PBH91001 - Critical Appraisal of Music Therapy for Sleep Quality
VerifiedAdded on 2023/06/03
|8
|6795
|254
Report
AI Summary
This report critically appraises the effectiveness of music therapy in improving sleep quality among older adults. It examines a randomized controlled study investigating the effects of sedative music on sleep quality in a cohort of older community-dwelling adults in Singapore, measuring sleep quality using the Pittsburgh Sleep Quality Index (PSQI). The intervention involved participants listening to soft, instrumental music for 6 weeks, with results showing significant improvements in sleep quality compared to a control group. The appraisal considers the study's methodology, findings, and implications for healthcare, emphasizing the potential of music listening as a non-pharmacological intervention to enhance sleep quality and promote healthy aging. This assignment also includes the critical appraisal of a systematic review (secondary evidence) related to this topic. Desklib provides access to a wealth of similar assignments and past papers for students seeking to deepen their understanding of healthcare research and evidence-based practice.

ComplementaryTherapiesin Medicine(2014)22, 49—56
Available online at www.sciencedirect.com
ScienceDirect
j ou rn a l home p a ge : w w w . e l s e v i e r h e a l t h . c o m / j o u r n a l s / c t i m
Theeffectsof sedativemusicon sleep
qualityof oldercommunity-dwellingadults
in Singapore
AngelaShuma, BeverleyJoan Taylorb, Jeff Thayalac,
MoonFaiChana,∗
a Alice Lee Centre for NursingStudies,YongLoo Lin Schoolof Medicine,NationalUniversityof Singapore,
Singapore
b Faculty of Medicine,Nursingand Health Sciences,Schoolof Nursingand Midwifery,MonashUniversity,
GippslandCampus,Churchill, Victoria, Australia
c Departmentof NursingAdministrations,Institute of Mental Health, Singapore
Availableonline 14 November2013
KEYWORDS
Musiclistening;
Olderadults;
Sleepquality
Summary
Objectives:Toexaminethe effectsof musiclisteningon sleepqualityamongstoldercommunity-
dwellingadultsin Singapore.
Methods:In a randomizedcontrolledstudy,a cohortof olderadults(N =60)age55yearsor above
were recruited in one communitycentre. Sleep quality, as measuredby the PittsburghSleep
QualityIndex(PSQI), was the primaryoutcome.Participants’demographicvariablesincluding
age,gender,religion,educationlevel, maritalandfinancialstatus,anychronicillness,previous
experiencesof musicinterventionas well asdepressionlevelswerecollected.Participantswere
askedto listen to soft, instrumentalslowsedativemusicwithoutlyrics, of approximately60—80
beatsper minute, and 40min in duration,for 6 weeks.Generalizedestimatingequationswere
usedto examinethe effects of the interventionon the elders’ sleepquality.
Results:Significantreductionsin PSQIscoreswere foundin the interventiongroup(n =28)from
baseline(mean± SD, 10.2± 2.5) to week 6 (5.9± 2.4, p <0.001),while there were no changes
in the control group (n =32) from baseline(9.0± 2.4) to week 6 (9.5± 2.6). At week 6, the
interventiongroupshoweda better sleepquality than the control ( 2 =61.84,p <0.001).
Conclusions:Notwithstandingthe placeboeffect, this studysupportsmusiclisteningasan effec-
tive interventionfor older adultsto improvesleep quality.Not only doesthis processimprove
their sleepingquality at old age, it also individualizesand enhancesthe quality of care pro-
vided by the healthcareprovideras the therapeuticrelationshipbetweenproviderand client
is beingestablished.Contemporarygerontologyis progressivelycharacterizedby collaboration
betweenseveralapproacheswith the intent to comprehendthe mentalaspectsof the multi-
fariousprocessof ageing.Musiclisteningis one suchavenueto enhancesleepquality amongst
older adultsand makean essentialcontributionto healthyageing.
©2013ElsevierLtd. All rightsreserved.
∗ Correspondingauthor.Tel.: +6565168684.
E-mail address:nurcmf@nus.edu.sg(M.F.Chan).
0965-2299/$— see front matter©2013ElsevierLtd. All rightsreserved.
http://dx.doi.org/10.1016/j.ctim.2013.11.003
Available online at www.sciencedirect.com
ScienceDirect
j ou rn a l home p a ge : w w w . e l s e v i e r h e a l t h . c o m / j o u r n a l s / c t i m
Theeffectsof sedativemusicon sleep
qualityof oldercommunity-dwellingadults
in Singapore
AngelaShuma, BeverleyJoan Taylorb, Jeff Thayalac,
MoonFaiChana,∗
a Alice Lee Centre for NursingStudies,YongLoo Lin Schoolof Medicine,NationalUniversityof Singapore,
Singapore
b Faculty of Medicine,Nursingand Health Sciences,Schoolof Nursingand Midwifery,MonashUniversity,
GippslandCampus,Churchill, Victoria, Australia
c Departmentof NursingAdministrations,Institute of Mental Health, Singapore
Availableonline 14 November2013
KEYWORDS
Musiclistening;
Olderadults;
Sleepquality
Summary
Objectives:Toexaminethe effectsof musiclisteningon sleepqualityamongstoldercommunity-
dwellingadultsin Singapore.
Methods:In a randomizedcontrolledstudy,a cohortof olderadults(N =60)age55yearsor above
were recruited in one communitycentre. Sleep quality, as measuredby the PittsburghSleep
QualityIndex(PSQI), was the primaryoutcome.Participants’demographicvariablesincluding
age,gender,religion,educationlevel, maritalandfinancialstatus,anychronicillness,previous
experiencesof musicinterventionas well asdepressionlevelswerecollected.Participantswere
askedto listen to soft, instrumentalslowsedativemusicwithoutlyrics, of approximately60—80
beatsper minute, and 40min in duration,for 6 weeks.Generalizedestimatingequationswere
usedto examinethe effects of the interventionon the elders’ sleepquality.
Results:Significantreductionsin PSQIscoreswere foundin the interventiongroup(n =28)from
baseline(mean± SD, 10.2± 2.5) to week 6 (5.9± 2.4, p <0.001),while there were no changes
in the control group (n =32) from baseline(9.0± 2.4) to week 6 (9.5± 2.6). At week 6, the
interventiongroupshoweda better sleepquality than the control ( 2 =61.84,p <0.001).
Conclusions:Notwithstandingthe placeboeffect, this studysupportsmusiclisteningasan effec-
tive interventionfor older adultsto improvesleep quality.Not only doesthis processimprove
their sleepingquality at old age, it also individualizesand enhancesthe quality of care pro-
vided by the healthcareprovideras the therapeuticrelationshipbetweenproviderand client
is beingestablished.Contemporarygerontologyis progressivelycharacterizedby collaboration
betweenseveralapproacheswith the intent to comprehendthe mentalaspectsof the multi-
fariousprocessof ageing.Musiclisteningis one suchavenueto enhancesleepquality amongst
older adultsand makean essentialcontributionto healthyageing.
©2013ElsevierLtd. All rightsreserved.
∗ Correspondingauthor.Tel.: +6565168684.
E-mail address:nurcmf@nus.edu.sg(M.F.Chan).
0965-2299/$— see front matter©2013ElsevierLtd. All rightsreserved.
http://dx.doi.org/10.1016/j.ctim.2013.11.003
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

50 A. Shumet al.
Introduction
Sleep disturbanceshave been recognizedas a significant
and growingcausefor public healthconcern.1 Eventhough
it is known to affect all age groups, prior researchhas
suggestedthat older adults are of greater vulnerability
to sleep problems.2 Previousepidemiologicalstudieshave
indicated that sleep complaintslike sleep fragmentation
and daytimesleepinessaffected approximately35%of the
generalpopulation,3 and up to 50%of the older adults.4
Sleepdisturbancescontributeto insufficientor ineffective
sleep patterns, which are known to heightenthe risk for
adverseconsequenceslike cognitiveimpairment,falls, and
deteriorationin physicalfunctioning.1,5,6 Currently,pharma-
cotherapyis the main form of remedyto alleviate sleep
disturbancesand improvesleep quality.8 However,these
medicationsare associatedwith psychologicaland physi-
ological side effects that can affect daily activities and
functioningof individuals.The use of thesedrugscan also
leadto toleranceanddependence.9 Aspriorresearchhasyet
to establishthe safetyandefficacyof thesepharmacological
measures,10 sleep scientistshave recommendedexploring
non-pharmacologicaltechniqueswith a mind-bodyinterac-
tion to promotesleep.11 A range of non-pharmacological
interventionsare availableas alternativetreatmentsfor
sleep disturbances.They include cognitive behavioural
treatments,12 bright light therapy,13 and neurofeedback.7
However,the feasibilityof theseinterventionsis question-
able, as they often require large investmentsof time for
training purposes.14 As such, music interventionis iden-
tified by the researchersas an area of interest as it is
relativelyinexpensive,readily availableand can be easily
self-administered.15
A meta-analysisof fiverandomizedcontrolledtrials(RCT)
conductedwith relevanceto thistopicreporteda significant
effect of musiclisteningon sleepqualityfor all agegroupsin
general.14 Generalizedfindingson the effectivenessof music
listeningon sleepqualityare shownto be optimistic.How-
ever,thesefindingsmustbe interpretedwith caution,as all
of thesestudieswereconductedin differentpopulationsand
settings.14 In referenceto the elderlypopulation,the effects
of musicon their sleepqualityremainsuncertaindueto the
limitedstudiesconducted.Despiteits potentialbenefits,no
systematicreviewhasbeenconductedto evaluatethe effec-
tivenessof musicon sleepqualityfor older populations.To
date, only five related studies,16—20were found, of which
only one was a RCT studywith a sole focuson musiclisten-
ingfor olderadults.16 Otherstudiesconductedto investigate
the effectivenessof musiclisteningon sleep quality were
focuson older females,17 femalestudents,19,21andpatients
with insomnia,22 but all studiesclearlyindicatedcontinuous
improvementin sleep acrossthe time spanof the applied
intervention.16—18,20,21,23—25
The interventionperiodof these
studiesrangedfrom 10 days17 up to 45 days.23
Aim
The aimof this studywasto investigatethe effectsof music
listeningonsleepqualityamongstoldercommunity-dwelling
adultsin Singapore.The hypothesisfor this studywas that
older adultswho participatein a musicinterventiongroup
will report better sleepqualityscores,as measuredby the
PittsburghSleep Quality Index (PSQI), 6 weeks after the
intervention,comparedwith non-music(control)group.
Methods
Designandparticipants
This researchwas a RCT conductedat the participants’
homes from January 2012 to January 2013. A cohort of
community-dwellingolder adultswasrecruitedin one com-
munitycentrein Singapore.Inclusioncriteria were (1) aged
55 years or older,30 (2) living within the selectedarea of
northernpart of Singapore,(3) non-institutionalizeddur-
ing the studyperiod, (4) physicallycapableof completing
psychologicalassessment,(5) able to understandand com-
municatein either Englishor Mandarinand give written
consent,and(6) havea poorsleepquality,measuredby the
PSQI, with a scoreof 6 or above.26 Exclusioncriteria were
(1) a medicaldiagnosisof anyabnormalcognitivefunction,
such as Parkinson’sdiseaseor dementia,and (2) hearing
difficulties.
The required sample size was based on an expected
effect size of sleepqualitylevelspost-intervention.de Niet
et al.14 conducteda meta-analysisand results suggested
that music interventionhas a moderateeffect on sleep
quality in five RCT studies.In relation to effect size, the
nQueryAdvisorsoftware27 showsthatat least30participants
with completedata per groupwould be neededto detect
an effect with 80%powerand 5%significance.Approvalto
conductthe current study was soughtand obtainedfrom
the InstitutionalReviewBoard ethics committee.Written
informedconsentwasobtainedfromeachparticipantbefore
obtainingtheir baselinePQSIscores.
Themeasurements
The instrumentwas presentedin both Englishand Chinese
and consistedof two parts.Part one collectedparticipants’
demographicvariablesincludingage, gender,religion,edu-
cation level, maritaland financialstatus,and any previous
experienceof music interventions,any chronic illness as
well as depressivesymptoms,as measuredby the Geriatric
DepressionScale(GDS-15).28 Parttwo collecteddataon par-
ticipants’sleepquality,asmeasuredby the PQSI.ThePQSIis
a self-ratedquestionnairewhichassessessleepqualityand
disturbancesovera periodof time. The PSQIwaschosento
measurethe qualityof sleepin older adultsbecauseit has
a goodoverallreliabilitycoefficient(˛ =0.83).35 It hasbeen
usedin previousstudiesinvestigatingthe effects of music
on the quality of sleep.36,37 It is dividedinto severalcom-
ponentsthat assesssubjectivesleepquality,sleeplatency,
sleepduration,sleepefficiency,sleepdisturbances,use of
sleepingmedication,and daytimedysfunction.The sumof
scoresrangesfrom 0 to 21, and a scoreof 6 or aboveindi-
catesa poorsleepquality.26 All participantshadthe options
to chooseeither Englishor Chineseinstruments.For par-
ticipantsin the interventiongroup,data were collectedat
baselinebeforethe musicinterventionat week1, andafter
the musicinterventionin weeks2—6,oncea weekfor a total
of six times, includingthe baseline.For participantsin the
Introduction
Sleep disturbanceshave been recognizedas a significant
and growingcausefor public healthconcern.1 Eventhough
it is known to affect all age groups, prior researchhas
suggestedthat older adults are of greater vulnerability
to sleep problems.2 Previousepidemiologicalstudieshave
indicated that sleep complaintslike sleep fragmentation
and daytimesleepinessaffected approximately35%of the
generalpopulation,3 and up to 50%of the older adults.4
Sleepdisturbancescontributeto insufficientor ineffective
sleep patterns, which are known to heightenthe risk for
adverseconsequenceslike cognitiveimpairment,falls, and
deteriorationin physicalfunctioning.1,5,6 Currently,pharma-
cotherapyis the main form of remedyto alleviate sleep
disturbancesand improvesleep quality.8 However,these
medicationsare associatedwith psychologicaland physi-
ological side effects that can affect daily activities and
functioningof individuals.The use of thesedrugscan also
leadto toleranceanddependence.9 Aspriorresearchhasyet
to establishthe safetyandefficacyof thesepharmacological
measures,10 sleep scientistshave recommendedexploring
non-pharmacologicaltechniqueswith a mind-bodyinterac-
tion to promotesleep.11 A range of non-pharmacological
interventionsare availableas alternativetreatmentsfor
sleep disturbances.They include cognitive behavioural
treatments,12 bright light therapy,13 and neurofeedback.7
However,the feasibilityof theseinterventionsis question-
able, as they often require large investmentsof time for
training purposes.14 As such, music interventionis iden-
tified by the researchersas an area of interest as it is
relativelyinexpensive,readily availableand can be easily
self-administered.15
A meta-analysisof fiverandomizedcontrolledtrials(RCT)
conductedwith relevanceto thistopicreporteda significant
effect of musiclisteningon sleepqualityfor all agegroupsin
general.14 Generalizedfindingson the effectivenessof music
listeningon sleepqualityare shownto be optimistic.How-
ever,thesefindingsmustbe interpretedwith caution,as all
of thesestudieswereconductedin differentpopulationsand
settings.14 In referenceto the elderlypopulation,the effects
of musicon their sleepqualityremainsuncertaindueto the
limitedstudiesconducted.Despiteits potentialbenefits,no
systematicreviewhasbeenconductedto evaluatethe effec-
tivenessof musicon sleepqualityfor older populations.To
date, only five related studies,16—20were found, of which
only one was a RCT studywith a sole focuson musiclisten-
ingfor olderadults.16 Otherstudiesconductedto investigate
the effectivenessof musiclisteningon sleep quality were
focuson older females,17 femalestudents,19,21andpatients
with insomnia,22 but all studiesclearlyindicatedcontinuous
improvementin sleep acrossthe time spanof the applied
intervention.16—18,20,21,23—25
The interventionperiodof these
studiesrangedfrom 10 days17 up to 45 days.23
Aim
The aimof this studywasto investigatethe effectsof music
listeningonsleepqualityamongstoldercommunity-dwelling
adultsin Singapore.The hypothesisfor this studywas that
older adultswho participatein a musicinterventiongroup
will report better sleepqualityscores,as measuredby the
PittsburghSleep Quality Index (PSQI), 6 weeks after the
intervention,comparedwith non-music(control)group.
Methods
Designandparticipants
This researchwas a RCT conductedat the participants’
homes from January 2012 to January 2013. A cohort of
community-dwellingolder adultswasrecruitedin one com-
munitycentrein Singapore.Inclusioncriteria were (1) aged
55 years or older,30 (2) living within the selectedarea of
northernpart of Singapore,(3) non-institutionalizeddur-
ing the studyperiod, (4) physicallycapableof completing
psychologicalassessment,(5) able to understandand com-
municatein either Englishor Mandarinand give written
consent,and(6) havea poorsleepquality,measuredby the
PSQI, with a scoreof 6 or above.26 Exclusioncriteria were
(1) a medicaldiagnosisof anyabnormalcognitivefunction,
such as Parkinson’sdiseaseor dementia,and (2) hearing
difficulties.
The required sample size was based on an expected
effect size of sleepqualitylevelspost-intervention.de Niet
et al.14 conducteda meta-analysisand results suggested
that music interventionhas a moderateeffect on sleep
quality in five RCT studies.In relation to effect size, the
nQueryAdvisorsoftware27 showsthatat least30participants
with completedata per groupwould be neededto detect
an effect with 80%powerand 5%significance.Approvalto
conductthe current study was soughtand obtainedfrom
the InstitutionalReviewBoard ethics committee.Written
informedconsentwasobtainedfromeachparticipantbefore
obtainingtheir baselinePQSIscores.
Themeasurements
The instrumentwas presentedin both Englishand Chinese
and consistedof two parts.Part one collectedparticipants’
demographicvariablesincludingage, gender,religion,edu-
cation level, maritaland financialstatus,and any previous
experienceof music interventions,any chronic illness as
well as depressivesymptoms,as measuredby the Geriatric
DepressionScale(GDS-15).28 Parttwo collecteddataon par-
ticipants’sleepquality,asmeasuredby the PQSI.ThePQSIis
a self-ratedquestionnairewhichassessessleepqualityand
disturbancesovera periodof time. The PSQIwaschosento
measurethe qualityof sleepin older adultsbecauseit has
a goodoverallreliabilitycoefficient(˛ =0.83).35 It hasbeen
usedin previousstudiesinvestigatingthe effects of music
on the quality of sleep.36,37 It is dividedinto severalcom-
ponentsthat assesssubjectivesleepquality,sleeplatency,
sleepduration,sleepefficiency,sleepdisturbances,use of
sleepingmedication,and daytimedysfunction.The sumof
scoresrangesfrom 0 to 21, and a scoreof 6 or aboveindi-
catesa poorsleepquality.26 All participantshadthe options
to chooseeither Englishor Chineseinstruments.For par-
ticipantsin the interventiongroup,data were collectedat
baselinebeforethe musicinterventionat week1, andafter
the musicinterventionin weeks2—6,oncea weekfor a total
of six times, includingthe baseline.For participantsin the

The effect of sedativemusicon sleepquality 51
controlgroup,datawerecollectedoncea weekfor the same
6 weeks as the interventiongroup, when the researcher
visitedthemat home.
Themusicintervention
The processof musicinterventiontook place in each par-
ticipant’shome.After the randomallocationof participants
to groups,weeklyvisitswere madefor 6 weeksto measure
the sameoutcomes.Six weeksis a recommendedperiodof
time for observingsleep patterns,16,23 and the effects of
a new interventionon sleep quality.14 Participantsin the
experimentalgroupwere providedwith an MP4playerwith
earphonesin order to listen to the music of their choice
from a selection of soft, slow music without lyrics (for
details,pleaseseethe sectionon Selectionof music).Previ-
ous literaturehas shownsubjectiveand scientificevidence
in demonstratingthat music preferenceis a key element
in derivingbeneficialbenefitsfrom music.16,18,36Therefore,
participantswere allowedto choosetheir preferredmusic
and they were requiredto adhereto the use of a single
genreof musicwithin the sameweek, to minimizepossi-
ble variancesin the effect on sleep quality. Participants
were also told to choosethe most comfortableplace to
listen to the music, for examplein their bedroom.Stan-
dardizedinstructionswere givento the participantsas per
a protocol proposedby Chan et al.16 The researcherleft
the participantsalone and stayed a short distanceaway
unobtrusively,so that she or he could be availablefor any
unexpectedresponse.After 40min, the researcherstopped
the music and then collected all outcomesfor each par-
ticipant within a 10—15min conversation.Previousstudies
havesuggestedthat listeningto musiceverydaycontributes
to a better sleep at night, even if it is not consistently
heardat bedtime.16,18,24,36,39
However,to ensureconsistency
in the times for listeningto music, the researchermade
one follow-up phonecall per week after the interviewto
remindparticipantsto listen to the musiconce a day. All
the data collection, includingadministeringthe interven-
tion and collectingthe data, was carried out by the same
researcher.
Thecontrolgroup
Participantsin the controlgroupmet the researcherfor the
samenumberof times as those in the interventiongroup.
Participantsin the control group were given an uninter-
ruptedrest period, but the samedata were collectedonce
a week for 6 weeks.The researchermet them only to col-
lect their sleep quality scores. The researcherrequested
participants,duringthe studyperiod,to not listen to seda-
tive music, but we could not restrict them from listening
to radio or TV. Duringdata collection,the researchermin-
imizedinteractionwith this groupof participants,so as to
reduceresultcontaminationandhenceincreasethe reliabil-
ity of the results.All the data collectionwascarriedout by
the sameresearcher.Everyweek,the researchervisitedthe
participantsandaskedthemwhethertheytookanymedica-
tions to changetheir sleeppatternsand noneof them had
takenanymedications.
Randomization
Two cards were put inside a bag in each draw, with one
labelled as ‘‘intervention’’ and the other as ‘‘control’’.
Each participantwas askedto draw one card from the bag
to allocatehim or her into either the interventionor con-
trol group. There was no blindingas the participantsand
interviewerknewthe allocationgroupsafter randomization.
Selectionof music
Recentstudieshaveshownthat givingparticipantsa choice
of musiclowersanxiety,promotesrelaxation,and leadsto
effective treatment.14,16,21,22Therefore,a varietyof relax-
ation music was provided by the research team based
on previousstudies. A diverse range of music has been
utilized in researchstudiesto investigateits therapeutic
effectiveness.SomegenresincludeWesternclassic(Bach:
Allemande,Sarabande;Mozart:Romancefrom Eine Kleine
Nachtmusik1; Chopin:Nocturne2), Chineseclassic(Spring
Riverin the Moonlight,Variationon YangPass),andNewAge
(Shizuku,Lordof Wind),andJazz (Everlasting,WinterWon-
derland,In Lovein Vain).All musiccompositionswere soft,
instrumental,slow musicwithout lyrics, of approximately
60—80beats per minute, for 40min duration.16,18 These
characteristicswere in accordancewith the Gaston’sdef-
inition of sedativemusicthat is expectedto evokerelaxing
effectsin the listener.41 Theywereall musiccompositionsof
variousgenreswith relaxationpotential.Participantswere
allowedto select the type of musicto listen to duringthe
studyperiods,from a list of musicprovidedby the research
team, basedon their personalpreferences.Sixparticipants
choseWesternclassic,15 participantschoseChineseclas-
sic, four participantschoseNewAge,andthreeparticipants
choseJazz music.
Statisticalanalysis
Descriptivestatisticswereusedto describethe characteris-
tics of all participantswhosuccessfullycompletedthe study.
Generalizedestimatingequations(GEE)wereusedto exam-
ine the effectsof the interventionon the elders’sleeplevel.
GEEshave becomean importantanalysismethodand are
robustin the analysisof longitudinaldata, in whichpartici-
pantsaremeasuredat differentpointsin time.29 All analyses
were undertakenusingIBMSPSSv20andall statisticaltests
were set at a significancelevel of p <0.05.
Results
Participantcharacteristics
Over the study period, 78 potential participants were
contacted,eight participantsrefusedto participateafter
receivingmoreinformationaboutthe study.Tenparticipants
were disqualifiedbecausenine had baselinePSQI scores
that were below six and one had hearingdifficulties. The
remaining60 participantswere randomlyallocatedinto the
intervention(n =28)andcontrolgroups(n =32)andall com-
pletedthe study(Fig. 1).
controlgroup,datawerecollectedoncea weekfor the same
6 weeks as the interventiongroup, when the researcher
visitedthemat home.
Themusicintervention
The processof musicinterventiontook place in each par-
ticipant’shome.After the randomallocationof participants
to groups,weeklyvisitswere madefor 6 weeksto measure
the sameoutcomes.Six weeksis a recommendedperiodof
time for observingsleep patterns,16,23 and the effects of
a new interventionon sleep quality.14 Participantsin the
experimentalgroupwere providedwith an MP4playerwith
earphonesin order to listen to the music of their choice
from a selection of soft, slow music without lyrics (for
details,pleaseseethe sectionon Selectionof music).Previ-
ous literaturehas shownsubjectiveand scientificevidence
in demonstratingthat music preferenceis a key element
in derivingbeneficialbenefitsfrom music.16,18,36Therefore,
participantswere allowedto choosetheir preferredmusic
and they were requiredto adhereto the use of a single
genreof musicwithin the sameweek, to minimizepossi-
ble variancesin the effect on sleep quality. Participants
were also told to choosethe most comfortableplace to
listen to the music, for examplein their bedroom.Stan-
dardizedinstructionswere givento the participantsas per
a protocol proposedby Chan et al.16 The researcherleft
the participantsalone and stayed a short distanceaway
unobtrusively,so that she or he could be availablefor any
unexpectedresponse.After 40min, the researcherstopped
the music and then collected all outcomesfor each par-
ticipant within a 10—15min conversation.Previousstudies
havesuggestedthat listeningto musiceverydaycontributes
to a better sleep at night, even if it is not consistently
heardat bedtime.16,18,24,36,39
However,to ensureconsistency
in the times for listeningto music, the researchermade
one follow-up phonecall per week after the interviewto
remindparticipantsto listen to the musiconce a day. All
the data collection, includingadministeringthe interven-
tion and collectingthe data, was carried out by the same
researcher.
Thecontrolgroup
Participantsin the controlgroupmet the researcherfor the
samenumberof times as those in the interventiongroup.
Participantsin the control group were given an uninter-
ruptedrest period, but the samedata were collectedonce
a week for 6 weeks.The researchermet them only to col-
lect their sleep quality scores. The researcherrequested
participants,duringthe studyperiod,to not listen to seda-
tive music, but we could not restrict them from listening
to radio or TV. Duringdata collection,the researchermin-
imizedinteractionwith this groupof participants,so as to
reduceresultcontaminationandhenceincreasethe reliabil-
ity of the results.All the data collectionwascarriedout by
the sameresearcher.Everyweek,the researchervisitedthe
participantsandaskedthemwhethertheytookanymedica-
tions to changetheir sleeppatternsand noneof them had
takenanymedications.
Randomization
Two cards were put inside a bag in each draw, with one
labelled as ‘‘intervention’’ and the other as ‘‘control’’.
Each participantwas askedto draw one card from the bag
to allocatehim or her into either the interventionor con-
trol group. There was no blindingas the participantsand
interviewerknewthe allocationgroupsafter randomization.
Selectionof music
Recentstudieshaveshownthat givingparticipantsa choice
of musiclowersanxiety,promotesrelaxation,and leadsto
effective treatment.14,16,21,22Therefore,a varietyof relax-
ation music was provided by the research team based
on previousstudies. A diverse range of music has been
utilized in researchstudiesto investigateits therapeutic
effectiveness.SomegenresincludeWesternclassic(Bach:
Allemande,Sarabande;Mozart:Romancefrom Eine Kleine
Nachtmusik1; Chopin:Nocturne2), Chineseclassic(Spring
Riverin the Moonlight,Variationon YangPass),andNewAge
(Shizuku,Lordof Wind),andJazz (Everlasting,WinterWon-
derland,In Lovein Vain).All musiccompositionswere soft,
instrumental,slow musicwithout lyrics, of approximately
60—80beats per minute, for 40min duration.16,18 These
characteristicswere in accordancewith the Gaston’sdef-
inition of sedativemusicthat is expectedto evokerelaxing
effectsin the listener.41 Theywereall musiccompositionsof
variousgenreswith relaxationpotential.Participantswere
allowedto select the type of musicto listen to duringthe
studyperiods,from a list of musicprovidedby the research
team, basedon their personalpreferences.Sixparticipants
choseWesternclassic,15 participantschoseChineseclas-
sic, four participantschoseNewAge,andthreeparticipants
choseJazz music.
Statisticalanalysis
Descriptivestatisticswereusedto describethe characteris-
tics of all participantswhosuccessfullycompletedthe study.
Generalizedestimatingequations(GEE)wereusedto exam-
ine the effectsof the interventionon the elders’sleeplevel.
GEEshave becomean importantanalysismethodand are
robustin the analysisof longitudinaldata, in whichpartici-
pantsaremeasuredat differentpointsin time.29 All analyses
were undertakenusingIBMSPSSv20andall statisticaltests
were set at a significancelevel of p <0.05.
Results
Participantcharacteristics
Over the study period, 78 potential participants were
contacted,eight participantsrefusedto participateafter
receivingmoreinformationaboutthe study.Tenparticipants
were disqualifiedbecausenine had baselinePSQI scores
that were below six and one had hearingdifficulties. The
remaining60 participantswere randomlyallocatedinto the
intervention(n =28)andcontrolgroups(n =32)andall com-
pletedthe study(Fig. 1).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
52 A. Shumet al.
Assessed for eligibil ity* (n=78)
Excluded (n =18)
Not meet in clusion criteria (n= 10)
Refused to parcipate (n=8)
Other rea sons (n=0)
Analysed (n=28)
Excluded from analysis (n=0)
Lost to follow-up (n =0)
or/and
Disconnu ed interve non (n =0)
Allocated to music (n=28)
Received allocated (n=28)
Did not re ceive allocated (n=0)
Lost to follow-up (n =0)
Or/and
Disconnu ed (n=0)
Allocated to control (n =32)
Received allo cated (n=32)
Did not re ceive allocated (n=0)
Analysed (n=32)
Excluded from analysis (n=0)
Alloca on
Analysis
Follow-Up
Randomizaon
*Screening an d collect baseline info rmao n
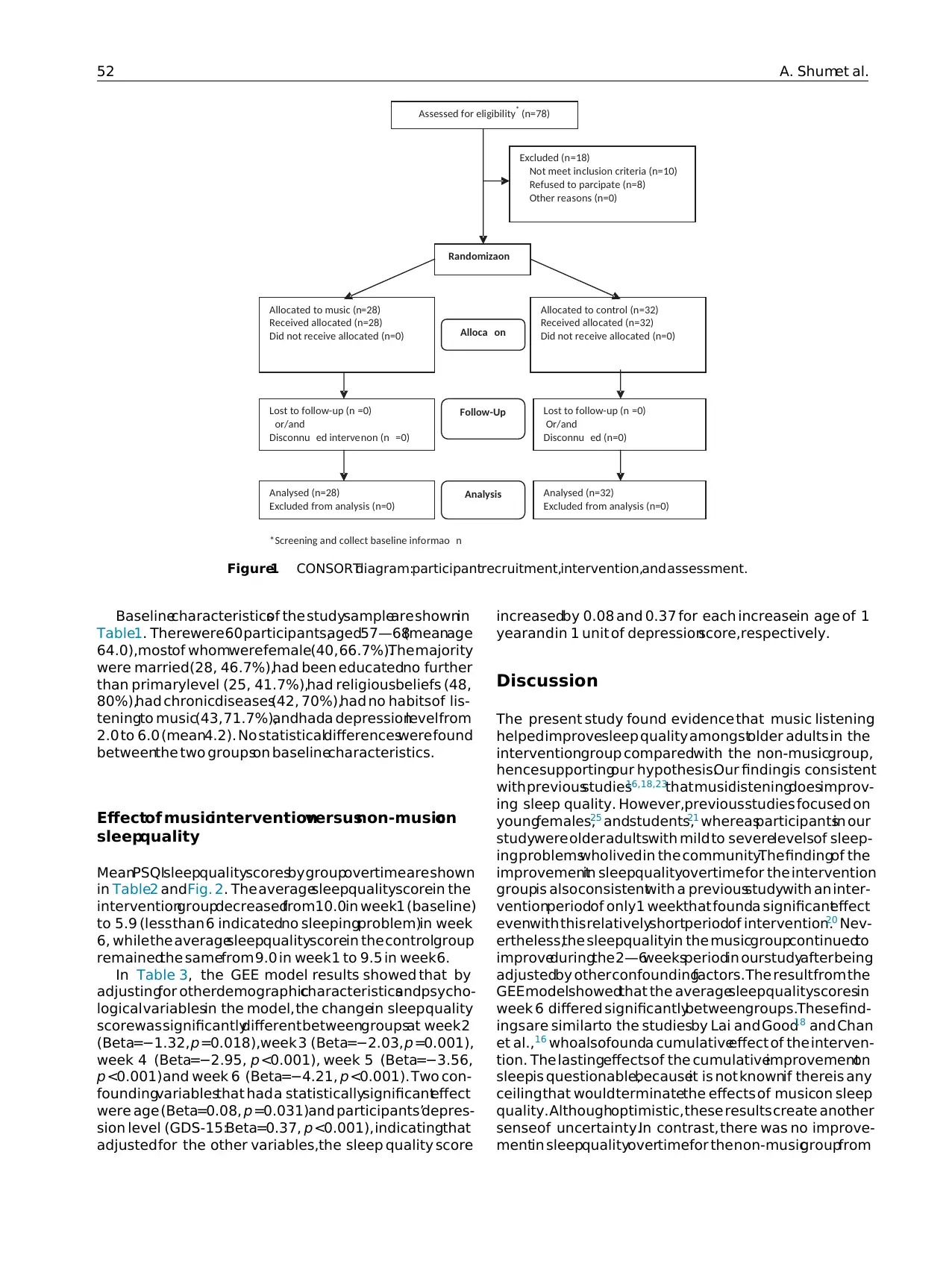
Figure1 CONSORTdiagram:participantrecruitment,intervention,and assessment.
Baselinecharacteristicsof the studysampleare shownin
Table1. Therewere 60 participants,aged57—68(meanage
64.0),mostof whomwerefemale(40, 66.7%).The majority
were married(28, 46.7%),had been educatedno further
than primarylevel (25, 41.7%),had religiousbeliefs (48,
80%),had chronicdiseases(42, 70%),had no habitsof lis-
teningto music(43, 71.7%),andhada depressionlevel from
2.0 to 6.0 (mean4.2). No statisticaldifferenceswere found
betweenthe two groupson baselinecharacteristics.
Effectof musicinterventionversusnon-musicon
sleepquality
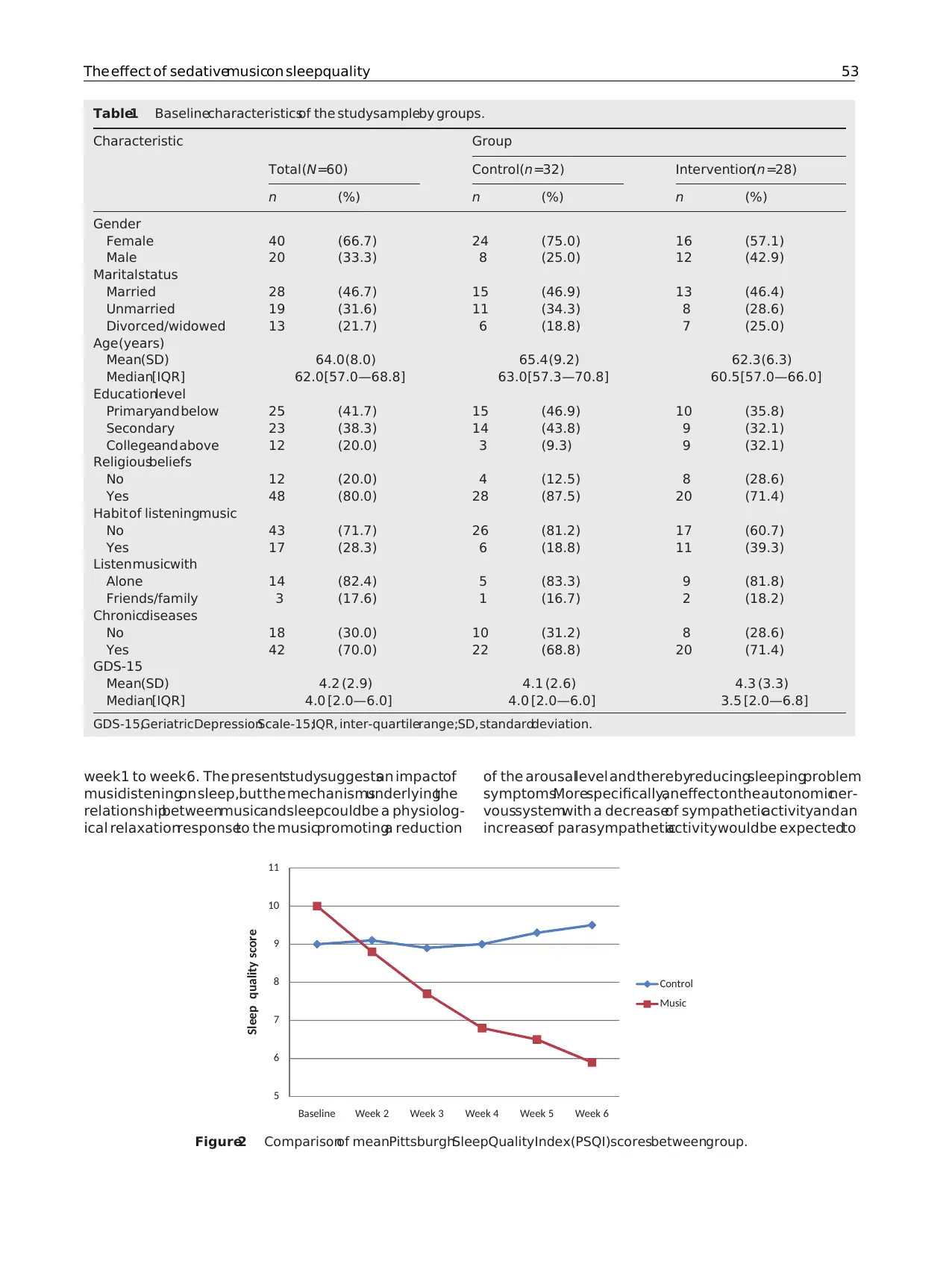
MeanPSQIsleepqualityscoresby groupovertimeare shown
in Table2 andFig. 2. The averagesleepqualityscorein the
interventiongroupdecreasedfrom10.0in week1 (baseline)
to 5.9 (less than 6 indicatedno sleepingproblem)in week
6, whilethe averagesleepqualityscorein the controlgroup
remainedthe samefrom 9.0 in week1 to 9.5 in week6.
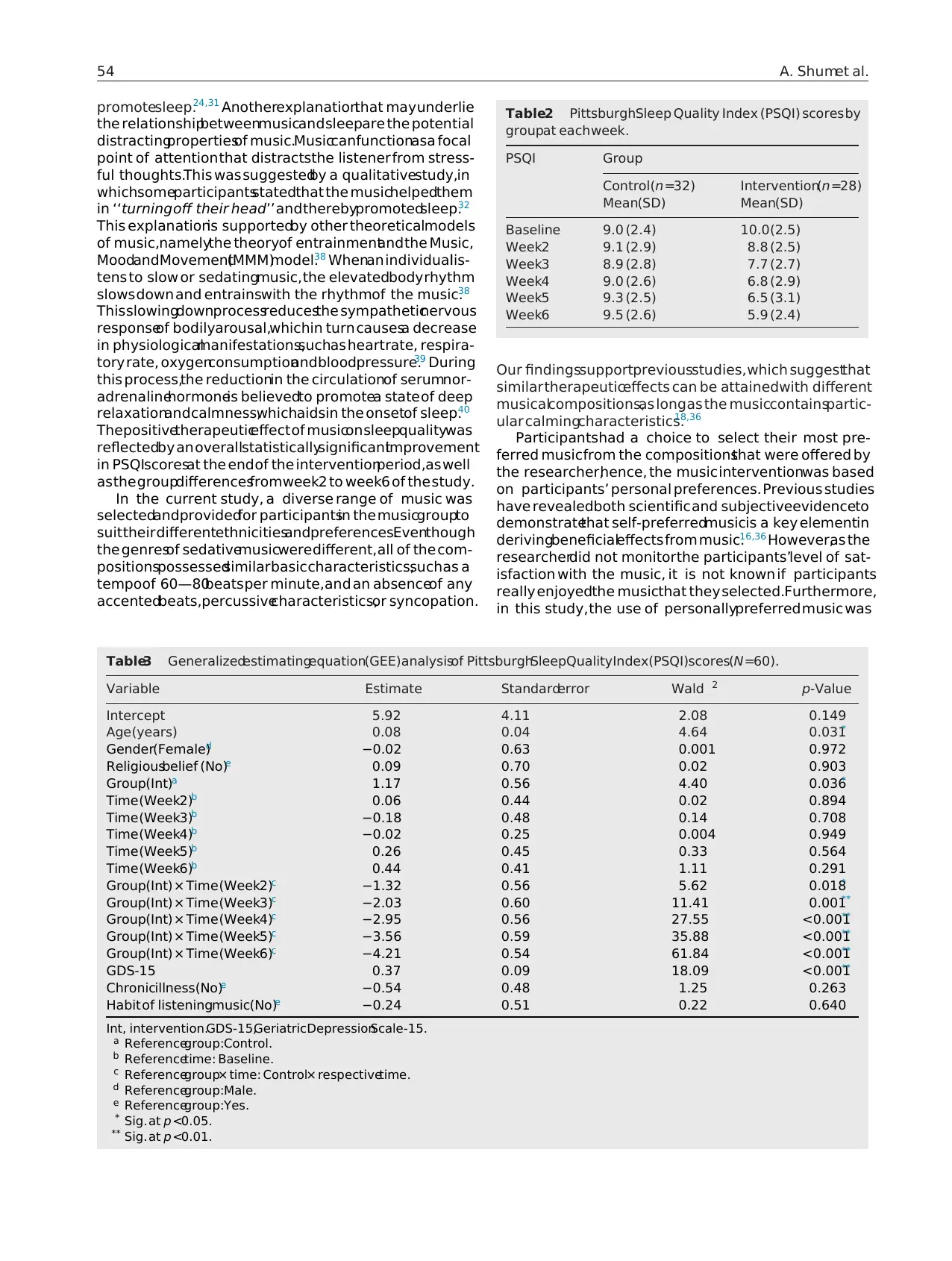
In Table 3, the GEE model results showed that by
adjustingfor otherdemographiccharacteristicsandpsycho-
logical variablesin the model, the changein sleep quality
scorewas significantlydifferent betweengroupsat week2
(Beta=−1.32, p =0.018),week 3 (Beta=−2.03, p =0.001),
week 4 (Beta=−2.95, p <0.001), week 5 (Beta=−3.56,
p <0.001)and week 6 (Beta=−4.21, p <0.001). Two con-
foundingvariablesthat had a statisticallysignificanteffect
were age (Beta=0.08, p =0.031)and participants’depres-
sion level (GDS-15:Beta=0.37, p <0.001), indicatingthat
adjusted for the other variables,the sleep quality score
increasedby 0.08 and 0.37 for each increasein age of 1
yearand in 1 unit of depressionscore,respectively.
Discussion
The present study found evidence that music listening
helped improvesleep quality amongstolder adults in the
interventiongroup comparedwith the non-musicgroup,
hencesupportingour hypothesis.Our findingis consistent
with previousstudies16,18,23
that musiclisteningdoesimprov-
ing sleep quality. However,previousstudies focused on
youngfemales,25 andstudents,21 whereasparticipantsin our
studywere older adultswith mild to severelevelsof sleep-
ing problemswholived in the community.The findingof the
improvementin sleepqualityovertime for the intervention
groupis alsoconsistentwith a previousstudywith an inter-
ventionperiodof only1 weekthat founda significanteffect
evenwith this relativelyshortperiodof intervention.20 Nev-
ertheless,the sleepqualityin the musicgroupcontinuedto
improveduringthe 2—6weeksperiodin ourstudyafter being
adjustedby other confoundingfactors. The resultfrom the
GEE modelshowedthat the averagesleepqualityscoresin
week 6 differed significantlybetweengroups.These find-
ingsare similarto the studiesby Lai and Good18 and Chan
et al.,16 whoalsofounda cumulativeeffect of the interven-
tion. The lastingeffects of the cumulativeimprovementon
sleepis questionable,becauseit is not knownif thereis any
ceilingthat would terminatethe effects of musicon sleep
quality. Althoughoptimistic, these results create another
senseof uncertainty.In contrast, there was no improve-
mentin sleepqualityovertimefor the non-musicgroupfrom
Assessed for eligibil ity* (n=78)
Excluded (n =18)
Not meet in clusion criteria (n= 10)
Refused to parcipate (n=8)
Other rea sons (n=0)
Analysed (n=28)
Excluded from analysis (n=0)
Lost to follow-up (n =0)
or/and
Disconnu ed interve non (n =0)
Allocated to music (n=28)
Received allocated (n=28)
Did not re ceive allocated (n=0)
Lost to follow-up (n =0)
Or/and
Disconnu ed (n=0)
Allocated to control (n =32)
Received allo cated (n=32)
Did not re ceive allocated (n=0)
Analysed (n=32)
Excluded from analysis (n=0)
Alloca on
Analysis
Follow-Up
Randomizaon
*Screening an d collect baseline info rmao n
Figure1 CONSORTdiagram:participantrecruitment,intervention,and assessment.
Baselinecharacteristicsof the studysampleare shownin
Table1. Therewere 60 participants,aged57—68(meanage
64.0),mostof whomwerefemale(40, 66.7%).The majority
were married(28, 46.7%),had been educatedno further
than primarylevel (25, 41.7%),had religiousbeliefs (48,
80%),had chronicdiseases(42, 70%),had no habitsof lis-
teningto music(43, 71.7%),andhada depressionlevel from
2.0 to 6.0 (mean4.2). No statisticaldifferenceswere found
betweenthe two groupson baselinecharacteristics.
Effectof musicinterventionversusnon-musicon
sleepquality
MeanPSQIsleepqualityscoresby groupovertimeare shown
in Table2 andFig. 2. The averagesleepqualityscorein the
interventiongroupdecreasedfrom10.0in week1 (baseline)
to 5.9 (less than 6 indicatedno sleepingproblem)in week
6, whilethe averagesleepqualityscorein the controlgroup
remainedthe samefrom 9.0 in week1 to 9.5 in week6.
In Table 3, the GEE model results showed that by
adjustingfor otherdemographiccharacteristicsandpsycho-
logical variablesin the model, the changein sleep quality
scorewas significantlydifferent betweengroupsat week2
(Beta=−1.32, p =0.018),week 3 (Beta=−2.03, p =0.001),
week 4 (Beta=−2.95, p <0.001), week 5 (Beta=−3.56,
p <0.001)and week 6 (Beta=−4.21, p <0.001). Two con-
foundingvariablesthat had a statisticallysignificanteffect
were age (Beta=0.08, p =0.031)and participants’depres-
sion level (GDS-15:Beta=0.37, p <0.001), indicatingthat
adjusted for the other variables,the sleep quality score
increasedby 0.08 and 0.37 for each increasein age of 1
yearand in 1 unit of depressionscore,respectively.
Discussion
The present study found evidence that music listening
helped improvesleep quality amongstolder adults in the
interventiongroup comparedwith the non-musicgroup,
hencesupportingour hypothesis.Our findingis consistent
with previousstudies16,18,23
that musiclisteningdoesimprov-
ing sleep quality. However,previousstudies focused on
youngfemales,25 andstudents,21 whereasparticipantsin our
studywere older adultswith mild to severelevelsof sleep-
ing problemswholived in the community.The findingof the
improvementin sleepqualityovertime for the intervention
groupis alsoconsistentwith a previousstudywith an inter-
ventionperiodof only1 weekthat founda significanteffect
evenwith this relativelyshortperiodof intervention.20 Nev-
ertheless,the sleepqualityin the musicgroupcontinuedto
improveduringthe 2—6weeksperiodin ourstudyafter being
adjustedby other confoundingfactors. The resultfrom the
GEE modelshowedthat the averagesleepqualityscoresin
week 6 differed significantlybetweengroups.These find-
ingsare similarto the studiesby Lai and Good18 and Chan
et al.,16 whoalsofounda cumulativeeffect of the interven-
tion. The lastingeffects of the cumulativeimprovementon
sleepis questionable,becauseit is not knownif thereis any
ceilingthat would terminatethe effects of musicon sleep
quality. Althoughoptimistic, these results create another
senseof uncertainty.In contrast, there was no improve-
mentin sleepqualityovertimefor the non-musicgroupfrom
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
The effect of sedativemusicon sleepquality 53
Table1 Baselinecharacteristicsof the studysampleby groups.
Characteristic Group
Total (N =60) Control(n =32) Intervention(n =28)
n (%) n (%) n (%)
Gender
Female 40 (66.7) 24 (75.0) 16 (57.1)
Male 20 (33.3) 8 (25.0) 12 (42.9)
Maritalstatus
Married 28 (46.7) 15 (46.9) 13 (46.4)
Unmarried 19 (31.6) 11 (34.3) 8 (28.6)
Divorced/widowed 13 (21.7) 6 (18.8) 7 (25.0)
Age(years)
Mean(SD) 64.0 (8.0) 65.4 (9.2) 62.3 (6.3)
Median[IQR] 62.0[57.0—68.8] 63.0[57.3—70.8] 60.5 [57.0—66.0]
Educationlevel
Primaryand below 25 (41.7) 15 (46.9) 10 (35.8)
Secondary 23 (38.3) 14 (43.8) 9 (32.1)
Collegeand above 12 (20.0) 3 (9.3) 9 (32.1)
Religiousbeliefs
No 12 (20.0) 4 (12.5) 8 (28.6)
Yes 48 (80.0) 28 (87.5) 20 (71.4)
Habit of listeningmusic
No 43 (71.7) 26 (81.2) 17 (60.7)
Yes 17 (28.3) 6 (18.8) 11 (39.3)
Listenmusicwith
Alone 14 (82.4) 5 (83.3) 9 (81.8)
Friends/family 3 (17.6) 1 (16.7) 2 (18.2)
Chronicdiseases
No 18 (30.0) 10 (31.2) 8 (28.6)
Yes 42 (70.0) 22 (68.8) 20 (71.4)
GDS-15
Mean(SD) 4.2 (2.9) 4.1 (2.6) 4.3 (3.3)
Median[IQR] 4.0 [2.0—6.0] 4.0 [2.0—6.0] 3.5 [2.0—6.8]
GDS-15,GeriatricDepressionScale-15;IQR, inter-quartilerange;SD, standarddeviation.
week1 to week6. The presentstudysuggestsan impactof
musiclisteningon sleep,but the mechanismsunderlyingthe
relationshipbetweenmusicandsleepcouldbe a physiolog-
ical relaxationresponseto the musicpromotinga reduction
of the arousallevel and therebyreducingsleepingproblem
symptoms.Morespecifically,aneffect onthe autonomicner-
voussystemwith a decreaseof sympatheticactivityand an
increaseof parasympatheticactivitywouldbe expectedto
5
6
7
8
9
10
11
WeekBaseline Week2 Week3 Week4 Week5 6
Sleep quality score
Control
Music
Figure2 Comparisonof meanPittsburghSleepQualityIndex(PSQI)scoresbetweengroup.
Table1 Baselinecharacteristicsof the studysampleby groups.
Characteristic Group
Total (N =60) Control(n =32) Intervention(n =28)
n (%) n (%) n (%)
Gender
Female 40 (66.7) 24 (75.0) 16 (57.1)
Male 20 (33.3) 8 (25.0) 12 (42.9)
Maritalstatus
Married 28 (46.7) 15 (46.9) 13 (46.4)
Unmarried 19 (31.6) 11 (34.3) 8 (28.6)
Divorced/widowed 13 (21.7) 6 (18.8) 7 (25.0)
Age(years)
Mean(SD) 64.0 (8.0) 65.4 (9.2) 62.3 (6.3)
Median[IQR] 62.0[57.0—68.8] 63.0[57.3—70.8] 60.5 [57.0—66.0]
Educationlevel
Primaryand below 25 (41.7) 15 (46.9) 10 (35.8)
Secondary 23 (38.3) 14 (43.8) 9 (32.1)
Collegeand above 12 (20.0) 3 (9.3) 9 (32.1)
Religiousbeliefs
No 12 (20.0) 4 (12.5) 8 (28.6)
Yes 48 (80.0) 28 (87.5) 20 (71.4)
Habit of listeningmusic
No 43 (71.7) 26 (81.2) 17 (60.7)
Yes 17 (28.3) 6 (18.8) 11 (39.3)
Listenmusicwith
Alone 14 (82.4) 5 (83.3) 9 (81.8)
Friends/family 3 (17.6) 1 (16.7) 2 (18.2)
Chronicdiseases
No 18 (30.0) 10 (31.2) 8 (28.6)
Yes 42 (70.0) 22 (68.8) 20 (71.4)
GDS-15
Mean(SD) 4.2 (2.9) 4.1 (2.6) 4.3 (3.3)
Median[IQR] 4.0 [2.0—6.0] 4.0 [2.0—6.0] 3.5 [2.0—6.8]
GDS-15,GeriatricDepressionScale-15;IQR, inter-quartilerange;SD, standarddeviation.
week1 to week6. The presentstudysuggestsan impactof
musiclisteningon sleep,but the mechanismsunderlyingthe
relationshipbetweenmusicandsleepcouldbe a physiolog-
ical relaxationresponseto the musicpromotinga reduction
of the arousallevel and therebyreducingsleepingproblem
symptoms.Morespecifically,aneffect onthe autonomicner-
voussystemwith a decreaseof sympatheticactivityand an
increaseof parasympatheticactivitywouldbe expectedto
5
6
7
8
9
10
11
WeekBaseline Week2 Week3 Week4 Week5 6
Sleep quality score
Control
Music
Figure2 Comparisonof meanPittsburghSleepQualityIndex(PSQI)scoresbetweengroup.
54 A. Shumet al.
promotesleep.24,31 Anotherexplanationthat may underlie
the relationshipbetweenmusicand sleepare the potential
distractingpropertiesof music.Musiccanfunctionasa focal
point of attention that distractsthe listener from stress-
ful thoughts.This was suggestedby a qualitativestudy,in
whichsomeparticipantsstatedthat the musichelpedthem
in ‘‘turning off their head’’ and therebypromotedsleep.32
This explanationis supportedby other theoreticalmodels
of music,namelythe theoryof entrainmentand the Music,
MoodandMovement(MMM)model.38 Whenan individuallis-
tens to slow or sedatingmusic, the elevatedbody rhythm
slows down and entrainswith the rhythmof the music.38
This slowingdownprocessreducesthe sympatheticnervous
responseof bodilyarousal,whichin turn causesa decrease
in physiologicalmanifestations,suchas heartrate, respira-
tory rate, oxygenconsumptionandbloodpressure.39 During
this process,the reductionin the circulationof serumnor-
adrenalinehormoneis believedto promotea state of deep
relaxationandcalmness,whichaidsin the onsetof sleep.40
Thepositivetherapeuticeffect of musicon sleepqualitywas
reflectedby an overallstatisticallysignificantimprovement
in PSQIscoresat the end of the interventionperiod,as well
as the groupdifferencesfromweek2 to week6 of the study.
In the current study, a diverse range of music was
selectedandprovidedfor participantsin the musicgroupto
suittheir differentethnicitiesandpreferences.Eventhough
the genresof sedativemusicwere different,all of the com-
positionspossessedsimilar basiccharacteristics,such as a
tempoof 60—80beats per minute,and an absenceof any
accentedbeats,percussivecharacteristics,or syncopation.
Table2 PittsburghSleep Quality Index (PSQI) scores by
groupat each week.
PSQI Group
Control(n =32) Intervention(n =28)
Mean(SD) Mean(SD)
Baseline 9.0 (2.4) 10.0(2.5)
Week2 9.1 (2.9) 8.8 (2.5)
Week3 8.9 (2.8) 7.7 (2.7)
Week4 9.0 (2.6) 6.8 (2.9)
Week5 9.3 (2.5) 6.5 (3.1)
Week6 9.5 (2.6) 5.9 (2.4)
Our findingssupportpreviousstudies, which suggestthat
similar therapeuticeffects can be attainedwith different
musicalcompositions,as long as the musiccontainspartic-
ular calmingcharacteristics.18,36
Participantshad a choice to select their most pre-
ferred musicfrom the compositionsthat were offered by
the researcher,hence, the music interventionwas based
on participants’ personal preferences. Previous studies
have revealedboth scientific and subjectiveevidenceto
demonstratethat self-preferredmusicis a key elementin
derivingbeneficialeffects from music.16,36 However,as the
researcherdid not monitorthe participants’level of sat-
isfaction with the music, it is not known if participants
really enjoyedthe musicthat they selected.Furthermore,
in this study, the use of personallypreferred music was
Table3 Generalizedestimatingequation(GEE)analysisof PittsburghSleepQualityIndex(PSQI)scores(N =60).
Variable Estimate Standarderror Wald 2 p-Value
Intercept 5.92 4.11 2.08 0.149
Age (years) 0.08 0.04 4.64 0.031*
Gender(Female)d −0.02 0.63 0.001 0.972
Religiousbelief (No)e 0.09 0.70 0.02 0.903
Group(Int)a 1.17 0.56 4.40 0.036*
Time (Week2)b 0.06 0.44 0.02 0.894
Time (Week3)b −0.18 0.48 0.14 0.708
Time (Week4)b −0.02 0.25 0.004 0.949
Time (Week5)b 0.26 0.45 0.33 0.564
Time (Week6)b 0.44 0.41 1.11 0.291
Group(Int) × Time (Week2)c −1.32 0.56 5.62 0.018*
Group(Int) × Time (Week3)c −2.03 0.60 11.41 0.001**
Group(Int) × Time (Week4)c −2.95 0.56 27.55 <0.001**
Group(Int) × Time (Week5)c −3.56 0.59 35.88 <0.001**
Group(Int) × Time (Week6)c −4.21 0.54 61.84 <0.001**
GDS-15 0.37 0.09 18.09 <0.001**
Chronicillness(No)e −0.54 0.48 1.25 0.263
Habit of listeningmusic(No)e −0.24 0.51 0.22 0.640
Int, intervention.GDS-15,GeriatricDepressionScale-15.
a Referencegroup:Control.
b Referencetime: Baseline.
c Referencegroup× time: Control× respectivetime.
d Referencegroup:Male.
e Referencegroup:Yes.
* Sig. at p <0.05.
** Sig. at p <0.01.
promotesleep.24,31 Anotherexplanationthat may underlie
the relationshipbetweenmusicand sleepare the potential
distractingpropertiesof music.Musiccanfunctionasa focal
point of attention that distractsthe listener from stress-
ful thoughts.This was suggestedby a qualitativestudy,in
whichsomeparticipantsstatedthat the musichelpedthem
in ‘‘turning off their head’’ and therebypromotedsleep.32
This explanationis supportedby other theoreticalmodels
of music,namelythe theoryof entrainmentand the Music,
MoodandMovement(MMM)model.38 Whenan individuallis-
tens to slow or sedatingmusic, the elevatedbody rhythm
slows down and entrainswith the rhythmof the music.38
This slowingdownprocessreducesthe sympatheticnervous
responseof bodilyarousal,whichin turn causesa decrease
in physiologicalmanifestations,suchas heartrate, respira-
tory rate, oxygenconsumptionandbloodpressure.39 During
this process,the reductionin the circulationof serumnor-
adrenalinehormoneis believedto promotea state of deep
relaxationandcalmness,whichaidsin the onsetof sleep.40
Thepositivetherapeuticeffect of musicon sleepqualitywas
reflectedby an overallstatisticallysignificantimprovement
in PSQIscoresat the end of the interventionperiod,as well
as the groupdifferencesfromweek2 to week6 of the study.
In the current study, a diverse range of music was
selectedandprovidedfor participantsin the musicgroupto
suittheir differentethnicitiesandpreferences.Eventhough
the genresof sedativemusicwere different,all of the com-
positionspossessedsimilar basiccharacteristics,such as a
tempoof 60—80beats per minute,and an absenceof any
accentedbeats,percussivecharacteristics,or syncopation.
Table2 PittsburghSleep Quality Index (PSQI) scores by
groupat each week.
PSQI Group
Control(n =32) Intervention(n =28)
Mean(SD) Mean(SD)
Baseline 9.0 (2.4) 10.0(2.5)
Week2 9.1 (2.9) 8.8 (2.5)
Week3 8.9 (2.8) 7.7 (2.7)
Week4 9.0 (2.6) 6.8 (2.9)
Week5 9.3 (2.5) 6.5 (3.1)
Week6 9.5 (2.6) 5.9 (2.4)
Our findingssupportpreviousstudies, which suggestthat
similar therapeuticeffects can be attainedwith different
musicalcompositions,as long as the musiccontainspartic-
ular calmingcharacteristics.18,36
Participantshad a choice to select their most pre-
ferred musicfrom the compositionsthat were offered by
the researcher,hence, the music interventionwas based
on participants’ personal preferences. Previous studies
have revealedboth scientific and subjectiveevidenceto
demonstratethat self-preferredmusicis a key elementin
derivingbeneficialeffects from music.16,36 However,as the
researcherdid not monitorthe participants’level of sat-
isfaction with the music, it is not known if participants
really enjoyedthe musicthat they selected.Furthermore,
in this study, the use of personallypreferred music was
Table3 Generalizedestimatingequation(GEE)analysisof PittsburghSleepQualityIndex(PSQI)scores(N =60).
Variable Estimate Standarderror Wald 2 p-Value
Intercept 5.92 4.11 2.08 0.149
Age (years) 0.08 0.04 4.64 0.031*
Gender(Female)d −0.02 0.63 0.001 0.972
Religiousbelief (No)e 0.09 0.70 0.02 0.903
Group(Int)a 1.17 0.56 4.40 0.036*
Time (Week2)b 0.06 0.44 0.02 0.894
Time (Week3)b −0.18 0.48 0.14 0.708
Time (Week4)b −0.02 0.25 0.004 0.949
Time (Week5)b 0.26 0.45 0.33 0.564
Time (Week6)b 0.44 0.41 1.11 0.291
Group(Int) × Time (Week2)c −1.32 0.56 5.62 0.018*
Group(Int) × Time (Week3)c −2.03 0.60 11.41 0.001**
Group(Int) × Time (Week4)c −2.95 0.56 27.55 <0.001**
Group(Int) × Time (Week5)c −3.56 0.59 35.88 <0.001**
Group(Int) × Time (Week6)c −4.21 0.54 61.84 <0.001**
GDS-15 0.37 0.09 18.09 <0.001**
Chronicillness(No)e −0.54 0.48 1.25 0.263
Habit of listeningmusic(No)e −0.24 0.51 0.22 0.640
Int, intervention.GDS-15,GeriatricDepressionScale-15.
a Referencegroup:Control.
b Referencetime: Baseline.
c Referencegroup× time: Control× respectivetime.
d Referencegroup:Male.
e Referencegroup:Yes.
* Sig. at p <0.05.
** Sig. at p <0.01.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

The effect of sedativemusicon sleepquality 55
not comparedagainst the use of a standardizedset of
researcher-selectedmusic.Therefore,eventhoughpositive
resultswereobtained,theycannotbe usedto concludethat
the use of personallypreferredmusicenhancedthe thera-
peuticeffects on sleepquality.
Anotherinterestingfindingwasthat participants’ageand
depressionscoreswerepositivelycorrelatedwith their sleep
quality. Despitethese two factors being correlated with
sleepquality,theydo not affect the musicintervention.Pre-
viousstudieshavefoundthatin olderpopulationsdepression
maybe relatedto insomnia.31,33Althoughthe musicusedfor
this studywasnot directedspecificallytowardsdepression,
it was able to facilitate stressreductionwhenparticipants
weretryingto sleep.Johnson17 suggestedthat patientswith
insomniamay have multiple causesincludingage, stress,
tension, and anxiety,but the mechanismsunderlyingthe
relationshipbetweenstressand sleepremainunclear.
Strengthensandlimitations
This study has two methodologicalstrengths.Firstly, the
presentstudyhadno attrition.Secondly,the presentstudy’s
researchdesigntakes the form of a RCT that providesa
strongerlevel of evidencethan other researchdesignsas
it helps reduceallocationbias.34 Despitethese strengths,
the study has several limitations. Firstly, the samples
were recruitedin one communitycentre that may induce
selectionbias. Secondly,the samplesizes may affect the
generalizabilityof the findings, althoughthe study was
appropriatelypowered to detect a mediumeffect size.
Thirdly,it wasnot possibleto blindparticipantto the exper-
imentalconditionandthereforeonemusttakeinto account
any Hawthorneeffect, which can influencethe perception
of participantsto rate their sleep quality.To explorethe
possibleplacebo-effectswithin the interventiongroup, a
futurestudycouldbe undertakento includeotherinterven-
tion groups,who listen to the natural environment,or to
other musicthat is pleasantto hear,but doesnot resemble
music with sedativecharacteristics.42 Lastly, becausethe
interventionswere conductedfor 6 weeks,other confound-
ing factors (e.g. whetherall participantsheard the same
amountof music within the intervention),that occurred
duringthe week, mayhaveaffectedparticipants’ratingsof
their sleepquality.Thesevariationsare inevitable,because
any attemptsto controltheseconfoundingvariableswould
havebeenpracticallyimpossibleandunethical.
Conclusions
The present study found evidence that music listening
helped improve sleep quality amongstolder adults. The
findingssuggestthat healthcareprofessionals,with ade-
quatetraining,couldengageelderlyclientsin the processof
musiclisteningtherapy.Not only doesthis processimprove
their sleepingqualityat old age, it also individualizesand
enhancesthe quality of care providedby the healthcare
provideras the therapeuticrelationshipbetweenprovider
andclient is beingestablished.Contemporarygerontologyis
progressivelycharacterizedby collaborationsbetweensev-
eral approacheswith the intent to comprehendboth the
mentaland physicalaspectsof the multifariousprocessof
ageing.Musiclisteningis one suchavenueto alleviatesleep
qualityamongstolder adultsand it makesan essentialcon-
tributionto healthyageing.
Contributors
MFC, AS, and JT designedthe study.AS collectedthe data.
MFCandASanalysedthe data.PreparationwasdonebyMFC,
AS, JT, and BJT.
Conflictof intereststatement
Theauthor(s)declarethat theyhaveno conflictof interests.
References
1. NomuraK, YamaokK, NakaoM, YanoE. Socialdeterminantsof
self-reportedsleepproblemsin SouthKoreaand Taiwan.Jour-
nal of PsychosomaticResearch2010;69(5):435—40.
2. RoepkeSK, Ancol-IsraelS. Sleep disordersin elderly. Indian
Journal of MedicalResearch2010;131:302—10.
3. YeungA, ChangD, GreshamJr R, NierenbergAA, FavaM. Illness
beliefsof depressedChineseAmericanpatientsin primarycare.
Journal of Nervousand Mental Disease2004;192(4):324—7.
4. ZahranHS, KobauR, MoriartyDG, Zack MM, Holt J, Donehoo
R. Health-relatedquality of life surveillance— United States,
1993—2002.Morbidity and Mortality WeeklyReport (MMWR)
SurveillanceSummaries2005;54(4):1—35.
5. BlackwellT, Yaffe K, Ancoli-IsraelS, SchneiderJL, CauleyJA,
Hillier TA, et al. Poorsleepis associatedwith impairedcognitive
function in older women:the studyof osteoporoticfractures.
Journal of Gerontology2006;61:405—10.
6. DamTL, EwingSK, Ancoli-IsraelS, EnsrudK, RedlinesSS,Stone
KL. Associationbetweensleep and physicalfunction in older
men: the osteoporoticfracturesin mansleepstudy.Journal of
AmericanGeriatric Society2008;56:1665—73.
7. Butnik SM. Neurofeedbackin adolescentsand adults with
attentiondeficit hyperactivitydisorder.Journal of Clinical Psy-
chology2005;61(5):621—5.
8. RothT, RoehrsT. Pharamcotherapyfor insomnia.SleepMedicine
Clinics 2010;5(4):529—39.
9. DeMartinisNA, Kamath J, Winokur A. New approachesfor
the treatmentof sleep disorders.Advancesin Pharmacology
2009;57:187—235.
10. BuscemiN, VandermeerB, FriesenC, BialyL, TubmanM, Ospina
M, et al. The efficacyand safetyof drugtreatmentsfor chronic
insomniain adults:a meta-analysisof RCTs.Journal of General
Internal Medicine2007;22(9):1335—50.
11. Kozasa EH, Hachul H, MonsonC, Pinto Jr L, Garcia MC, de
AraujoMoraesMLE,et al. Mind-bodyinterventionsfor the treat-
ment of insomnia:a review. Revista Brasileira de Psquiatria
2010;32(4):437—43.
12. Morin CM, Le Blanc M, Daley M, Gregoire JP, Merette C.
Epidemiologyof insomnia:prevalence,self-help treatments,
consultations, and determinatesof self-seeking behaviors.
SleepMedicine2006;7:123—30.
13. MontgomeryP, DennisJ. Brightlight therapyfor sleepproblems
in adults aged60+.CochraneDatabaseof SystematicReviews
2002;2:145—51.
14. de Niet G, TiemensB, LendemeijerB, HutschemaekersG. Music-
assistedrelaxation to improve sleep quality: meta-analysis.
Journal of AdvancedNursing2009;65(7):1356—64.
15. McCaffrey R. Music listening, its effects in creating a
healing environment. Journal of Psychosocial Nursing
2008;46(10):39—44.
not comparedagainst the use of a standardizedset of
researcher-selectedmusic.Therefore,eventhoughpositive
resultswereobtained,theycannotbe usedto concludethat
the use of personallypreferredmusicenhancedthe thera-
peuticeffects on sleepquality.
Anotherinterestingfindingwasthat participants’ageand
depressionscoreswerepositivelycorrelatedwith their sleep
quality. Despitethese two factors being correlated with
sleepquality,theydo not affect the musicintervention.Pre-
viousstudieshavefoundthatin olderpopulationsdepression
maybe relatedto insomnia.31,33Althoughthe musicusedfor
this studywasnot directedspecificallytowardsdepression,
it was able to facilitate stressreductionwhenparticipants
weretryingto sleep.Johnson17 suggestedthat patientswith
insomniamay have multiple causesincludingage, stress,
tension, and anxiety,but the mechanismsunderlyingthe
relationshipbetweenstressand sleepremainunclear.
Strengthensandlimitations
This study has two methodologicalstrengths.Firstly, the
presentstudyhadno attrition.Secondly,the presentstudy’s
researchdesigntakes the form of a RCT that providesa
strongerlevel of evidencethan other researchdesignsas
it helps reduceallocationbias.34 Despitethese strengths,
the study has several limitations. Firstly, the samples
were recruitedin one communitycentre that may induce
selectionbias. Secondly,the samplesizes may affect the
generalizabilityof the findings, althoughthe study was
appropriatelypowered to detect a mediumeffect size.
Thirdly,it wasnot possibleto blindparticipantto the exper-
imentalconditionandthereforeonemusttakeinto account
any Hawthorneeffect, which can influencethe perception
of participantsto rate their sleep quality.To explorethe
possibleplacebo-effectswithin the interventiongroup, a
futurestudycouldbe undertakento includeotherinterven-
tion groups,who listen to the natural environment,or to
other musicthat is pleasantto hear,but doesnot resemble
music with sedativecharacteristics.42 Lastly, becausethe
interventionswere conductedfor 6 weeks,other confound-
ing factors (e.g. whetherall participantsheard the same
amountof music within the intervention),that occurred
duringthe week, mayhaveaffectedparticipants’ratingsof
their sleepquality.Thesevariationsare inevitable,because
any attemptsto controltheseconfoundingvariableswould
havebeenpracticallyimpossibleandunethical.
Conclusions
The present study found evidence that music listening
helped improve sleep quality amongstolder adults. The
findingssuggestthat healthcareprofessionals,with ade-
quatetraining,couldengageelderlyclientsin the processof
musiclisteningtherapy.Not only doesthis processimprove
their sleepingqualityat old age, it also individualizesand
enhancesthe quality of care providedby the healthcare
provideras the therapeuticrelationshipbetweenprovider
andclient is beingestablished.Contemporarygerontologyis
progressivelycharacterizedby collaborationsbetweensev-
eral approacheswith the intent to comprehendboth the
mentaland physicalaspectsof the multifariousprocessof
ageing.Musiclisteningis one suchavenueto alleviatesleep
qualityamongstolder adultsand it makesan essentialcon-
tributionto healthyageing.
Contributors
MFC, AS, and JT designedthe study.AS collectedthe data.
MFCandASanalysedthe data.PreparationwasdonebyMFC,
AS, JT, and BJT.
Conflictof intereststatement
Theauthor(s)declarethat theyhaveno conflictof interests.
References
1. NomuraK, YamaokK, NakaoM, YanoE. Socialdeterminantsof
self-reportedsleepproblemsin SouthKoreaand Taiwan.Jour-
nal of PsychosomaticResearch2010;69(5):435—40.
2. RoepkeSK, Ancol-IsraelS. Sleep disordersin elderly. Indian
Journal of MedicalResearch2010;131:302—10.
3. YeungA, ChangD, GreshamJr R, NierenbergAA, FavaM. Illness
beliefsof depressedChineseAmericanpatientsin primarycare.
Journal of Nervousand Mental Disease2004;192(4):324—7.
4. ZahranHS, KobauR, MoriartyDG, Zack MM, Holt J, Donehoo
R. Health-relatedquality of life surveillance— United States,
1993—2002.Morbidity and Mortality WeeklyReport (MMWR)
SurveillanceSummaries2005;54(4):1—35.
5. BlackwellT, Yaffe K, Ancoli-IsraelS, SchneiderJL, CauleyJA,
Hillier TA, et al. Poorsleepis associatedwith impairedcognitive
function in older women:the studyof osteoporoticfractures.
Journal of Gerontology2006;61:405—10.
6. DamTL, EwingSK, Ancoli-IsraelS, EnsrudK, RedlinesSS,Stone
KL. Associationbetweensleep and physicalfunction in older
men: the osteoporoticfracturesin mansleepstudy.Journal of
AmericanGeriatric Society2008;56:1665—73.
7. Butnik SM. Neurofeedbackin adolescentsand adults with
attentiondeficit hyperactivitydisorder.Journal of Clinical Psy-
chology2005;61(5):621—5.
8. RothT, RoehrsT. Pharamcotherapyfor insomnia.SleepMedicine
Clinics 2010;5(4):529—39.
9. DeMartinisNA, Kamath J, Winokur A. New approachesfor
the treatmentof sleep disorders.Advancesin Pharmacology
2009;57:187—235.
10. BuscemiN, VandermeerB, FriesenC, BialyL, TubmanM, Ospina
M, et al. The efficacyand safetyof drugtreatmentsfor chronic
insomniain adults:a meta-analysisof RCTs.Journal of General
Internal Medicine2007;22(9):1335—50.
11. Kozasa EH, Hachul H, MonsonC, Pinto Jr L, Garcia MC, de
AraujoMoraesMLE,et al. Mind-bodyinterventionsfor the treat-
ment of insomnia:a review. Revista Brasileira de Psquiatria
2010;32(4):437—43.
12. Morin CM, Le Blanc M, Daley M, Gregoire JP, Merette C.
Epidemiologyof insomnia:prevalence,self-help treatments,
consultations, and determinatesof self-seeking behaviors.
SleepMedicine2006;7:123—30.
13. MontgomeryP, DennisJ. Brightlight therapyfor sleepproblems
in adults aged60+.CochraneDatabaseof SystematicReviews
2002;2:145—51.
14. de Niet G, TiemensB, LendemeijerB, HutschemaekersG. Music-
assistedrelaxation to improve sleep quality: meta-analysis.
Journal of AdvancedNursing2009;65(7):1356—64.
15. McCaffrey R. Music listening, its effects in creating a
healing environment. Journal of Psychosocial Nursing
2008;46(10):39—44.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
56 A. Shumet al.
16. ChanMF, Chan EA, Mok E. Effects of musicon depressionand
sleepqualityon elderly people: a randomizedcontrolledtrial.
ComplementaryTherapiesin Medicine2010;18:150—9.
17. JohnsonJE. The useof musicto promotesleepin older women.
Journal of CommunityHealth Nursing2003;20(1):27—35.
18. Lai HL, Good M. Musicimprovessleep quality in older adults.
Journal of AdvancedNursing2005;49:234—44.
19. Lazic SE, Ogilvie RD. Lack of efficacy of music to improve
sleep:a polysomnographicandquantitativeEEGanalysis.Inter-
nationalJournal of Psychophysiology2007;63:232—9.
20. ZivN, RotemT, ArnonZ, HaimovI. Theeffect of musicrelaxation
versusprogressivemuscularrelaxationon insomniain olderpeo-
ple andtheir relationshipto personalitytraits. Journal of Music
Therapy2008;45(3):360—80.
21. Harmat L, Takacs J, Bodizs R. Music improves sleep qual-
ity in students. Journal of Advanced Nursing 2008;62(3):
327—35.
22. ChangET, Lai HL, Chen PW, Hsieh YM, Lee LH. The effects of
musicon the sleepqualityof adultswith chronicinsomniausing
evidencefrom polysomnographicand self-reportedanalysis:a
randomizedcontrolled trial. InternationalJournal of Nursing
Studies2012;49:921—30.
23. DeshmukhAD, SarvaiyaAA, SeethalakshmiR, Nayak AS. The
effect of Indianclassicalmusicon qualityof sleepin depressed
patients:a randomizedcontrolledtrial. NordicJournal of Music
Therapy2009;18(1):70—8.
24. JespersenKV, VuustP. The effect of relaxationmusiclistening
on sleepqualityin traumatizedrefugees:a pilot study.Journal
of MusicTherapy2012;49(2):205—29.
25. Tan LP. The effects of backgroundmusic on quality of sleep
in elementary school children. Journal of Music Therapy
2004;41(2):128—50.
26. Daniel JB, CharlesFR, TimothyHM, SusanRB, David JK. The
Pittsburgh Sleep Quality Index: a new instrument for psy-
chiatric practice and research.PsychiatryResearch1989;28:
193—213.
27. Elashoff JD. nQuery Advisor 6.01. UK: Statistical Solutions;
2009.
28. YesavageJA, Brink TL, Rose TL. Developmentand validation
of a geriatricdepressionscreeningscale: a preliminaryreport.
Journal of PsychiatricResearch1982;17(1):37—99.
29. MunroBH. Statisticalmethodsfor healthcareresearch.5th ed.
USA: LippincottWilliams& Wilkins; 2005.p. 109—35[Chapter
4].
30. World Health Organization.Definition of an older or elderly
person. Heath Statistics and Health Information System;
2011.Availablefrom: http://www.who.int/healthinfo/survey/
ageingdefnolder/en/[cited 12.08.13].
31. BonnetMH, ArandDL. Hyperarousaland insomnia:state of the
science.SleepMedicineReviews2010;14(1):9—15.
32. MornhinwegGC, VoignierRR. Musicfor sleepdisturbancein the
elderly.Journal of Holistic Nursing1995;13:248—54.
33. GuerreroJ, CrocqM. Sleepdisordersin the elderly: depression
and posttraumaticstress disorder.Journal of Psychosomatic
Research1994;38(Suppl.1):141—50.
34. Joanna BriggsInstitute.Appraiseevidence;2012.http://www.
joannabriggs.edu.au/Appraise%20Evidence[cited 21.03.2012].
35. BuysseDJ, ReynoldsCF, MonkTH, BermanSR, Kupfer DJ. The
PittsburghSleep Quality Index: new instrumentfor psychiatry
practiceand research.Sleep1989;28:193—213.
36. Lai HL. Music preferenceand relaxationin Taiwaneseelderly
people.Journal of Geriatric Nursing2004;25(5):286—91.
37. DeshmukhAD, SarvaiyaAA, Nayak AS. Effect of Indian clas-
sical music on quality of sleep in depressed patients: a
randomizedcontrolledtrial. Nordic Journal of Music Therapy
2009;18(1):70—8.
38. MurrockCJ, HigginsPA. The theoryof music,moodand move-
mentto improvehealthoutcomes.Journal of AdvancedNursing
2009;65(10):2249—57.
39. SchneckDJ, Berger DS. The music effect: music physiology
and clinical applications.London:Jessica KingsleyPublishers;
2006.
40. Bloch B, ReshefA, VadasL, Haliba Y, Ziv N, Kremer I, et al.
The effects of musicrelaxationon sleepqualityand emotional
measuresin peopleliving with schizophrenia.Journal of Music
Therapy2010;47(1):27—52.
41. GastonET. Dynamicmusicfactors in moodchange.MusicEdu-
catorsJournal 1951;37(4):42—4.
42. WampoldBE, MinamiT, TierneySC, BaskinTW, Bhati KS. The
placebo is powerful: estimatingplacebo effects in medicine
and psychotherapyfrom randomizedclinical trials. Journal of
Clinical Psychology2005;61(7):835—54.
16. ChanMF, Chan EA, Mok E. Effects of musicon depressionand
sleepqualityon elderly people: a randomizedcontrolledtrial.
ComplementaryTherapiesin Medicine2010;18:150—9.
17. JohnsonJE. The useof musicto promotesleepin older women.
Journal of CommunityHealth Nursing2003;20(1):27—35.
18. Lai HL, Good M. Musicimprovessleep quality in older adults.
Journal of AdvancedNursing2005;49:234—44.
19. Lazic SE, Ogilvie RD. Lack of efficacy of music to improve
sleep:a polysomnographicandquantitativeEEGanalysis.Inter-
nationalJournal of Psychophysiology2007;63:232—9.
20. ZivN, RotemT, ArnonZ, HaimovI. Theeffect of musicrelaxation
versusprogressivemuscularrelaxationon insomniain olderpeo-
ple andtheir relationshipto personalitytraits. Journal of Music
Therapy2008;45(3):360—80.
21. Harmat L, Takacs J, Bodizs R. Music improves sleep qual-
ity in students. Journal of Advanced Nursing 2008;62(3):
327—35.
22. ChangET, Lai HL, Chen PW, Hsieh YM, Lee LH. The effects of
musicon the sleepqualityof adultswith chronicinsomniausing
evidencefrom polysomnographicand self-reportedanalysis:a
randomizedcontrolled trial. InternationalJournal of Nursing
Studies2012;49:921—30.
23. DeshmukhAD, SarvaiyaAA, SeethalakshmiR, Nayak AS. The
effect of Indianclassicalmusicon qualityof sleepin depressed
patients:a randomizedcontrolledtrial. NordicJournal of Music
Therapy2009;18(1):70—8.
24. JespersenKV, VuustP. The effect of relaxationmusiclistening
on sleepqualityin traumatizedrefugees:a pilot study.Journal
of MusicTherapy2012;49(2):205—29.
25. Tan LP. The effects of backgroundmusic on quality of sleep
in elementary school children. Journal of Music Therapy
2004;41(2):128—50.
26. Daniel JB, CharlesFR, TimothyHM, SusanRB, David JK. The
Pittsburgh Sleep Quality Index: a new instrument for psy-
chiatric practice and research.PsychiatryResearch1989;28:
193—213.
27. Elashoff JD. nQuery Advisor 6.01. UK: Statistical Solutions;
2009.
28. YesavageJA, Brink TL, Rose TL. Developmentand validation
of a geriatricdepressionscreeningscale: a preliminaryreport.
Journal of PsychiatricResearch1982;17(1):37—99.
29. MunroBH. Statisticalmethodsfor healthcareresearch.5th ed.
USA: LippincottWilliams& Wilkins; 2005.p. 109—35[Chapter
4].
30. World Health Organization.Definition of an older or elderly
person. Heath Statistics and Health Information System;
2011.Availablefrom: http://www.who.int/healthinfo/survey/
ageingdefnolder/en/[cited 12.08.13].
31. BonnetMH, ArandDL. Hyperarousaland insomnia:state of the
science.SleepMedicineReviews2010;14(1):9—15.
32. MornhinwegGC, VoignierRR. Musicfor sleepdisturbancein the
elderly.Journal of Holistic Nursing1995;13:248—54.
33. GuerreroJ, CrocqM. Sleepdisordersin the elderly: depression
and posttraumaticstress disorder.Journal of Psychosomatic
Research1994;38(Suppl.1):141—50.
34. Joanna BriggsInstitute.Appraiseevidence;2012.http://www.
joannabriggs.edu.au/Appraise%20Evidence[cited 21.03.2012].
35. BuysseDJ, ReynoldsCF, MonkTH, BermanSR, Kupfer DJ. The
PittsburghSleep Quality Index: new instrumentfor psychiatry
practiceand research.Sleep1989;28:193—213.
36. Lai HL. Music preferenceand relaxationin Taiwaneseelderly
people.Journal of Geriatric Nursing2004;25(5):286—91.
37. DeshmukhAD, SarvaiyaAA, Nayak AS. Effect of Indian clas-
sical music on quality of sleep in depressed patients: a
randomizedcontrolledtrial. Nordic Journal of Music Therapy
2009;18(1):70—8.
38. MurrockCJ, HigginsPA. The theoryof music,moodand move-
mentto improvehealthoutcomes.Journal of AdvancedNursing
2009;65(10):2249—57.
39. SchneckDJ, Berger DS. The music effect: music physiology
and clinical applications.London:Jessica KingsleyPublishers;
2006.
40. Bloch B, ReshefA, VadasL, Haliba Y, Ziv N, Kremer I, et al.
The effects of musicrelaxationon sleepqualityand emotional
measuresin peopleliving with schizophrenia.Journal of Music
Therapy2010;47(1):27—52.
41. GastonET. Dynamicmusicfactors in moodchange.MusicEdu-
catorsJournal 1951;37(4):42—4.
42. WampoldBE, MinamiT, TierneySC, BaskinTW, Bhati KS. The
placebo is powerful: estimatingplacebo effects in medicine
and psychotherapyfrom randomizedclinical trials. Journal of
Clinical Psychology2005;61(7):835—54.
1 out of 8
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.