influenced by environmental, social and personal factors. Common demographic factors that
correspond to physical activity behaviour in the general population are age and gender.
Physical activity levels are higher in men and inversely associated with age (Ebers, 2008;
Sakkas, Giannaki, Karatzaferi, & Manconi, 2019). When a review of studies assessing
interpersonal variables was conducted, self-efficacy (a person’s confidence in their ability to
participate in regular physical activity) was found to be the most commonly cited correlate of
physical activity behaviour (Platta, Ensari, Motl, & Pilutti, 2016).
6 | Page
A rehabilitation programme used energy conservation course to measure the impact of
this intervention on fatigue, self-efficacy, and quality of life (QOL) for patients with MS
(Mathiowetz, Matuska, & Murphy, 2001). The role of the program is to educate patients
about time management, efficient body mechanics, conservation techniques, and task
improvement independently. The study concluded that effective rehabilitation interventions
can help to reduce the impact of MS on affected persons reducing disabilities and enhance
their QOL (Mathiowetz et al., 2001). However, there is a conflicting finding from different
studies about the effectiveness of various forms of cognitive rehabilitation techniques used
with MS patients (Mitolo, Venneri, Wilkinson, & Sharrack, 2015).
Clinical consultations are effective in reducing the impacts of MS as well as the
occurrence of any correlated disease symptoms or complication (Koriem, 2016; Siegert &
Abernethy, 2005). The utilisation of effective interventions such as proactive management
can result in decreased hospital admissions and emergency presentations of people with
multiple sclerosis (Leary, Quinn, & Bowen, 2015; McLean et al., 2013).
2.2 Determinants of Physical Exercises for Patients with Multiple Sclerosis
Participation in physical exercises among healthy adults within the population is
influenced by environmental, social and personal factors. Common demographic factors that
correspond to physical activity behaviour in the general population are age and gender.
Physical activity levels are higher in men and inversely associated with age (Ebers, 2008;
Sakkas, Giannaki, Karatzaferi, & Manconi, 2019). When a review of studies assessing
interpersonal variables was conducted, self-efficacy (a person’s confidence in their ability to
participate in regular physical activity) was found to be the most commonly cited correlate of
physical activity behaviour (Platta, Ensari, Motl, & Pilutti, 2016).
6 | Page
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Additionally, barriers or challenges of effectively engaging in physical activity
include; exercise partners, lack of facilities, bad weather, fear of falling, too weak, too tiring
and lack of time. Social support also appears to influence physical activity behaviour
strongly. Every study reviewed showed measures of social support in their analysis and found
an important positive association between social support and physical activity levels. Finally,
several environmental factors are known to influence physical activity behaviour in the
general population. These environmental factors include; satisfaction with recreational
facilities, access to facilities, equipment at home, and community levels influences such as
hilly terrain, neighbourhood safety, enjoyable scenery and observation of others exercising.
Although determinants of physical activity have been well established in the general
population; few studies have investigated the determinants of physical exercise engagement
by patients with multiple sclerosis. It is unknown whether the determinants of physical
activity behaviour will be the same in persons with MS. It could be speculated that due to the
nature of MS, disease-specific factors may influence physical activity behaviours, and
barriers to physical activity practices that may differ from those observed in the general
population (Prosperini, Piattella, Giannì, & Pantano, 2015).
For persons with MS to safely participate in the exercise, special considerations
should be made when prescribing exercise. Firstly, one should be aware that symptom
exacerbations may occur during or following periods of physical activity. Symptom
exacerbations refer to the onset or increase in the intensity of symptoms. For example,
persons with MS may develop foot drop or become progressively unsteady while
participating in, or following physical activity. Symptom exacerbations are one of the
primary reasons why persons with MS were initially discouraged from exercise participation
(Ransohoff, Hafler, & Lucchinetti, 2015).
7 | Page
include; exercise partners, lack of facilities, bad weather, fear of falling, too weak, too tiring
and lack of time. Social support also appears to influence physical activity behaviour
strongly. Every study reviewed showed measures of social support in their analysis and found
an important positive association between social support and physical activity levels. Finally,
several environmental factors are known to influence physical activity behaviour in the
general population. These environmental factors include; satisfaction with recreational
facilities, access to facilities, equipment at home, and community levels influences such as
hilly terrain, neighbourhood safety, enjoyable scenery and observation of others exercising.
Although determinants of physical activity have been well established in the general
population; few studies have investigated the determinants of physical exercise engagement
by patients with multiple sclerosis. It is unknown whether the determinants of physical
activity behaviour will be the same in persons with MS. It could be speculated that due to the
nature of MS, disease-specific factors may influence physical activity behaviours, and
barriers to physical activity practices that may differ from those observed in the general
population (Prosperini, Piattella, Giannì, & Pantano, 2015).
For persons with MS to safely participate in the exercise, special considerations
should be made when prescribing exercise. Firstly, one should be aware that symptom
exacerbations may occur during or following periods of physical activity. Symptom
exacerbations refer to the onset or increase in the intensity of symptoms. For example,
persons with MS may develop foot drop or become progressively unsteady while
participating in, or following physical activity. Symptom exacerbations are one of the
primary reasons why persons with MS were initially discouraged from exercise participation
(Ransohoff, Hafler, & Lucchinetti, 2015).
7 | Page
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Figure 2: The Importance of Physical exercise for people with MS in Middle East
2.3 Impact of rehabilitation on people with Multiple Sclerosis
According to a study that was conducted in Saudi Arabia to assess the impact of
multidisciplinary rehabilitation on people with multiple sclerosis among 24 patients; the
findings indicated 48% of cases linked to lack of rehabilitation. Rehabilitation intervention
was found to improve independence among patients with chronic MS. Multiple sclerosis
(MS) causes neurologic disability mostly in young adults. Studies show that in relapsing-
remitting form (RR-MS), the cause of MS is characterised by relapses which represent in
58% to 66% of patients. These relapses cause impairment within ten years of onset, affecting
one-half of the patients through the progressive form. The patient can either be on neither
progressive course nor spontaneous remission. Although the majority of patients may have
extended periods of stability, MS can also begin with a continuous form affecting
8 | Page
2.3 Impact of rehabilitation on people with Multiple Sclerosis
According to a study that was conducted in Saudi Arabia to assess the impact of
multidisciplinary rehabilitation on people with multiple sclerosis among 24 patients; the
findings indicated 48% of cases linked to lack of rehabilitation. Rehabilitation intervention
was found to improve independence among patients with chronic MS. Multiple sclerosis
(MS) causes neurologic disability mostly in young adults. Studies show that in relapsing-
remitting form (RR-MS), the cause of MS is characterised by relapses which represent in
58% to 66% of patients. These relapses cause impairment within ten years of onset, affecting
one-half of the patients through the progressive form. The patient can either be on neither
progressive course nor spontaneous remission. Although the majority of patients may have
extended periods of stability, MS can also begin with a continuous form affecting
8 | Page
approximately 18% to 34% of patients. Mostly, eight years after the onset of a progressive
way, the patient is likely to experience limitations to movement or walking resulting in
needing for support by 20 years and diagnosis at 30 years (Pearson, Dieberg, & Smart, 2015).
This patient will be able to walk a few steps after a successful diagnosis. Functional processes
and systems such as the cerebellum, the visual system, cognition, the brainstem, bladder,
sexual function, sensory system, bowel, and cerebral become affected progressively causing
disability in affected people. These facts justify rehabilitation in MS as a process that focuses
on helping patients to successfully maintain and reach their potential physical, social,
psychological, and vocational abilities helping them to achieve acceptable quality of life
(Hauser et al., 2017).
Study conducted in Saudi Arabia on clinical trials found that rehabilitation programs
help to improve the patient's condition and quality of life between the relapse stage in terms
of strength, reduction in motor fatigue, and physical condition. According to the study
findings, rehabilitation and intensive physiotherapy programs are useful when treating
relapses in patients (Thompson et al., 2018). Study findings on clinical trials found the
effectiveness of rehabilitation programs for people with MS and proved that the programs are
useful especially when they are combined with ant spasticity medication as well as
complemented by videos. The purpose of occupational therapy is to support optimise
functional capacity from the affected person. The goal of this therapy is to allow patients to
participate in recreation activities as needed. Patients sent to occupational therapy with
symptoms such as upper limb impairment and fatigue have limitations in their development
of daily and social events (Kerling et al., 2015). The role of occupational health is to educate
patients about time management, efficient body mechanics, conservation techniques, and task
improvement independently. Analysis of results shows that many clinical trials containing
high methodologic evidence and quality, suggests that the use of educational courses on
9 | Page
way, the patient is likely to experience limitations to movement or walking resulting in
needing for support by 20 years and diagnosis at 30 years (Pearson, Dieberg, & Smart, 2015).
This patient will be able to walk a few steps after a successful diagnosis. Functional processes
and systems such as the cerebellum, the visual system, cognition, the brainstem, bladder,
sexual function, sensory system, bowel, and cerebral become affected progressively causing
disability in affected people. These facts justify rehabilitation in MS as a process that focuses
on helping patients to successfully maintain and reach their potential physical, social,
psychological, and vocational abilities helping them to achieve acceptable quality of life
(Hauser et al., 2017).
Study conducted in Saudi Arabia on clinical trials found that rehabilitation programs
help to improve the patient's condition and quality of life between the relapse stage in terms
of strength, reduction in motor fatigue, and physical condition. According to the study
findings, rehabilitation and intensive physiotherapy programs are useful when treating
relapses in patients (Thompson et al., 2018). Study findings on clinical trials found the
effectiveness of rehabilitation programs for people with MS and proved that the programs are
useful especially when they are combined with ant spasticity medication as well as
complemented by videos. The purpose of occupational therapy is to support optimise
functional capacity from the affected person. The goal of this therapy is to allow patients to
participate in recreation activities as needed. Patients sent to occupational therapy with
symptoms such as upper limb impairment and fatigue have limitations in their development
of daily and social events (Kerling et al., 2015). The role of occupational health is to educate
patients about time management, efficient body mechanics, conservation techniques, and task
improvement independently. Analysis of results shows that many clinical trials containing
high methodologic evidence and quality, suggests that the use of educational courses on
9 | Page
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
energy conservation portrayed positive impact on fatigue as well as other aspects of quality of
life. On the other hand, measurements related to occupational therapy in patients affected
with MS showed a moderate improvement in the coordination of the exercise program as well
as upper limbs. However, new studies should be conducted to prove the efficacy within the
aspects of occupational therapy among patients with MS (Wattjes et al., 2015).
2.4 Impact of Education to people with multiple sclerosis
Recent reports from middle East identied a substantial burden of multiple sclerosis within the
Middle East countries. Data on the epidemiology, clinical presentation, risk factors, and
management of multiple sclerosis within middle East countries showed different impacts of
multiple sclerosis on education. Studies conducted by scientists to find out education level
with MS revealed that low education level was associated to a low-income level while high
education level associated to a high-income level. According to findings of the study, people
with high education level were less affected by multiple sclerosis since they were
knowledgeable on how to avoid the disease. In this study, the majority of people affected
with MS were associated with low education level. This is because they did not have
appropriate knowledge and information on how to avoid the disease hence contracting the
disease easily (Chen et al., 2016). Today, nearly half of the patients diagnosed with MS either
never worked or they were housewives representing an increased percentage of those who
were employed as well as educated. Another study showed that 33% of women who were
doing housework jobs had previously been used outside their home. Education level and
social customs may also have a different impact on the prevalence of MS causing a difference
in the demographic presentation of the condition (Hatcher, Waubant, Nourbakhsh, Crabtree-
Hartman, & Graves, 2016).
According to another study that was conducted in state of Qatar to assess prevalence
of multiple sclerosis among young university students; prevalence of the disease was at 2%.
10 | Page
life. On the other hand, measurements related to occupational therapy in patients affected
with MS showed a moderate improvement in the coordination of the exercise program as well
as upper limbs. However, new studies should be conducted to prove the efficacy within the
aspects of occupational therapy among patients with MS (Wattjes et al., 2015).
2.4 Impact of Education to people with multiple sclerosis
Recent reports from middle East identied a substantial burden of multiple sclerosis within the
Middle East countries. Data on the epidemiology, clinical presentation, risk factors, and
management of multiple sclerosis within middle East countries showed different impacts of
multiple sclerosis on education. Studies conducted by scientists to find out education level
with MS revealed that low education level was associated to a low-income level while high
education level associated to a high-income level. According to findings of the study, people
with high education level were less affected by multiple sclerosis since they were
knowledgeable on how to avoid the disease. In this study, the majority of people affected
with MS were associated with low education level. This is because they did not have
appropriate knowledge and information on how to avoid the disease hence contracting the
disease easily (Chen et al., 2016). Today, nearly half of the patients diagnosed with MS either
never worked or they were housewives representing an increased percentage of those who
were employed as well as educated. Another study showed that 33% of women who were
doing housework jobs had previously been used outside their home. Education level and
social customs may also have a different impact on the prevalence of MS causing a difference
in the demographic presentation of the condition (Hatcher, Waubant, Nourbakhsh, Crabtree-
Hartman, & Graves, 2016).
According to another study that was conducted in state of Qatar to assess prevalence
of multiple sclerosis among young university students; prevalence of the disease was at 2%.
10 | Page
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Similar statistics were revealed to show a comparison between the disease and education, but
more severe cases of MS reported increased destructive effect among people with a low-
income level as well as low education level (Kalron, Fonkatz, Frid, Baransi, & Achiron,
2016). Similarly, another study revealed an extended duration of disease affected individual
ability to progress in education. In the study, the majority of respondents had acquired their
high school education but the level of education did not have an adverse effect on the
duration of the diseases since the majority of patients affected with the disease were in their
30s. The study only found that 6.1% of the respondents affected with MS had their education
affected too, but the majority were not affected (Campbell et al., 2016).
2.5 Impact of Consultation to people with multiple sclerosis
According to a study that was conducted in the Qatar on the impact of consultation to
people with MS has resulted in low number of cases of people affected with the infection.
According to the study, out of 100 predicted people that were examined, only eleven were
found positive on MS case. Nurses providing consultation services helped to manage existing
cases as well as providing necessary measures to prevent the occurrence of new cases. Rapid
response to emergency cases of MS helped to minimise the effects of the disease such as
disability in younger adults. Other countries such as middle East have also shown significant
low number of cases of MS due to increased consultation services. According to this study,
proactive management demonstrated a useful intervention to decrease hospital admissions
and emergency presentations which consequently reduced the number of cases reported
(Palace et al., 2015).
11 | Page
more severe cases of MS reported increased destructive effect among people with a low-
income level as well as low education level (Kalron, Fonkatz, Frid, Baransi, & Achiron,
2016). Similarly, another study revealed an extended duration of disease affected individual
ability to progress in education. In the study, the majority of respondents had acquired their
high school education but the level of education did not have an adverse effect on the
duration of the diseases since the majority of patients affected with the disease were in their
30s. The study only found that 6.1% of the respondents affected with MS had their education
affected too, but the majority were not affected (Campbell et al., 2016).
2.5 Impact of Consultation to people with multiple sclerosis
According to a study that was conducted in the Qatar on the impact of consultation to
people with MS has resulted in low number of cases of people affected with the infection.
According to the study, out of 100 predicted people that were examined, only eleven were
found positive on MS case. Nurses providing consultation services helped to manage existing
cases as well as providing necessary measures to prevent the occurrence of new cases. Rapid
response to emergency cases of MS helped to minimise the effects of the disease such as
disability in younger adults. Other countries such as middle East have also shown significant
low number of cases of MS due to increased consultation services. According to this study,
proactive management demonstrated a useful intervention to decrease hospital admissions
and emergency presentations which consequently reduced the number of cases reported
(Palace et al., 2015).
11 | Page
Chapter Three: Methodology & Method (2500 words)
This chapter will present the literature review as a chosen research methodology. The method
used to collect, access, analyse, and present information extracted from secondary sources.
12 | Page
This chapter will present the literature review as a chosen research methodology. The method
used to collect, access, analyse, and present information extracted from secondary sources.
12 | Page
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 20
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.