Analysis of National Safety and Quality Health Service Standard 3
VerifiedAdded on 2022/11/10
|11
|2484
|481
Report
AI Summary
This report provides a critical review of the National Safety and Quality Health Service (NSQHS) Standard 3, which focuses on preventing and controlling healthcare-associated infections (HAIs). The report examines the importance of evidence-based practices, such as hand hygiene and infection control systems, in healthcare settings to improve patient safety and quality of life. It discusses the role of the Australian Guidelines for the Prevention and Control of Infections in Healthcare, the Australian Capital Territory Government, and the Australian Council on Healthcare Standards (ACHS) in ensuring compliance with the standard. The report also highlights the challenges in HAI surveillance, the need for improved data collection, and the importance of accountability in healthcare environments. The report concludes by emphasizing the significance of HAI surveillance programs and the need for national initiatives to improve data reliability and the validation of infection prevention methods. The report also references the accreditation process and the challenges faced by Canberra Hospital in meeting the standards.

Running head: NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 1
A Critical Review of National Safety and Quality Health Service Standard 3
Student’s Name
University
A Critical Review of National Safety and Quality Health Service Standard 3
Student’s Name
University
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 2
A Critical Review of National Safety and Quality Health Service Standard 3
The rise of evidence-based approaches has changed the clinical environment requiring
professionals to follow a certain set of standards in dealing with clinical issues. When standards
are set within a certain industry, then it means that related organizations have to observe
uniformity by all means. In scientific approaches and use of standards, it is important to have a
clear guideline that defines the level of engagement that organizations follow when handling
patient-related issues. Uniformity of care in healthcare institutions can only be achieved if there
is a set of standards that are set to control and manage the healthcare environment by setting a
benchmark that can be used to assess and measure the performance standards of the institution
(Black, Balneaves, Garossino, Puyat, & Qian, 2015). Standards provide levels that customers
expect from healthcare organizations. The outcome of the standards is to provide patient safety
and improve the quality of life in different areas. Healthcare organizations have to be assessed to
determine if they meet the criteria set out as a way of protecting the public from harm. This
means that standards exist to set consistent levels that organizations work along to ensure
consistency and uniformity in healthcare. The National Safety and Quality Health Service
(NSQHS) Standards are used by healthcare organizations to assess their performance by
benchmarking themselves against the standards (Australian Commission on Safety and Quality
in Health Care, 2017). This means that the criteria set are the minimum standard that needs to be
followed by healthcare institutions. This will be reflected in the consistency that will be achieved
when healthcare institutions work with a standard framework that sets a benchmark on what
needs to be done and how it can be achieved. The outcome is public protection from harm and
improved quality of health services.
Standard 3: preventing and controlling healthcare-associated infection
A Critical Review of National Safety and Quality Health Service Standard 3
The rise of evidence-based approaches has changed the clinical environment requiring
professionals to follow a certain set of standards in dealing with clinical issues. When standards
are set within a certain industry, then it means that related organizations have to observe
uniformity by all means. In scientific approaches and use of standards, it is important to have a
clear guideline that defines the level of engagement that organizations follow when handling
patient-related issues. Uniformity of care in healthcare institutions can only be achieved if there
is a set of standards that are set to control and manage the healthcare environment by setting a
benchmark that can be used to assess and measure the performance standards of the institution
(Black, Balneaves, Garossino, Puyat, & Qian, 2015). Standards provide levels that customers
expect from healthcare organizations. The outcome of the standards is to provide patient safety
and improve the quality of life in different areas. Healthcare organizations have to be assessed to
determine if they meet the criteria set out as a way of protecting the public from harm. This
means that standards exist to set consistent levels that organizations work along to ensure
consistency and uniformity in healthcare. The National Safety and Quality Health Service
(NSQHS) Standards are used by healthcare organizations to assess their performance by
benchmarking themselves against the standards (Australian Commission on Safety and Quality
in Health Care, 2017). This means that the criteria set are the minimum standard that needs to be
followed by healthcare institutions. This will be reflected in the consistency that will be achieved
when healthcare institutions work with a standard framework that sets a benchmark on what
needs to be done and how it can be achieved. The outcome is public protection from harm and
improved quality of health services.
Standard 3: preventing and controlling healthcare-associated infection
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 3
The NSQHS third standard of preventing and controlling healthcare-associated infection
applies to the management and control of healthcare-associated infections to increase patient
quality of life and prevent harm. Through infection prevention and control systems, healthcare
organizations are supposed to use evidence-based systems to prevent and control health-related
associations. To achieve this standard, hospital settings must have measures in place for
identifying patients presented to the facility with risk factors for infection of different diseases or
organisms to be identified immediately so that they can receive management and treatment of the
conditions that they have. The Australian Guidelines for the Prevention and Control of Infections
in Healthcare has set guidelines that define evidence-based systems that hospitals are supposed
to comply with. These are hand hygiene, standard and transmission-based precautions, invasive
medical devices, workforce immunization and clean environment, aseptic technique, and
invasive services. This is because different initiatives are used to define how health initiatives
need to be done. For example, hand hygiene needs to be consistent with the National Hand
Hygiene Initiative that is based on the WHO patient safety campaigns that define the way hand
hygiene needs to be carried out.
In the Australian Capital Territory Government, infection and prevention control units
are established in hospitals to minimize the risk of infection for patients, health care providers,
and medical students. This infection control program has several strategies that are used to
ensure that there is compliance with different requirements for hospitals (ACT Government,
2019). This is seen in Canberra Hospital which has established the unit as per the ACT
government requirements. In Infection prevention and control systems, the hospital applies
several strategies to achieve its objective. The first infection prevention strategy is to ensure
compliance with sterilization standards and guidelines like the AS4187 and GENCA which are
The NSQHS third standard of preventing and controlling healthcare-associated infection
applies to the management and control of healthcare-associated infections to increase patient
quality of life and prevent harm. Through infection prevention and control systems, healthcare
organizations are supposed to use evidence-based systems to prevent and control health-related
associations. To achieve this standard, hospital settings must have measures in place for
identifying patients presented to the facility with risk factors for infection of different diseases or
organisms to be identified immediately so that they can receive management and treatment of the
conditions that they have. The Australian Guidelines for the Prevention and Control of Infections
in Healthcare has set guidelines that define evidence-based systems that hospitals are supposed
to comply with. These are hand hygiene, standard and transmission-based precautions, invasive
medical devices, workforce immunization and clean environment, aseptic technique, and
invasive services. This is because different initiatives are used to define how health initiatives
need to be done. For example, hand hygiene needs to be consistent with the National Hand
Hygiene Initiative that is based on the WHO patient safety campaigns that define the way hand
hygiene needs to be carried out.
In the Australian Capital Territory Government, infection and prevention control units
are established in hospitals to minimize the risk of infection for patients, health care providers,
and medical students. This infection control program has several strategies that are used to
ensure that there is compliance with different requirements for hospitals (ACT Government,
2019). This is seen in Canberra Hospital which has established the unit as per the ACT
government requirements. In Infection prevention and control systems, the hospital applies
several strategies to achieve its objective. The first infection prevention strategy is to ensure
compliance with sterilization standards and guidelines like the AS4187 and GENCA which are
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 4
used to prevent clinical infections and at the same time monitoring bloodstream and surgical site
infections (Russo, et al., 2018). Apart from that, the unit is in charge of implementation and
monitoring of hygiene, reducing the emergence of antibiotic-resistant organisms and at the same
time ensuring that infection control guidelines are adhered to within clinical settings. Further, the
unit is supposed to ensure that buildings are renovated and projects designed according to the
required clinical standards like managing the supply of medical equipment to ensure that they
meet the standards established under different medical and clinical standards.
According to the Bedoya, et al. (2017), infection prevention and control practices are a
characteristic of the whole healthcare system and not just an individual healthcare provider. This
implies that the prevention and control of infections are critical in the well-functioning of a
healthcare system. The WHO estimates that around 165,000 Australians contract hospital-related
infections every year which can be prevented (Mitchell, 2017). This challenge has been
attributed to the lack of health-associated infection surveillance which can capture the changes in
the country. This burden is not all about infection but rather some patients die due to these
infections while others are forced to stay longer in hospitals for treatment. In a review
by Mitchell, Shaban, MacBeth, Wood, & Russo (2017) reported that there is limited data on
common infection in Australia due to lack of health surveillance system that can capture and
report.
Stone (2019) adds that having reliable estimate data on health associated infections forms
the basis of prioritization of the prevention and control strategies while at the same time
providing a benchmark for the future. This shows that the existing strategies are limited in the
prevention of infections which call for the need to address the gaps by bringing together different
government bodies which can be important in achieving consensus on prevention approaches and
used to prevent clinical infections and at the same time monitoring bloodstream and surgical site
infections (Russo, et al., 2018). Apart from that, the unit is in charge of implementation and
monitoring of hygiene, reducing the emergence of antibiotic-resistant organisms and at the same
time ensuring that infection control guidelines are adhered to within clinical settings. Further, the
unit is supposed to ensure that buildings are renovated and projects designed according to the
required clinical standards like managing the supply of medical equipment to ensure that they
meet the standards established under different medical and clinical standards.
According to the Bedoya, et al. (2017), infection prevention and control practices are a
characteristic of the whole healthcare system and not just an individual healthcare provider. This
implies that the prevention and control of infections are critical in the well-functioning of a
healthcare system. The WHO estimates that around 165,000 Australians contract hospital-related
infections every year which can be prevented (Mitchell, 2017). This challenge has been
attributed to the lack of health-associated infection surveillance which can capture the changes in
the country. This burden is not all about infection but rather some patients die due to these
infections while others are forced to stay longer in hospitals for treatment. In a review
by Mitchell, Shaban, MacBeth, Wood, & Russo (2017) reported that there is limited data on
common infection in Australia due to lack of health surveillance system that can capture and
report.
Stone (2019) adds that having reliable estimate data on health associated infections forms
the basis of prioritization of the prevention and control strategies while at the same time
providing a benchmark for the future. This shows that the existing strategies are limited in the
prevention of infections which call for the need to address the gaps by bringing together different
government bodies which can be important in achieving consensus on prevention approaches and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 5
surveillance for regular reporting. In addition to the health associated infection programs also
need to be established to capture and report relevant data that can inform recommendations for
research and development. In most cases, the biggest challenge that has been faced is the failure
to enforce accountability within clinical environments as a way of ensuring professional
compliance. This is because low compliance rates in most healthcare situations are regarded as
system or problem failures.
Accreditation plan
The Australian Council on Healthcare Standards (ACHS) is charged with the evaluation,
assessment, and improvement of efficiency, effectiveness, and quality within Australian
hospitals. Each hospital is required to undergo accreditation tests to assess whether it meets the
requirements as set out by the law or not. According to Scott (2018), the March 2018 ACHS
assessment of Canberra hospital revealed that it failed to meet 33 core criteria out of 209, where
two were ranked as extreme risk and six ranked as high. This means that patients attending this
hospital were at the extreme and high risk of health-related challenges. The challenges were
related to fragmentation, lack of cohesion and the failure for the organization to focus on what
was good for the patient and the larger Canberra (White, 2018). The hospital was thus given a
second chance to turn around the 33 core criteria that it failed to meet in March. This means that
the hospital was awarded the accreditation certificate for three years after a second review.
For standard three, the hospital was reported to be compliant with most of the
requirements based on the assessment that was done by ACHS. Since the hospital was accredited
in 2018, it means that it is free to operate for the next two years as they wait for another
accreditation in 2022. This is because the hospital passed all the 42 requirements of standard
three and all the 209 requirement standards after a second review (ACT Health, 2018). The
surveillance for regular reporting. In addition to the health associated infection programs also
need to be established to capture and report relevant data that can inform recommendations for
research and development. In most cases, the biggest challenge that has been faced is the failure
to enforce accountability within clinical environments as a way of ensuring professional
compliance. This is because low compliance rates in most healthcare situations are regarded as
system or problem failures.
Accreditation plan
The Australian Council on Healthcare Standards (ACHS) is charged with the evaluation,
assessment, and improvement of efficiency, effectiveness, and quality within Australian
hospitals. Each hospital is required to undergo accreditation tests to assess whether it meets the
requirements as set out by the law or not. According to Scott (2018), the March 2018 ACHS
assessment of Canberra hospital revealed that it failed to meet 33 core criteria out of 209, where
two were ranked as extreme risk and six ranked as high. This means that patients attending this
hospital were at the extreme and high risk of health-related challenges. The challenges were
related to fragmentation, lack of cohesion and the failure for the organization to focus on what
was good for the patient and the larger Canberra (White, 2018). The hospital was thus given a
second chance to turn around the 33 core criteria that it failed to meet in March. This means that
the hospital was awarded the accreditation certificate for three years after a second review.
For standard three, the hospital was reported to be compliant with most of the
requirements based on the assessment that was done by ACHS. Since the hospital was accredited
in 2018, it means that it is free to operate for the next two years as they wait for another
accreditation in 2022. This is because the hospital passed all the 42 requirements of standard
three and all the 209 requirement standards after a second review (ACT Health, 2018). The
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 6
management of standard three is driven by a small multidisciplinary team which is fragmented
and reports through three streams: the infection d Prevention Service and Central equipment
service report to Clinical Support Service the domestic and environmental service and lastly the
d building maintenance report through to Health Infrastructure. However, the recommendation
after the accreditation review highlighted the need for the hospital to restructure and review how
the health associated infection committee interacts with the top-level management in the
organization and also the need to review the resource allocation model towards the Infection
Prevention and Surveillance Service (IP&S) to maximize quality improvement (ACT Health,
2018).
The operation of the Infection prevention and control systems as established by standard
three is through infection control where risks are identified early and actions implemented
through careful monitoring to ensure vigilance. Despite the fact the hospital has a risk register
number, the hospital needs to have a Gantt chart for addressing the concerns and the use of
policies for dealing with the risk areas. The fact that the hospital failed to meet 33 out 209
standards during the initial assessment means that there is need to focus on the policy areas and
organization risk assessment standards to create the best outcomes for the organization and
ACHS compliance.
Conclusion
Nunez-Nunez, et al. (2017) states that the WHO views Healthcare-associated infection
(HAI) surveillance programs as critical in the prevention of infections and increasing of health
outcomes. These programs enable easy monitoring of outcomes of current practice and reporting
timely feedback that can be used for clinical practice. As a country, Australia lacks a
comprehensive national HAI surveillance program that can be implemented in different
management of standard three is driven by a small multidisciplinary team which is fragmented
and reports through three streams: the infection d Prevention Service and Central equipment
service report to Clinical Support Service the domestic and environmental service and lastly the
d building maintenance report through to Health Infrastructure. However, the recommendation
after the accreditation review highlighted the need for the hospital to restructure and review how
the health associated infection committee interacts with the top-level management in the
organization and also the need to review the resource allocation model towards the Infection
Prevention and Surveillance Service (IP&S) to maximize quality improvement (ACT Health,
2018).
The operation of the Infection prevention and control systems as established by standard
three is through infection control where risks are identified early and actions implemented
through careful monitoring to ensure vigilance. Despite the fact the hospital has a risk register
number, the hospital needs to have a Gantt chart for addressing the concerns and the use of
policies for dealing with the risk areas. The fact that the hospital failed to meet 33 out 209
standards during the initial assessment means that there is need to focus on the policy areas and
organization risk assessment standards to create the best outcomes for the organization and
ACHS compliance.
Conclusion
Nunez-Nunez, et al. (2017) states that the WHO views Healthcare-associated infection
(HAI) surveillance programs as critical in the prevention of infections and increasing of health
outcomes. These programs enable easy monitoring of outcomes of current practice and reporting
timely feedback that can be used for clinical practice. As a country, Australia lacks a
comprehensive national HAI surveillance program that can be implemented in different
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 7
healthcare organizations (Russo, et al., 2018). Although the Australian Commission for Safety
and Quality in Health Care has developed HAI national initiatives, there is a risk of misdirecting
them due to the lack of data that informs the interventions since the government lacks reliable
national HAI data. This calls for the need to develop national initiatives that will lead to reliable
data to be used in the validation of the different infection prevention methods that are adopted.
healthcare organizations (Russo, et al., 2018). Although the Australian Commission for Safety
and Quality in Health Care has developed HAI national initiatives, there is a risk of misdirecting
them due to the lack of data that informs the interventions since the government lacks reliable
national HAI data. This calls for the need to develop national initiatives that will lead to reliable
data to be used in the validation of the different infection prevention methods that are adopted.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 8
References
ACT Government. (2019). Infection Prevention and Control. Retrieved from ACT Government:
https://www.health.act.gov.au/about-our-health-system/accreditation/infection-
prevention-and-control
ACT Health. (2018). Report of the ACHS National Safety and Quality Health Service (NSQHS)
Standards Survey Canberra, ACT . The Australian Council on Healthcare Standard.
Australian Commission on Safety and Quality in Health Care. (2017). National Safety and
Quality Health Service Standards (2nd ed.). Sydney: Australian Commission on Safety
and Quality in Health Care.
Bedoya, G., Dolinger, A., Rogo, K., Mwaura, N., Wafula, F., Coarasa, J., . . . Das, J. (2017).
Observations of infection prevention and control practices in primary health care, Kenya.
Bulletin of the World Health Organization, 95, 503-516.
doi:http://dx.doi.org/10.2471/BLT.16.179499
Black, A. T., Balneaves, L. G., Garossino, C., Puyat, J. H., & Qian, H. (2015). Promoting
Evidence-Based Practice Through a Research Training Program for Point-of-Care
Clinicians. The Journal of Nursing Administration, 45(1), 14–20.
Mitchell, B., Shaban, R. Z., MacBeth, D., Wood, C.-J., & L.Russo, P. (2017). The burden of
healthcare-associated infection in Australian hospitals: A systematic review of the
literature. Infection, Disease & Health, 22(3), 117-128.
doi:https://doi.org/10.1016/j.idh.2017.07.001
Mitchell, B. (2017 , August ). Here’s how many people get infections in Australian hospitals
every year. The Conversation.
References
ACT Government. (2019). Infection Prevention and Control. Retrieved from ACT Government:
https://www.health.act.gov.au/about-our-health-system/accreditation/infection-
prevention-and-control
ACT Health. (2018). Report of the ACHS National Safety and Quality Health Service (NSQHS)
Standards Survey Canberra, ACT . The Australian Council on Healthcare Standard.
Australian Commission on Safety and Quality in Health Care. (2017). National Safety and
Quality Health Service Standards (2nd ed.). Sydney: Australian Commission on Safety
and Quality in Health Care.
Bedoya, G., Dolinger, A., Rogo, K., Mwaura, N., Wafula, F., Coarasa, J., . . . Das, J. (2017).
Observations of infection prevention and control practices in primary health care, Kenya.
Bulletin of the World Health Organization, 95, 503-516.
doi:http://dx.doi.org/10.2471/BLT.16.179499
Black, A. T., Balneaves, L. G., Garossino, C., Puyat, J. H., & Qian, H. (2015). Promoting
Evidence-Based Practice Through a Research Training Program for Point-of-Care
Clinicians. The Journal of Nursing Administration, 45(1), 14–20.
Mitchell, B., Shaban, R. Z., MacBeth, D., Wood, C.-J., & L.Russo, P. (2017). The burden of
healthcare-associated infection in Australian hospitals: A systematic review of the
literature. Infection, Disease & Health, 22(3), 117-128.
doi:https://doi.org/10.1016/j.idh.2017.07.001
Mitchell, B. (2017 , August ). Here’s how many people get infections in Australian hospitals
every year. The Conversation.
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 9
Nunez-Nunez, M., Navarro, M. D., Gkolia, P., Rajendran, N. B., Toro, M. D., Voss, A., . . .
Rodríguez-Bano, J. (2017). Surveillance Systems from Public Health Institutions and
Scientific Societies for Antimicrobial Resistance and Healthcare-Associated Infections in
Europe (SUSPIRE): protocol for a systematic review. BMJ Open, 7.
doi:10.1136/bmjopen-2016-014538
Russo, P. L., Stewardson, A., Cheng, A. C., Bucknall, T., Marimuthu, K., & Mitchell, B. G.
(2018). Establishing the prevalence of healthcare-associated infections in Australian
hospitals: protocol for the Comprehensive Healthcare Associated Infection National
Surveillance (CHAINS) study. BMJ Open , 8. doi:10.1136/bmjopen-2018-024924
Scott, E. (2018, April). Canberra Hospital faces accreditation issues, commits to more than 30
changes. ABC News, pp. 1-7.
Stone, P. W. (2019). Economic burden of healthcare-associated infections: an American
perspective. Expert Review in Pharmacoeconomic Outcomes Research, 9(5), 417–422.
White, D. (2018 , August ). Canberra Hospital accredited for next three years . The Canberra
Times, pp. 1--18.
Nunez-Nunez, M., Navarro, M. D., Gkolia, P., Rajendran, N. B., Toro, M. D., Voss, A., . . .
Rodríguez-Bano, J. (2017). Surveillance Systems from Public Health Institutions and
Scientific Societies for Antimicrobial Resistance and Healthcare-Associated Infections in
Europe (SUSPIRE): protocol for a systematic review. BMJ Open, 7.
doi:10.1136/bmjopen-2016-014538
Russo, P. L., Stewardson, A., Cheng, A. C., Bucknall, T., Marimuthu, K., & Mitchell, B. G.
(2018). Establishing the prevalence of healthcare-associated infections in Australian
hospitals: protocol for the Comprehensive Healthcare Associated Infection National
Surveillance (CHAINS) study. BMJ Open , 8. doi:10.1136/bmjopen-2018-024924
Scott, E. (2018, April). Canberra Hospital faces accreditation issues, commits to more than 30
changes. ABC News, pp. 1-7.
Stone, P. W. (2019). Economic burden of healthcare-associated infections: an American
perspective. Expert Review in Pharmacoeconomic Outcomes Research, 9(5), 417–422.
White, D. (2018 , August ). Canberra Hospital accredited for next three years . The Canberra
Times, pp. 1--18.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 10
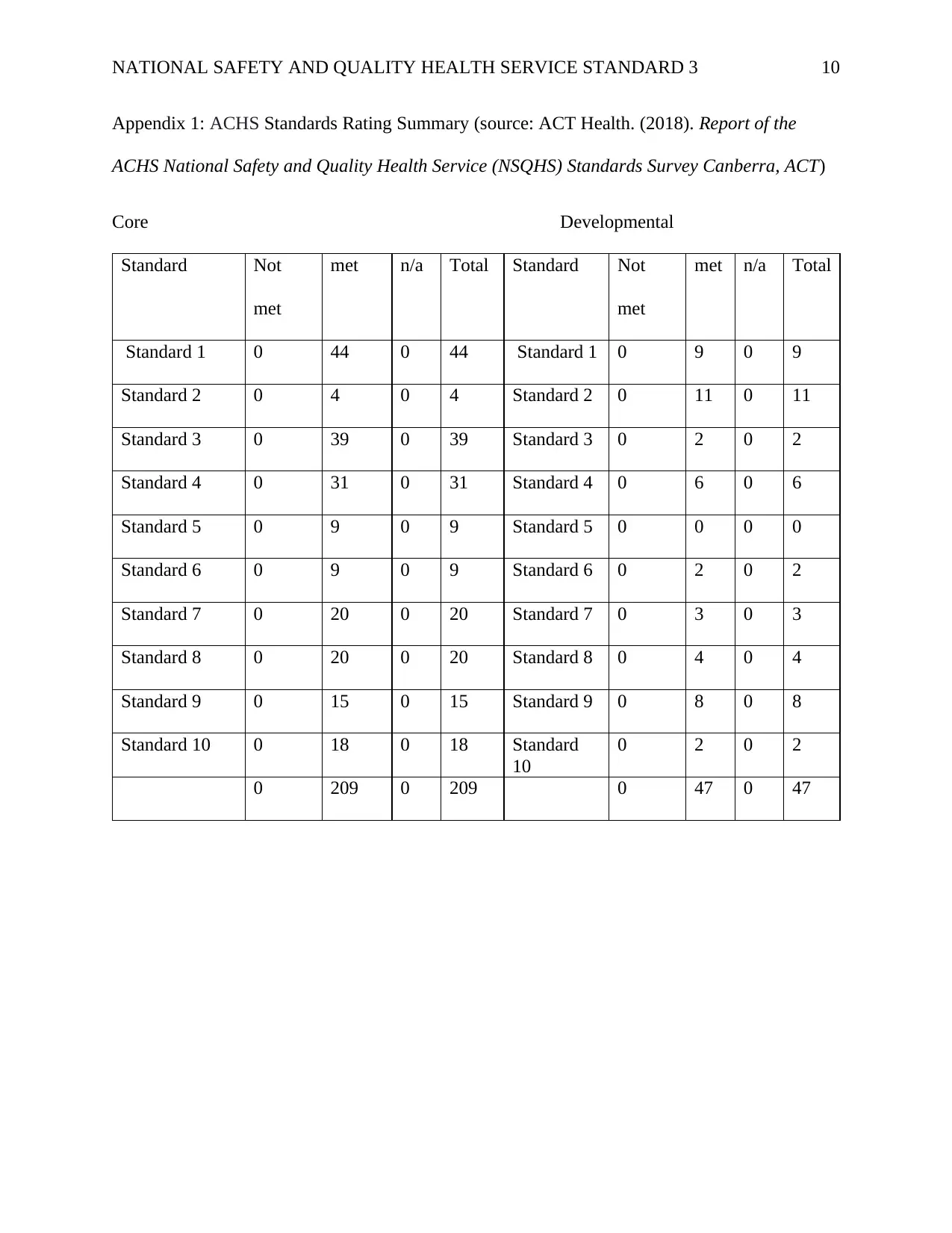
Appendix 1: ACHS Standards Rating Summary (source: ACT Health. (2018). Report of the
ACHS National Safety and Quality Health Service (NSQHS) Standards Survey Canberra, ACT)
Core Developmental
Standard Not
met
met n/a Total Standard Not
met
met n/a Total
Standard 1 0 44 0 44 Standard 1 0 9 0 9
Standard 2 0 4 0 4 Standard 2 0 11 0 11
Standard 3 0 39 0 39 Standard 3 0 2 0 2
Standard 4 0 31 0 31 Standard 4 0 6 0 6
Standard 5 0 9 0 9 Standard 5 0 0 0 0
Standard 6 0 9 0 9 Standard 6 0 2 0 2
Standard 7 0 20 0 20 Standard 7 0 3 0 3
Standard 8 0 20 0 20 Standard 8 0 4 0 4
Standard 9 0 15 0 15 Standard 9 0 8 0 8
Standard 10 0 18 0 18 Standard
10
0 2 0 2
0 209 0 209 0 47 0 47
Appendix 1: ACHS Standards Rating Summary (source: ACT Health. (2018). Report of the
ACHS National Safety and Quality Health Service (NSQHS) Standards Survey Canberra, ACT)
Core Developmental
Standard Not
met
met n/a Total Standard Not
met
met n/a Total
Standard 1 0 44 0 44 Standard 1 0 9 0 9
Standard 2 0 4 0 4 Standard 2 0 11 0 11
Standard 3 0 39 0 39 Standard 3 0 2 0 2
Standard 4 0 31 0 31 Standard 4 0 6 0 6
Standard 5 0 9 0 9 Standard 5 0 0 0 0
Standard 6 0 9 0 9 Standard 6 0 2 0 2
Standard 7 0 20 0 20 Standard 7 0 3 0 3
Standard 8 0 20 0 20 Standard 8 0 4 0 4
Standard 9 0 15 0 15 Standard 9 0 8 0 8
Standard 10 0 18 0 18 Standard
10
0 2 0 2
0 209 0 209 0 47 0 47
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

NATIONAL SAFETY AND QUALITY HEALTH SERVICE STANDARD 3 11
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.